
Manuscript accepted on :24-05-2021
Published online on: 29-05-2021
Plagiarism Check: Yes
Reviewed by: Dr. Michael Jothirajan
Second Review by: Dr. Alamgir Ahmad Dar
Final Approval by: Dr. Francesca Gorini
Dipankar Chakraborty1 , Ranjana S Kale2, Lakshman Das3*, Mousumi Das1 and Sonali Kirde2
, Ranjana S Kale2, Lakshman Das3*, Mousumi Das1 and Sonali Kirde2
1Department of Pharmacology, Agartala Government Medical College, Agartala, Tripura, India.
2Department of Pharmacology, Mahatma Gandhi Institute of Medical Sciences, Sewagram, Wardha, Maharashtra. India.
3Department of Pharmacology, Tripura Medical College and Dr BRAM Teaching Hospital, Hapania, Agartala, Tripura, India.
Corresponding Author's E-mail: doctorldas@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2162
Abstract
The present study has been undertaken to evaluate the pattern of adverse drug reactions (ADRs) of intravenous anticancer (i.v.) drugs with their causality and severity in a tertiary health care set up. The study was an observational cross-sectional survey over a period of 18 months. The indoor patients who were diagnosed to have cancer and receiving i.v. anticancer drugs were included in the study. The details of the patients and ADRs were recorded at the time of visit or within one-month of occurrence of ADRs using case record form and ADR reporting form. A total of 374 patients on cancer chemotherapy were included in the study and ADR was seen in 293(78.34%) patients. Out of total 812 number of ADRs, most ADRs (51.60%) were G.I. system related, followed by skin and appendages related ADRs (23.88%). The association of females in developing haematological ADRs is statistically significant (p<0.05). Most common (19.80%) cause of ADRs was the use of combination of Cisplatin, Paclitaxel and 5 Fluorouracil. Most (90.02%) of the ADRs were categorized as ‘possible’ and the remaining (9.98%) as ‘probable/likely’. The maximum number of the ADRs were classified as ‘mild’(87.68%) followed by moderate (11.45%) and severe (0.86%). The mild reactions were more common as compare to moderate & severe category in G.I & haematology related ADRs (p<0.05).
Keywords
Adverse Drug Reactions; ADRs; Anticancer Drugs; Causality; Pharmacovigilance; Severity
Download this article as:| Copy the following to cite this article: Chakraborty D, Kale R. S, Das L, Das M, Kirde S. Pharmacovigilance Study of Anticancer Drugs in a Tertiary Care Rural Hospital in Central India. Biomed Pharmacol J 2021;14(2). |
| Copy the following to cite this URL: Chakraborty D, Kale R. S, Das L, Das M, Kirde S. Pharmacovigilance Study of Anticancer Drugs in a Tertiary Care Rural Hospital in Central India. Biomed Pharmacol J 2021;14(2). Available from: https://bit.ly/3c29Mh7 |
Introduction
“Cured yesterday of my disease, I died last night of my physician.”
Matthew Prior, from “The Remedy Worse than the Disease” (1714).
The main aim of pharmacovigilance is to reduce the risk of drug related problems to the patient. The information generated by pharmacovigilance is useful in educating doctors about adverse drug reactions (ADRs) and in the official regulation of drug use[1]. A study conducted in USA showed that adverse drug events extended the hospital stay, increased hospitalization cost and increased the risk of death nearly two-fold.[2] In India too, ADRs are increasing and is a great concerned of health, increased hospitalization and cost.[3] One study conducted among patients of Medicine Dept. showed incidence of ADRs 1.8%[4] while another study showed that Incidence of ADRs is 4.75%.[5]
Chemotherapy is a part of the multimodal treatment of cancer, thus allowing for more limited surgery and even cure of formerly incurable cases. [6] Chemotherapy regimens are immensely complex and susceptible to errors.[7] Due to the narrow therapeutic index of anticancer drugs, multiple combinations of drug and the dosage required to achieve a therapeutic response frequently proves toxic to the body’s rapidly proliferating cells.[8]A pharmacovigilance study conducted by Couffignal Al et. al. in a French oncology institute showed that there is a high incidence and economic burden of ADR related to cancer chemotherapy.[9] One study from South India shows that ADRs reported in Oncology Department is the second highest percentage after general medicine.[10]
It is well accepted that anticancer agents are associated with severe adverse effects, decreased the quality of life, and causes an economic burden on patients. No extensive published data is available in Indian population regarding the ADRs of cancer chemotherapy. So, the present study has been undertaken to
Estimate the pattern of ADRs of intravenous(i.v.) anticancer drugs.
Assess the causality of ADRs.
Assess the severity of ADRs.
This study will create a safety profile of anticancer drugs representing central India.
Material and Methods
Study design
The study was planned as a single-centric prospective observational cross-sectional survey.
Setting
This study was conducted in the Department of Pharmacology and Radiotherapy of Mahatma Gandhi Institute of Medical Sciences, Sewagram, Wardha, Maharashtra over a period of 18 months from 1st January 2015 to 30th June 2016.
Study population
The indoor patients who were diagnosed to have cancer and receiving i.v anticancer drugs during the study period.
The following recruitment criteria were used:
Inclusion criteria
Patients diagnosed to have cancer.
Patients receiving i.v. anti-cancer drugs.
Patients of either gender above 18 years of age.
Exclusion criteria:
Patients not willing to give written informed consent.
Patients on concurrent Radiotherapy.
Patients with altered hepatic or renal parameters prior to chemotherapy.
Patients who are taking the alternative system of medicines like Ayurveda, Homeopathy, Unani etc.
Mentally retarded patients.
Drug addicts.
Unconscious and patients unable to respond to verbal questions.
Sampling procedure
Convenience sampling was used to select the study sample.
Sample size
The sample size was calculated by using following formula for cross-sectional study.
Formula: Sample size =
![]()
Where Z= Z value that is 1.96 at 95% confidence interval, p= proportion, q= (1-p), d= α error
Using previous studies knowledge[11], proportion of ADR due to anticancer drug is 41.67%, 95% Confidence Interval with 5% absolute error or precision
In this study, Sample size =

Data Collection
Data were recorded in the Case Record Form. Patient details, chemotherapy details and pattern of ADRs were collected and the data were documented as per study proforma. Haematological and biochemical tests that were performed during chemotherapy as a part of treatment protocol were noted. The details of ADRs which were present at the time of visit or occurred within one-month (to avoid recall bias) were noted in the ADR Reporting Form.
The ADRs encountered in the study population were classified depending on the various body systems involved. Causality was evaluated as per World Health Organization – Uppsala Monitoring Centre causality assessment scale [12].The severity of the ADRs was evaluated by Modified Hartwig and Siegel scale[13,14]
Statistical Analysis
Patient’s details (gender & age), site of malignancy wise distribution, different groups of anticancer drugs prescribed, age-wise & system wise distribution of ADRs, causality & severity of ADRs are represented as percentage. Odds ratio was calculated to assess the relationship between the profile of patient and the system wise ADRs. Statistical significance was determined at 95% level of confidence.
Human subject protection
Approval of the Institutional Ethics Committee was taken before commencing the study. Patients were included in the study after a written, informed consent. Confidentiality of the patient’s identity was maintained.
Results
Characteristics of study population are shown in table-1.
A total of 374 patients on cancer chemotherapy were included in the study. Out of 374 cases 210 (56.15%) were females, 164 (43.85%) were males. Large no. of cases i.e. 121(32.35%) were from 41 to 50 yrs age group followed by 92(24.60%) from 51 to 60 yrs age group. Oral carcinoma was the commonest type found in 124 (33.16%) cases, followed by breast carcinoma (20.32%) and cervical carcinoma (10.70%). A total of 780 no. of anticancer drugs were received by the patients out of which 311 (39.87%) were alkylating agents followed by natural products 266(34.10%). ADR was seen in 293(78.34%) patients, whereas 81(21.66%) cases were without any ADR. Out of 293 patients with ADRs, 168 cases were female and 125 cases were male. Highest number i.e. 92(31.40%) cases with ADR were between 41 to 50 yrs and least number i.e. 20(6.83%) ADR cases were between 18 to 30 yrs of age.
Table 1: Characteristics of study population.
| Characteristics | Categories | No. of patients/drugs (%) | ADR cases (%) |
| Gender | Male | 164(43.85) | 125(42.66) |
| Female | 210 (56.15) | 168(57.34) | |
| Age (years) | 18 to 30 | 22(5.88) | 20(6.83) |
| 31 to 40 | 64(17.11) | 50(17.06) | |
| 41 to 50 | 121(32.35) | 92(31.40) | |
| 51 to 60 | 92(24.60) | 71(24.23) | |
| > 60 | 75(20.05) | 60(20.48) | |
| Site
of malignancy |
Oral | 124 (33.16) | |
| Breast | 76(20.32) | ||
| Cervix | 40(10.70) | ||
| Lungs | 21(5.61) | ||
| Rectum | 18(4.81) | ||
| Larynx | 14(3.74) | ||
| Oesophagus | 13(3.48) | ||
| Colon | 11(2.94) | ||
| Ovary | 9(2.41) | ||
| Testis | 9(2.41) | ||
| NH Lymphoma | 9(2.41) | ||
| Sarcoma | 7(1.87) | ||
| H. Lymphoma | 4(1.07) | ||
| M. Myeloma | 4(1.07) | ||
| Gall Bladder | 4(1.07) | ||
| Occult Primary | 4(1.07) | ||
| Ear | 3(0.80) | ||
| Stomach | 2(0.53) | ||
| Bladder | 2(0.53) | ||
| Groups of anticancer drugs prescribed | Alkylating Agents | 311(39.87) | |
| Natural Products | 266(34.10) | ||
| Antimetabolites | 152(19.49) | ||
| Immunostimulant & Biological Response Modifiers | 36 (4.62) | ||
| Miscellaneous Agents | 8(1.03) | ||
| Hormones and Hormones antagonist | 7(0.90) |
Out of 812 no. of ADRs, most ADRs i.e. 419(51.60%) were G.I. system related, followed by skin and appendages related ADRs [194(23.88%)] and least no. of ADRs i.e. 2(0.25%) were related with cardiovascular system (shown in table-2). The association of female in developing haematological ADRs are statistically significant (p<0.05) .
Table 2: System wise distribution of ADRs.
| System | No. of ADRs | Percentage |
| Gastrointestinal System | ||
| Anorexia | 125 | 15.39% |
| Nausea | 112 | 13.79% |
| Vomiting | 69 | 8.50% |
| Diarrhoea | 40 | 4.93% |
| Constipation | 36 | 4.43% |
| Mouth ulcer | 12 | 1.48% |
| Pain abdomen | 10 | 1.23% |
| Dysphagia | 5 | 0.62% |
| Heart burn | 4 | 0.49% |
| Hematemesis | 3 | 0.37% |
| Halitosis | 2 | 0.25% |
| Hiccup | 1 | 0.12% |
| Total | 419 | 51.60% |
| Skin and Appendages | ||
| Alopecia | 146 | 17.98% |
| Hyperpigmentation | 36 | 4.43% |
| Skin rash | 4 | 0.49% |
| Blackish tongue | 3 | 0.37% |
| Blackish nail | 3 | 0.37% |
| Lips swelling | 1 | 0.12% |
| Thrombophlebitis | 1 | 0.12% |
| Total | 194 | 23.88% |
| Haematology | ||
| Anaemia | 57 | 7.02% |
| Leucopenia | 22 | 2.71% |
| Thrombocytopenia | 17 | 2.09% |
| Total | 96 | 11.82% |
| General | ||
| Weakness | 14 | 1.72% |
| Body ache | 9 | 1.11% |
| Fever | 7 | 0.86% |
| Vertigo | 5 | 0.62% |
| Burning sensation whole body | 4 | 0.49% |
| Generalized oedema | 3 | 0.37% |
| Dryness of mouth | 2 | 0.25% |
| Swelling of legs | 2 | 0.25% |
| Rhinorrhoea | 1 | 0.12% |
| Total | 47 | 5.79% |
| Musculoskeletal System | ||
| Leg cramps | 24 | 2.96% |
| Joint pain | 2 | 0.25% |
| Total | 26 | 3.21% |
| Central Nervous System | ||
| Headache | 10 | 1.23% |
| Sleeplessness | 7 | 0.86% |
| Paraesthesia | 6 | 0.74% |
| Drowsiness | 2 | 0.25% |
| Total | 25 | 3.08% |
| Ocular | ||
| Pain in eyes | 2 | 0.25% |
| Blurring of vision | 1 | 0.12% |
| Total | 3 | 0.37% |
| Cardiovascular System | ||
| Palpitation | 2 | 0.25% |
| Total | 2 | 0.25% |
| Total No. of ADRs | 812 |
Out of 293 patients with ADR, the combination of cisplatin, paclitaxel and 5-fluorouracil caused ADRs in 58(19.80%) patients followed by 51(17.41%) ADR cases caused by cisplatin alone depicted in Fig.1. The association between skin & appendages disorders and combination therapy is very highly significant (p<0.0001). The musculoskeletal ADRs are also significantly (p<0.05) more common with combination therapy.
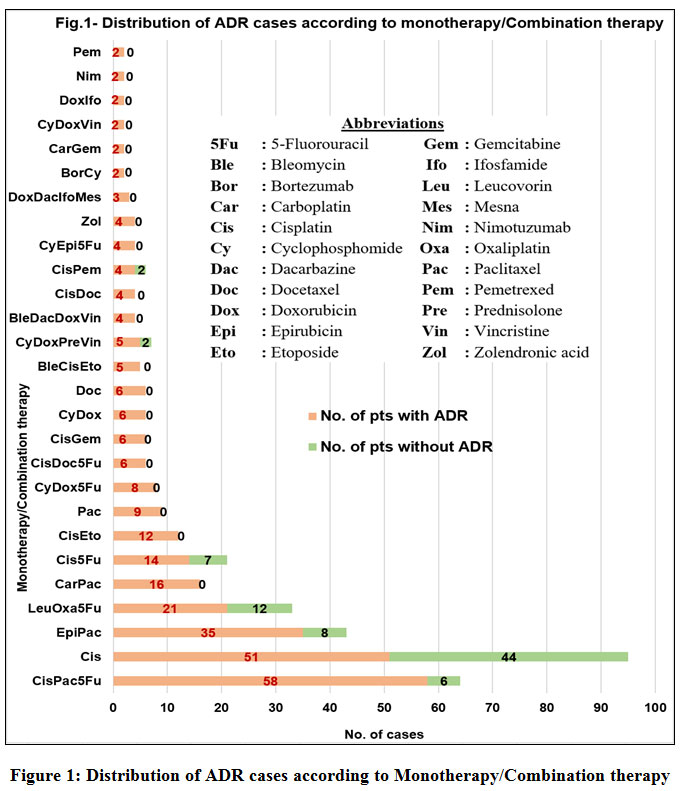 |
Figure 1: Distribution of ADR cases according to Monotherapy/Combination therapy. |
Causality & severity Categories of ADRs are shown in table-3.
Table 3: Causality and severity Categories of ADRs
| Categories | No. of cases (%) | |
|
Causality |
Certain | 0(0.00) |
| Probable/Likely | 81(9.98) | |
| Possible | 731(90.02) | |
| Unlikely | 0(0.00) | |
| Conditional/Unclassified | 0(0.00) | |
| Unassessable/Unclassifiable | 0(0.00) | |
|
Severity |
Mild | 712(87.68) |
| Moderate | 93(11.45) | |
| Severe | 7(0.86) |
731(90.02%) ADRs had been categorized as ‘possible’ whereas the remaining 81(9.98%) ADRs had been categorized as ‘probable/likely’. The association of G.I & haematology related ADRs with the causality (probable & possible) was highly significant (p<0.01). Out of 812 ADRs, most ADRs i.e. 712(87.68%) were found in mild category followed by 93(11.45%) ADRs were in moderate category and 7(0.86%) were in severe category. The mild reactions were more common in G.I & haematology related ADRs as compare to moderate & severe category (p<0.05).(shown in table-4)
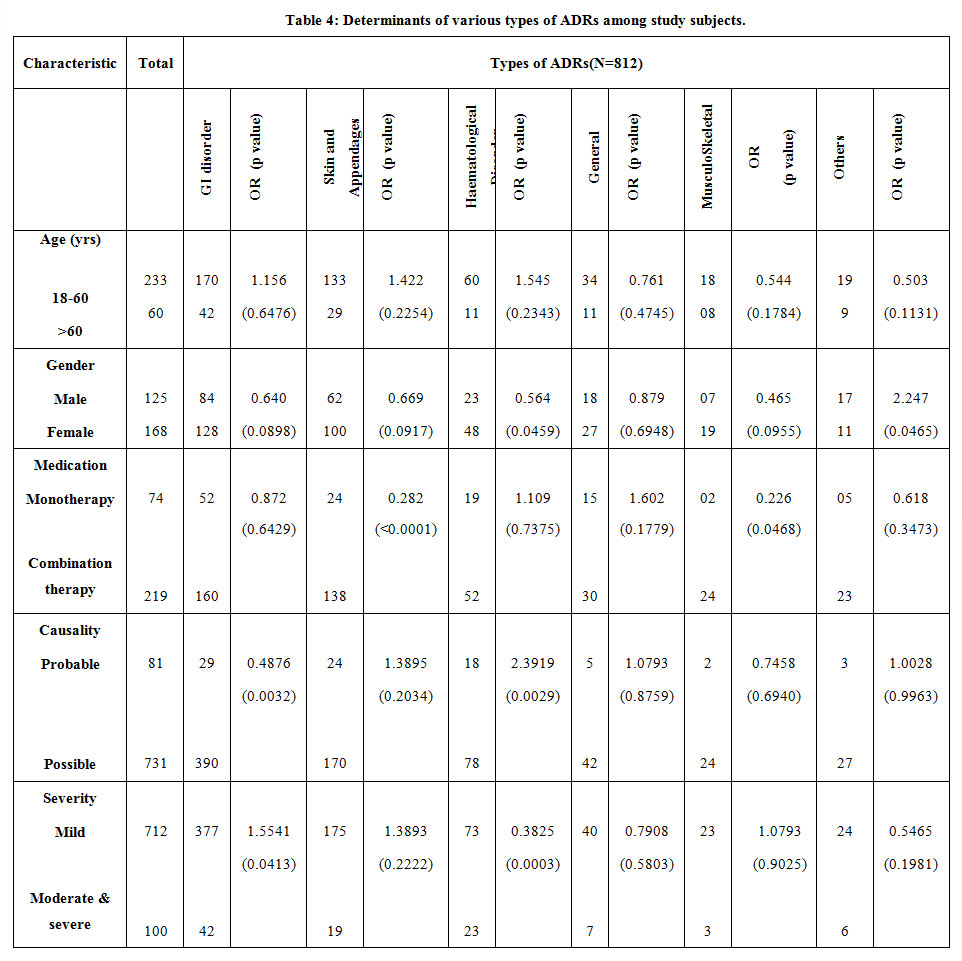 |
Table 4: Determinants of various types of ADRs among study subjects. |
Discussion
ADRs are negative effects of drug therapy which will lead to increased health care costs, increased physician visits, diminished quality of life, hospitalizations, and even death.[14] Jose et al.[10] showed that among all classes of drugs anticancer drugs cause most of ADRs.[10] Over the past few decades, newer anticancer agents have added to the treatment of cancer but simultaneously increased the incidence of ADRs. So, the documentation and reporting of ADRs become an essential element in exploring the side effect profile of a drug. It is possible only by an extensive drug safety monitoring program[15].
Our study shows that oral carcinoma is the commonest(33.16%) type of cancer in central India which correlates with the study findings of Bellare et al.[16] and Rao et al.[17] conducted in South India. As far as prescription of drugs is concerned, alkylating agents were most frequently(39.87%) used anticancer drugs followed by natural products (34.10%). Sharma et al.[18] also found that alkylating agents were mostly used.
In this study, ADRs were found in 78.34% cases which is similar to the finding (70%) of Goyal et al.[19] In contrast to our study, Khandelwal et al.[20] found that only 37.70% cases were suffering from ADRs. We found that out of all ADR cases, females(57.34%) suffered more in comparison with males(42.66%) which is almost similar to the findings (55.9% female) of Sharma et al. [18] In our study, more no. of ADRs (31.40%) were found in between 41 to 50 yrs of age which is comparable (27.4%) to the findings of Chopra et al.[21]. In contrast to our study Mallik et al.[11] found that highest no. of ADR cases (40%) occurred in 61 to 70 yrs group. We found least no. of ADR cases i.e. 6.83% in 18 to 30 yrs group which is similar to the result of Poddar et al.[22] The most commonly affected system by anticancer drugs was G.I. system(51.60%) followed by skin and appendages (23.88%). Similarly Chopra et al.[21] found that highest no. of ADRs were G.I.T. related(43.7%) followed by skin and appendages related(24.9%). On the contrary, Mallik et al.[11] found hematological system to be the most frequently involved followed by G.I.T. In the present study, we have found that haematological ADRs are more common in female. Alopecia was the most common (17.98%) ADR followed by anorexia (15.39%), nausea (13.79%) and vomiting (8.50%). In a similar study by Wahlang et al.[23] also found highest no. of alopecia patients, followed by vomiting, constipation, anorexia. Prasad et al.[22] found nausea and vomiting as most common ADRs, whereas Gunaseelan et al.[24] reported the same as less common.[24] Patients on monotherapy had 74 ADR cases out of which 68.92% cases of ADRs were caused by cisplatin followed by paclitaxel (12.16%). Anorexia, constipation, anemia, leukaemia & weakness were frequently seen in cisplatin treated patients. In a similar study Goyal et al.[19] showed that the most common individual drug responsible for ADR was cisplatin (45%). The combination of cisplatin, paclitaxel and 5-fluorouracil caused maximum number (26.48%) of ADRs followed by the combination of epirubicin and paclitaxel (15.99%). The skin and appendages related ADRs & musculoskeletal ADRs were significantly(p<0.05) associated with combination therapy. Gunaseelan et al.[24] reported that cisplatin was the most common individual drug causing ADRs either alone or in combination. Colon carcinoma was treated by the combination of leucovorin, oxaliplatin and 5 fluorouracil (FOLFOX regimen). The FOLFOX regimen produced lower rates of severe anorexia, anemia, rash and diarrhoea which is comparable with the finding of Goldberg RM et al. [25]
As per WHO-UMC causality assessment, our study revealed that most of the ADRs were under ‘possible’ category (90.02%). The remaining ADRs (9.98%) were under ‘probable’ category. The G.I.T. & haematology related ADRs were significantly (p<0.01) more common under ‘possible’ category. In consistent with our finding Chopra et al.[21] and Bellare et al.[16] revealed that most of the ADRs were “possible” followed by “probable” category. On contrary to our study Amartya De[3] reported 85.28% were probable, 12.88% were possible and about 1.84% were certain ADRs. Most of the chemotherapy in our study was comprised of more than a single drug. Thus, multiple drugs developed a causal link for a ADR. So, most of the causality assessment in our study has been classified as “possible”. Previous studies showed that causality assessment of ADR is a subjective, imprecise and low level of agreement exists between two observers.[26,27] This may be the cause for the difference among various studies. In this study, severity assessment was evaluated by using modified Hartwig and Siegel scale which showed most of the cases were under ‘mild’(87.68%) category followed by ‘moderate’(11.45%) and ‘severe’ (0.86%) category which were comparable with the result of Chopra et al.[21] This shows that ADRs are due to cancer chemotherapy are rarely life threatening with early detection and appropriate pre-medications. The mild reactions were significantly(p<0.05) more common in G.I.T. & haematology related ADRs.
Conclusion
Gastrointestinal system ADRs are the most commonly observed ADRs in cancer chemotherapy. The patients receiving anticancer drugs should be closely monitored for development of any ADR. Pharmacovigilance is an essential tool which can identify the ADRs of cancer chemotherapy by regular monitoring of clinical and laboratory findings. Prompt detection of ADR is important to reduce morbidity and mortality. All ADRs cannot be prevented but their incidence can be decreased by timely use of various medications. There is a high necessity for patient counselling about the therapy and possible ADRs during treatment and also encouraging the treating physicians to report all ADRs irrespective of their severity which can definitely be able to safeguard the health of our population.
Acknowledgement
Authors would like to acknowledge the HOD, Department of Pharmacology and HOD, Department of Radiotherapy, Mahatma Gandhi Institute of Medical Sciences, Sewagram, Wardha, Maharashtra for providing the necessary facilities to carry out this study.
Conflict of interest
There is no conflict of interest in this study.
Funding source
The study received no grants from any funding agency or sectors.
References
- Tripathi KD. Adverse Drug Effects. In: Essentials of Medical Pharmacology. 2019. page 93
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse Drug Events in Hospitalized Patients: Excess Length of Stay, Extra Costs, and Attributable Mortality. Surv Anesthesiol 1998;42(3):130–1.
CrossRef - De A. Monitoring of Suspected Adverse Drug Reactions in Oncology Unit of an Urban Multispeciality Teaching Hospital. Int J Res Pharm Biomed Sci 2010;1(2):1–32.
- Sriram S, Ghasemi A, Ramasamy R, Devi M, Balasubramanian R, Ravi TK, et al. Prevalence of adverse drug reactions at a private tertiary care hospital in south India. J Res Med Sci 2011;16(1):16–25.
- Raut A, Diwan A, Patel C, Patel P, Pawar A. Incidence, severity and financial burden associated with adverse drug reactions in medicine inpatients. Asian J Pharm Clin Res 2011;4(SUPPL. 2):107–11.
- Chabner B. General principles of cancer chemotherapy. In: Brunton L, Chabner B, Knollman B, editors. Goodman & Gillman’s –The pharmacological basis of therapeutics-12th ed. New York: Mc Graw Hill; 2011. page 1667.
- Muller T. Typical medication errors in oncology: Analysis and prevention strategies. Onkologie 2003;26(6):539–44.
CrossRef - Kirthi C, Afzal A, Reddy M, Ali S. A study on the adverse effects of anticancer drugs in an oncology center of a tertiary care hospital. Int J Pharm Pharm Sci 2014;6(2):18–21.
- Couffignal AL, Lapeyre-Mestre M, Bonhomme C, Bugat R, Montastruc JL. Adverse effects of anticancer drugs: apropos of a pharmacovigilance study at a specialized oncology institution. Therapie 2000;55(5):635–41.
- Jose J, Rao PGM. Pattern of adverse drug reactions notified by spontaneous reporting in an Indian tertiary care teaching hospital. Pharmacol Res 2006;54(3):226–33.
CrossRef - Mallik S, Palaian S, Ojha P, Mishra P. Pattern of adverse drug reactions due to cancer chemotherapy in a tertiary care teaching hospital in Nepal. Pak J Pharm Sci 2007;20(3):214–8.
- World Health Organization. The use of the WHO-UMC system for standardized case causality assessment. Uppsala Monit Cent 2005;
- Hartwig SC, Siegel J, Schneider PJ. Preventability and severity assessment in reporting adverse drug reactions. Am J Heal Pharm 1992;49(9):2229–32.
CrossRef - Kumar S, State T. A prospective observational study on monitoring , evaluating and reporting of adrs in a tertiary care hospital. World J Pharm Pharm Sci 2016;5(2):736–52.
- World Health Organization. International drug monitoring: the role of the hospital, report of a WHO meeting [held in Geneva from 18 to 23 November 1968]. Geneva: World Health Organization; 1969.
- Bellare PS, Ashwin K, PU SP, Vinaykumar S, Rakesh K. B.1. A Retrospective Evaluation of Adverse Drug Reactions Due to Cancer Chemotherapy in a Tertiary Care Hospital in South India. J Young Pharm 2016;8(3):251–4.
CrossRef - Rao AY, Rasala NY, Mandarapu RK, Pakeerupalli B, Puchchakayala G. Adverse Effects of Anticancer Drugs in A Tertiary Care Hospital in South India. IOSR J Dent Med Sci 2016;15(6):129–33.
- Sharma A, Thomas J, Bairy K, Kumari Km, Manohar H. Pattern of adverse drug reactions due to cancer chemotherapy in a tertiary care hospital in South India. Perspect Clin Res 2015;6(2):109.
CrossRef - Goyal YN, College PDUM, Govt MPS. Pattern of Adverse Drug Reactions Due to Cancer Chemotherapy in Tertiary Care Teaching Hospital in Gujarat. Int J Sci Res 2014;3(1):333–5.
CrossRef - Khandelwal S, Bairy KL, Vidyasagar MS, Chogtu B, Sharan K. Adverse drug reaction profile of cancer patients on chemotherapy in a tertiary care hospital. Int J Pharma Bio Sci 2015;6(2):233–44.
- Chopra D, Rehan HS, Sharma V, Mishra R. Chemotherapy-induced adverse drug reactions in oncology patients: A prospective observational survey. Indian J Med Paediatr Oncol 2016;37(1):42–6.
CrossRef - Poddar S, Sultana R. Pattern of adverse drug reactions due to cancer chemotherapy in tertiary care teaching hospital in Bangladesh. Dhaka Univ 2009;8(1):11–6.
CrossRef - Wahlang JB, Laishram PD, Brahma DK, Sarkar C, Lahon J, Nongkynrih BS. Adverse drug reactions due to cancer chemotherapy in a tertiary care teaching hospital. Ther Adv Drug Saf 2016;1–6.
CrossRef - Gunaseelan V, Mandal SK, VN P, Khumukcham R, Devi K, Pramodini K, et al. Adverse drug reactions to cancer chemotherapy in a regional cancer center in northeast india. Int J Pharm Sci Res 2014;5(8):3358–63.
- Goldberg RM, Sargent DJ, Morton RF, Fuchs CS, Ramanathan RK, Williamson SK, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol 2004;22(1):23–30.
CrossRef - Belhekar MN, Taur SR, Munshi RP. A study of agreement between the Naranjo algorithm and WHO-UMC criteria for causality assessment of adverse drug reactions. Indian J Pharmacol 2014;46(1):117.
CrossRef - Blanc S, Leuenberger P, Berger J-P, Brooke EM, Schelling J-L. Judgments of trained observers on adverse drug reactions. Clin Pharmacol Ther 1979;25(5):493–8.
CrossRef

