
Manuscript accepted on :24-05-2021
Published online on: 11-06-2021
Plagiarism Check: Yes
Reviewed by: Dr. Salman Ahmed Pharmacognosy
Second Review by: Dr. Mohammad Barary
Final Approval by: Dr. Ian James Martin
Tasneem H. Ali Fathi1 and Shaima Ali Miraj2*
1Department of Public Health, College of Health Sciences, Saudi Electronic University, Riyadh, Kingdom of Saudi Arabia, Clinical Laboratory Department of Pathology and Lab Medicine King Saud University Medical City King Khalid University Hospital Riyadh Saudi Arabia
2Department of Public Health, College of Health Sciences Saudi Electronic University, Riyadh 11673Saudi Arabia.
Corresponding Author E-mail: shaima.s.ali@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2183
Abstract
Background: The current study was premeditated to evaluate the attitude, knowledge and practice of the pharmacy employees (including interns and trainees) dealing with medical practice towards medical errors and adverse drug reaction reports. Methods:The study is a quantitative, descriptive, cross-sectional one with the influence of medication-error reporting, focused on pharmacy department of King Saud University Medical City, Riyadh, Saudi Arabia using the Likert-scale survey. The research population was 167 pharmacy employees, (including interns, and trainees) from King Saud University Medical City. The legalized items connected to knowledge, attitude and practices (KAP) survey was given to each member. Results:Majority of the total sample size (n=167) are pharmacists, managers, lead pharmacists, pharmacist-in-charge, or staff pharmacist by 74.3 %, where 15.6 % are pharmacy technicians, 7.8 % are pharmacy students interns/externs and 2.4 % other workers. Positive responses were highest in teamwork within the pharmacy employee (87.3% vs. 81.6%), staff training and skills within the pharmacy employee (86.35% vs. 79.25%), physical space and environment in the pharmacy (83.8% vs. 73.6%). Lower responses were found in response to mistakes (79.75% vs. 74.4%) compared to community pharmacy database report (AHRQ, 2019).Conclusion:The findings indicate that ratings on documenting mistakes (reporting)as perceived by pharmacy employee are at par with the community pharmacy elsewhere. The weakest dimension identified was mistakes (reporting) having the lowest positive response with a mean score of 3. This denotes a low level of agreement according to Likert scale confirming that is the dimension needing improvement.
Keywords
Attitude; Improvement; Knowledge; Medication Errors; Practice; Pharmacy; Safety
Download this article as:| Copy the following to cite this article: Fathi T. H. A, Miraj S. A. Impact of Knowledge, Attitude and Practice on Medication errors and Safety Improvement in Pharmacy Departments of King Saud University Medical City Riyadh Saudi Arabia. Biomed Pharmacol J 2021;14(2). |
| Copy the following to cite this URL: Fathi T. H. A, Miraj S. A. Impact of Knowledge, Attitude and Practice on Medication errors and Safety Improvement in Pharmacy Departments of King Saud University Medical City Riyadh Saudi Arabia. Biomed Pharmacol J 2021;14(2). Available from: https://bit.ly/2TQ1z9g |
Introduction
Poor patient safety in health systems through medical error reporting is the third most common cause of death globally, behind cardiovascular diseases and cancer, it is a reversible action as being the main responsibility of the health care provider for the patient safety, and can be rectified and avoided. The healthcare organizations need to encourage reporting of the medical related errors and implement clear policies and guidelines which can encourage the healthcare provider to safeguard the interest of the patients. The safety system needs not just to be in place, but to be successful.1,2,3,4,5 Recently Ahmed6 et al., have reported that the common medical errors result from incomplete instructions, incorrect dosage, and incorrect route of administration, diagnosis errors, and labelling errors. The perceived causes of these medical errors include high workload, lack of support systems, stress, medical negligence, inadequate training, miscommunication, poor collaboration, and non-adherence to safety guidelines among the healthcare professionals based on a study conducted in a Kuwait tertiary hospital. A similar work has reported seven perceived reasons for medical errors, namely system reason, nurses’ staffing, physician communication, medication packaging, transcription, and pharmacy process. The study recommended the development of active quality assurance systems in all health care environments, concerning medications and drug administration4.
Medication errors occur broadly on various steps that includes dispensing, transcribing, prescribing and administration. It has decreased due to use of computerized physician order administration than hand written prescription (HWP). Numerous approaches have been suggested in detection and of the occurrence of medical errors and the way of reducing it. Adverse drug reaction is the common approach used and mostly employed in high risk industries such as hospitals.7,8Alsulami9 et al., Hammoudi10 et al., and Alshahrani 11 et al., have surveyed information, frames of mind and practices towards the detailing of prescription mistakes among wellbeing professionals at some hospitals of Saudi Arabia to find remedies to ward off such medical errors. The investigations led by Stewart12 et al., planned to measure and disclose conduct determinants identifying with errors announcing of human services experts in Qatar, as a premise of creating intercessions to upgrade the adequacy and proficiency of mistake revealing. Quantitative results showed that while these were issues for all medicinal services experts, thosemore youthful and less experienced were generally concerned.
George13 et al., created mediations to decrease level of patients with at least one medicine error during release. A drug specialist drove quality improvement (QI) program more than a half year directed in medicinal wards at a tertiary open emergency clinic. With the usage of the QI program, the level of patients with at least one prescription error during release that was remedied by drug specialists fundamentally expanded from 77.6% to 95.9%. Assiri14 et al., utilized electronic wellbeing record information. Many studies have investigated the burden of medical errors in healthcare systems throughout the world15, which significantly increase treatment costs and hospitalization periods, aside from increasing patient rates of mortality and morbidity in some situations16. However, there is insufficient data about medical error reporting and actions taken thereof, in Saudi Arabia, and in Middle Eastern countries generally. One report indicates that there were 1,356 cases reported in 201317, but the true prevalence is undoubtedly far higher than the number of reported instances.18
It is essential to understand the difficulties associated with disclosing medical error mishaps in Saudi Arabia in order to avoid other potential errors and near misses that could adversely affect patients. This study helps filling this gap in knowledge and contributes towards professional discourse and policy decisionmaking to improve medication safety in King Saud University Medical City (KSUMC) based in the Capital of Saudi Arabia, Riyadh. It is one of the largest university medical cities around the Kingdom. The objective of the present research was to assess the current status of the medication error reporting programand evaluate the cultural impact of patient safety initiatives and interventions.It also addresses toidentify the strengths and weakness areas forpatient safety culture improvement in a bid to raise the staff awareness about the patient and medication safety.
Material and Methods
Study Design and Setting
The observational cross-sectional study was conducted to assess the knowledge, attitude and practices about medication errors and patient safety among the pharmacy professionals in King Saud University Medical City, (KSUMC), Riyadh, Saudi Arabia. Necessary Ethical approval was obtained from the Institutional review board (IRB) Ref. No. 19/0143/14RB. The data were collected between December 2019 and March 2020.The inclusion criteria included those who were available and willing to participate were approached and asked to fill out questionnaires whereas the exclusion criteria included those individuals who couldn’t complete the questionnaire for any reasonThe community pharmacy survey questionnaire, adapted from AHRQ, USA wasdistributed to the participating pharmacists and clinical pharmacists and were requested to complete the 5 point Likert-scale survey, ranging from ‘strongly disagree’ to `strongly agree’. Thequestionnaire consisted of 2 sections namely demographic characteristicswhereas the second section included 4 parts with a total of 38 questions with a total of working in pharmacy department, ccommunication and work pace, patient safety and response to mistakes as well as documenting mistakes. Before executing the actual study, necessary piloting was doneon 60 community pharmacists with Reliabilitystatistics(Cronbach’s alpha = 0.86) suggesting a good internal consistency.A total of 496 staffusing convenient samplingwas used for the selection of participants. The actual sample size estimated was 150 usingthe Thompson equationwith an error margin of 5%,95% confidence interval and aresponse distribution of 50%(19) . The actual cohort which participated in the study was167.We assured the respondents that anonymity and confidentiality will be upheldduring the entire process.
Statistical analysis: SPSS version 22 was used to evaluate the results (IBM Corp., Armonk, NY, USA). A statistically relevant value of p < 0.05 was calculated. The categorical variables were evaluated with the Chi-square test.
Results and Discussion
A total of 167 pharmacists from the King Saud University Medical City in Riyadh participated in the study with a response rate of 99%. The demographic data was represented in Table 1,showing working characteristics of the respondents in terms of years of work in pharmacy department, number of working hours/week and their work position/designation. The data showed that15 %of the respondents worked for less than 6 months, whereas 5.4 % worked for more than 6 months and less than 1 year. Similarly, 17.4 % worked from 1-3 years, 32.3 % worked between 3-6 years, 16.2 % between 6-12 years, finally 13.8 % worked for 12 and more years. In terms of working hours, 6 % out of the total sample size (n=167) worked at most 16 hours per week, 3 % from 17 to 31 hours, 78.4 % from 32 to 40 hour per week, and finally 12.6 % for more than 40 hours. In terms of working position, majority of the total sample (n=124), 74.3% were Pharmacist, managers, lead pharmacists, pharmacist-in-charge, or staff pharmacists where 15.6 % are Pharmacy technician, 7.8 % are Pharmacy student intern/extern, and finally 2.4 % other workers. ThePharmacists perception on the different dimensions that influence patient safety cultureused to describe the basic features of the collected data in each dimension, such as frequencies, percentages, mean, standard and deviation(Table 2,3,4 and 5).This 5-point Likert scale measure were used to answer the items in each dimension, that ranged from [1] strongly disagree or [Never] up to [5] strongly agree or [Always].The mean Likert scale was calculated to determine the overall score of the dimension that gauges the respondents’ level of agreement to the dimension.
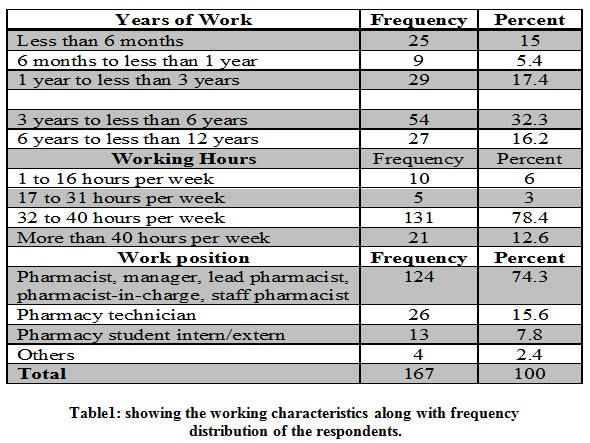 |
Table 1: showing the working characteristics along with frequency distribution of the respondents. |
A positive response rate of 86.05%, 26.78%, 75.5% and 45.56% respectively were recorded for the four variables under study.
Working in Pharmacy
The total factor mean was 3.81 ± 0.597 with the highest meanbeen reported as 3.86 for the four statements whereas the lowest mean was 3.7 ± 0.775 for the fifth statement. Similarly, apositive response rate of (86.05%) with a mean score of 3.81±0.597was reported indicating that the factor is above medium values(Table 2).
Table 2: Working in the Pharmacy Factor by Mean and Standard deviation for each Statement.
| Working in the Pharmacy | Strongly Disagree | Disagree | Neither | Agree | Strongly Agree | Mean | S.D |
| This pharmacy is well organized | 6 | 6 | 13 | 131 | 9 | 3.79 | 0.753 |
| 3.6 | 3.6 | 7.9 | 79.4 | 5.5 | |||
| Staff treat each other with respect | 6 | 4 | 10 | 135 | 12 | 3.86 | 0.73 |
| 3.6 | 2.4 | 6 | 80.8 | 7.2 | |||
| Technicians in this pharmacy receive the training they need to do their jobs | 5 | 10 | 11 | 133 | 6 | 3.76 | 0.75 |
| 3 | 6.1 | 6.7 | 80.6 | 3.6 | |||
| Staff in this pharmacy clearly understand their roles and responsibilities | 5 | 6 | 11 | 135 | 9 | 3.83 | 0.713 |
| 3 | 3.6 | 6.6 | 81.3 | 5.4 | |||
| This pharmacy is free of clutter | 6 | 11 | 12 | 133 | 3 | 3.7 | 0.775 |
| 3.6 | 6.7 | 7.3 | 80.6 | 1.8 | |||
| Staff in this pharmacy have the skills they need to do their jobs well | 5 | 4 | 10 | 137 | 10 | 3.86 | 0.687 |
| 3 | 2.4 | 6 | 82.5 | 6 | |||
| The physical layout of this pharmacy supports 3 workflow | 7 | 5 | 11 | 133 | 11 | 3.81 | 0.773 |
| 4.2 | 3 | 6.6 | 79.6 | 6.6 | |||
| Staff who are new to this pharmacy receive adequate orientation | 3 | 9 | 7 | 136 | 9 | 3.85 | 0.679 |
| 1.8 | 5.5 | 4.3 | 82.9 | 5.5 | |||
| Staff work together as an effective team | 4 | 5 | 12 | 134 | 11 | 3.86 | 0.678 |
| 2.4 | 3 | 7.2 | 80.7 | 6.6 | |||
| Staff get enough training from this pharmacy | 5 | 7 | 14 | 132 | 8 | 3.79 | 0.729 |
| 3 | 4.2 | 8.4 | 79.5 | 4.8 | |||
| 3.81 | 0.597 | ||||||
Communication and Work Pace
The total factor mean is 3.28 ± 0.543 with the highest and lowest mean for factor statements reported to be 3.37 and 3.04 respectively. The mean for the whole factor was again observed close to 3 which indicating that the factor has a medium value for itself and statements as well(Table 3).
Table 3: Communication and Work Pace Factor by Mean and Standard deviation for each Statement.
| Communication and Work Pace | Never | Rarely | Sometimes | Most of the time | Always | Mean | S.D |
| Staff ideas and suggestions are valued in this pharmacy | 2 | 10 | 117 | 29 | 6 | 3.16 | 0.639 |
| 1.2 | 6.1 | 71.3 | 17.7 | 3.7 | |||
| We encourage patients to talk to pharmacists about their medications | 3 | 3 | 111 | 32 | 12 | 3.29 | 0.713 |
| 1.9 | 1.9 | 68.9 | 19.9 | 7.5 | |||
| Staff take adequate breaks during their shifts | 2 | 3 | 111 | 33 | 18 | 3.37 | 0.748 |
| 1.2 | 1.8 | 66.5 | 19.8 | 10.8 | |||
| We have clear expectations about exchanging important prescription information across shifts | 1 | 4 | 114 | 34 | 7 | 3.26 | 0.609 |
| 0.6 | 2.5 | 71.2 | 21.2 | 4.4 | |||
| Staff feel comfortable asking questions when they are unsure about something | 2 | 2 | 111 | 35 | 16 | 3.37 | 0.724 |
| 1.2 | 1.2 | 66.9 | 21.1 | 9.6 | |||
| We have standard procedures for communicating prescription information across shifts | 4 | 5 | 108 | 34 | 13 | 3.29 | 0.758 |
| 2.4 | 3 | 65.9 | 20.7 | 7.9 | |||
| Our pharmacists spend enough time talking to patients about how to use their medications | 1 | 10 | 106 | 32 | 13 | 3.28 | 0.726 |
| 0.6 | 6.2 | 65.4 | 19.8 | 8 | |||
| Staff in this pharmacy discuss mistakes | 2 | 5 | 118 | 31 | 11 | 3.26 | 0.678 |
| 1.2 | 3 | 70.7 | 18.6 | 6.6 | |||
| We feel rushed when processing prescriptions | 3 | 2 | 117 | 31 | 12 | 3.28 | 0.697 |
| 1.8 | 1.2 | 70.9 | 18.8 | 7.3 | |||
| It is easy for staff to speak up to their supervisor/ manager about patient safety concerns in this pharmacy] | 2 | 4 | 109 | 32 | 19 | 3.37 | 0.766 |
| 1.2 | 2.4 | 65.7 | 19.3 | 11.4 | |||
| Our pharmacists tell patients important information about their new prescriptions] | 2 | 5 | 109 | 31 | 16 | 3.33 | 0.746 |
| 1.2 | 3.1 | 66.9 | 19 | 9.8 | |||
| We have enough staff to handle the workload] | 14 | 7 | 111 | 26 | 8 | 3.04 | 0.855 |
| 8.4 | 4.2 | 66.9 | 15.7 | 4.8 | |||
| When patient safety issues occur in this pharmacy, staff discuss them] | 1 | 9 | 113 | 30 | 13 | 3.27 | 0.708 |
| 0.6 | 5.4 | 68.1 | 18.1 | 7.8 | |||
| The status of problematic prescriptions is well communicated across shifts] | 2 | 8 | 114 | 31 | 7 | 3.2 | 0.651 |
| 1.2 | 4.9 | 70.4 | 19.1 | 4.3 | |||
| In this pharmacy, we talk about ways to prevent mistakes from happening again] | 0 | 7 | 115 | 28 | 13 | 3.29 | 0.673 |
| 0 | 4.3 | 70.6 | 17.2 | 8 | |||
| Interruptions/distractions in this pharmacy (from phone calls, faxes, customers, etc.) make it difficult for staff to work accurately] | 4 | 2 | 109 | 30 | 20 | 3.36 | 0.805 |
| 2.4 | 1.2 | 66.1 | 18.2 | 12.1 | |||
| 3.28 | 0.543591 | ||||||
Patient Safety and Response to Mistakes in Pharmacy
The mean total factor reported was is 3.71± 0.569 with highest and lowest mean been mean3.76 ± 0.656 and 3.63± 0.697 respectively indicating that the factor had medium to high values for itself and statements as well(Table 4).
Table 4 :Patient Safety and Response to Mistakes Factor by Mean and Standard deviation for each Statement
| Patient Safety and Response to Mistakes | Strongly Disagree | Disagree | Neither | Agree | Strongly Agree | Mean | S.D |
| Staff are treated 2ly when they make mistakes] | 3 | 10 | 32 | 115 | 1 | 3.63 | 0.697 |
| 1.9 | 6.2 | 19.9 | 71.4 | 0.6 | |||
| When a mistake happens, we try to figure out what problems in the work process led to the mistake] | 1 | 9 | 27 | 120 | 6 | 3.74 | 0.644 |
| 0.6 | 5.5 | 16.6 | 73.6 | 3.7 | |||
| This pharmacy helps staff learn from their mistakes rather than punishing them] | 2 | 6 | 30 | 122 | 3 | 3.72 | 0.622 |
| 1.2 | 3.7 | 18.4 | 74.8 | 1.8 | |||
| When the same mistake keeps happening, we change the way we do things] | 4 | 8 | 30 | 117 | 6 | 3.68 | 0.731 |
| 2.4 | 4.8 | 18.2 | 70.9 | 3.6 | |||
| This pharmacy is 3 at preventing mistakes] | 4 | 7 | 30 | 120 | 4 | 3.68 | 0.705 |
| 2.4 | 4.2 | 18.2 | 72.7 | 2.4 | |||
| We look at staff actions and the way we do things to understand why mistakes happen in this pharmacy] | 1 | 12 | 28 | 117 | 7 | 3.71 | 0.69 |
| 0.6 | 7.3 | 17 | 70.9 | 4.2 | |||
| Staff feel like their mistakes are held against them] | 3 | 7 | 31 | 117 | 4 | 3.69 | 0.681 |
| 1.9 | 4.3 | 19.1 | 72.2 | 2.5 | |||
| The way we do things in this pharmacy reflects a strong focus on patient safety] | 2 | 5 | 30 | 120 | 6 | 3.75 | 0.629 |
| 1.2 | 3.1 | 18.4 | 73.6 | 3.7 | |||
| Mistakes have led to positive changes in this pharmacy] | 3 | 4 | 30 | 120 | 7 | 3.76 | 0.656 |
| 1.8 | 2.4 | 18.3 | 73.2 | 4.3 | |||
| Patient Safety and Response to Mistakes | 3.7108 | 0.56925 | |||||
Documenting Mistakes
The total factor mean was 3.35± 0.68 with highest and lowest mean for factor statements been 3.44± 0.708 and 3.36± 0.707 respectively again indicating that factor has a medium to high values for itself and statements as well(Table 5).The overall comparison between the 4 parameters was made in Table No. 6.
 |
Table 5: The Percentage of each Item in Documenting Mistakes in Pharmacy Dimension. |
Note
Percentages indicate average percent response for each item response category across the pharmacy employee in the study.Overall Rating :Thus with response to overall rating it could be observed that while all the factors reported medium value to be high except Factor B i.e Communication and work pace which was found to be of medium value.
Table 6: Summary of mean scores of Patient Safety Culture of Pharmacies in KSUMC dimension
| Pharmacy Perceptions on Patient Safety Culture Dimension | Mean | SD | Level |
| Section A: Working in the Pharmacy | 3.81 | 0.597 | Above medium values to be high |
| Section B: Communication and Work Pace | 3.28 | 0.543 | A medium value |
| Section C: Patient Safety and Response to Mistakes | 3.71 | 0.569 | A medium value to be high |
| Section D: Documenting Mistakes | 3.35 | 0.680 | A medium value to be high |
On further evaluation, it was observed that only 1 factori.e working in the pharmacy did not have a significant difference between means for the Years of Work groups(Table 7). However, the other two factors namely, communication and work pace as well as patient safety and responses to mistake had been found to be statistically significant with notable differences between reported with respect of groups of years working variable(Table 7).
Table 7: Mean, Standard Deviation, and F Test for the Three Factors of Safety Improvement by Work Position.
| N | Mean | Std. Deviation | F | Sig. | ||
| Working in the Pharmacy | Pharmacist | 124 | 3.875 | .487 | 2.512 | .060 |
| technician | 26 | 3.676 | .690 | |||
| student | 13 | 3.458 | 1.058 | |||
| Others | 4 | 3.758 | .845 | |||
| *Communication and Work Pace How | Pharmacist | 124 | 3.112 | .309 | 25.289 | .000** |
| technician | 26 | 3.704 | .697 | |||
| student | 13 | 4.031 | .803 | |||
| Others | 4 | 3.432 | .777 | |||
| Patient Safety and Response to Mistakes | Pharmacist | 124 | 3.819 | .483 | 12.708 | .000 |
| technician | 26 | 3.136 | .634 | |||
| student | 11 | 3.798 | .461 | |||
| Others | 4 | 3.826 | .819 | |||
The areas of strength that were identi fiedor with a high level of agreement according to Like rt scale were teamwork in pharmacy, communications and work pace, response to mistakes, and documenting the mistakes. Positive responses were highest in teamwork within the pharmacy employees,(87.3% vs. 81.6%), staff training and skills within the pharmacy employees(86.35% vs. 79.25%), physical space and environment in the pharmacy (83.8% vs. 73.6%)compared to AHRQ’s 2019 community pharmacy database report 21. Lower responses were found in response to mistakes(79.75% vs. 74.4%) as compared to AHRQ’s 2019 community pharmacy database report 21.
The present findings indicated that ratings on documenting mistakes(reporting)as perceived by pharmacy employees were almost equivalent to another study conducted by AHRQ with regard to the community pharmacy in the United States21. Among the various factors, the weakest dimension identified was mistakes(reporting)having the lowest positive response with a mean score of 3. This denoted that a low level of agreement according to Like rt scale thereby confirming that the dimension need edurgent improvements. It has been time and again reported that health care professionals play a very significant role in reducing the medication errors. The methods used in improving the process includes; the introduction of computerized physician order entry(CPOE) and the adversative drug reaction(ADR) reporting which has led to advancement in detection and prevention of the medical errors.22
Thus, from the above findings,it can be observed that the pharmacy employees had little knowledge, attitude and practice to the existing medication errors and therefore were not aware of ways to significant reduce them. Patient safety overview in error detection and reporting require ethics, empathetic human approach,safety tools and vigilant system based on the interactive clerkships. Some of the findings from earlier studies described that pharmacy employees exhibited consciousness of the responsibility of adverse drug reaction reports and appropriate attitude towards it.24
Health care professionals had meagre knowledge and attitude towards pharmacovigilance. It could be supplemented by the fact that among the participants not only a single ADR has been reported to the medical Centre. The study therefore guides and provides information regarding the fact that education and exercise are most acknowledged means of advancing ADR reporting as pointed out by Anderson 25 et al. Thus, proper training and appropriate curriculum development and implementation is appropriate alternative way of improving the knowledge and attitude towards ADR reporting on medical errors. This will not only result in proper identification of causes of medication errors but will also minimize sentinel events within the hospital. As per our observation in the present analysis, there are 5 stages involved in the ordering and delivery in the pharmacy department namely, monitoring, administration, dispensing, transcription and prescription. Each phase represents a susceptible link in the chain along a diversity of medical errors. The most common stage/s associated with medical error are inadequate knowledge on drug prescription and knowledge concerning the patient whom drug is prescribed for.26
Data strongly advocates that the appropriate way of eliminating the medical error that may arise in each of the stage is by ensuring the standardization of medication process. Medication transcript error refers to communication failure between the prescribing clinician and supply staff. In the pharmacy department, it is mostly initiated by the oral medication instruction being misheard. To avoid such medical errors, it is vital to contrivance a protocol on use of verbal drug orders and take steps of including some retrospective, verification and documentation signing. Correction of medication error for the patient discharged from the pharmacy makes use of critical redundancies. The clinicians must ensure that they have confirmed the patient’s status of allergy, proved weight and implemented double checking on administering high risk medicine and medication errors prone to the population as advised by Vessal.27
Administration medical errors occur when a right drug is administered through a wrong route or a wrong drug is administered to the patient. Safety checklist helps to eliminate such type of errors and the staff is always encouraged to prescribe and offer dugs on the right dosage.28 A possible solution to reduce medication errors is to employ full-time pharmacists, based on results of some studies like that of Plutínská and Plevová,29 it is recommended that electronic health records together with clinical decision support systems, zero tolerance to handwritten orders, with the exception of situations requiring immediate help and a policy of not interrupting the professionals on work.
Limitations of the study: The present study was cross sectional in nature and included only the pharmacists. These limitations may include recall bias as well as communication barriers between investigators and participants. Similarly, the study was conducted only at one centreKSU University Hospital and henceforth the results cannot be generalized to the entire population.
Conclusion
The current study was premeditated to evaluate the attitude, knowledge and practice of the pharmacy employeesabout medication errors and patient safety in King Saud University Medical City, (KSUMC), Riyadh. Among the various factors, the weakest dimension identified was mistakes (reporting) having the lowest positive response with a mean score of 3 thereby indicating that the dimension needed improvement. It is therefore suggested that future researches can be carried out using more centers and more participants to evaluate the barriers of under-reporting of medication errors. Further studies could be also conducted to measure the compliance to ADR reporting with respect to different healthcare professionals and its correlation with patient safety.
Acknowledgement
The authors are grateful to all the participants who took time to complete this survey despite a busy schedule. Special thanks to King Saud University Hospital for supporting this work under Project No. E19-4311.
Conflict of Interest
The authors declare no conflict of interest
References
- Makary, M.A. and Daniel, M. (2016) Medical Error—The Third Leading Cause of Death in the US. BMJ, 353, i2139. https://doi.org/10.1136/bmj.i2139
CrossRef - Health and Safety Executive (2017). Employer’s responsibilities: Workers’ health and safety.[online] Hse.gov.uk. Available at: http://www.hse.gov.uk/workers/employers.htm WHO 2017,
- World Health Organisation (2017) WHO launches global effort to halve medication-related errors in 5 years.
- Elasrag GAE (2020) Nurses’ Perception of Factors Contributing to Medication Administration Errors International Journal of Research in Pharmaceutical Sciences DOI: https://doi.org/10.26452/ijrps.v11i1.1781
CrossRef - Alamrani K (2020) Perspectives on Causes and Barriers to Reporting Medication Administration Errors. Health Sci J. 14 No. 2: 70
- Ahmed Z, Mohammad S, Alan M. J, Abdullah M. Al-Hamid (2019) Medical errors: Healthcare professionals’ perspective at a tertiary hospital in Kuwait PLoS One https://doi.org/10.1371/journal.pone.0217023
CrossRef - Patton M Q (2015). Qualitative Evaluation and Research Methods. Thousand Oaks, CA: Sage.https://us.sagepub.com/en-us/nam/qualitative-research-evaluation methods/book232962
- Kaae, S., &Traulsen, J. M. (2015). Qualitative methods in pharmacy practice research. In Z-U-D. Babar (Ed.), Pharmacy Practice Research Methods, 49-68. Switzerland: Springer. https://doi.org/10.1007/978-3-319-14672-0_4
CrossRef - Alsulami S L, Sardidi H O, Almuzaini R S, Alsaif M A, Almuzaini H S, Moukaddem A K, Kharal M S (2019). Knowledge, attitude and practice on medication error reporting among health practitioners in a tertiary care setting in Saudi Arabia. Saudi medical journal, 40(3), 246. https://europepmc.org/article/pmc/pmc6468206
CrossRef - Hammoudi, B. M., Ismaile, S., & Abu Yahya, O. (2018). Factors associated with medication administration errors and why nurses fail to report them. Scandinavian journal of caring sciences, 32(3), 1038-1046. doi: 10.1111/scs.12546. Epub 2017 Nov 22
CrossRef - Alshahrani S M, Alakhali, K M, Al-Worafi Y M (2019). Medication errors in a health care facility in southern Saudi Arabia. Tropical Journal of Pharmaceutical Research, 18(5), 1119-1122. http://dx.doi.org/10.4314/tjpr.v18i5.29
CrossRefa - Stewart D, Thomas B, MacLure K, Wilbur K, Wilby K, Pallivalapila A, McLay J S (2018). Exploring facilitators and barriers to medication error reporting among healthcare professionals in Qatar using the theoretical domains framework: A mixed-methods approach. PloS one, 13(10), e0204987. doi: 10.1371/journal.pone.0204987. eCollection 2018.
CrossRef - George D, Supramaniam N D, Hamid S Q A, Hassali M A, Lim W Y, Hss A S (2019). Effectiveness of a pharmacist-led quality improvement program to reduce medication errors during hospital discharge. Pharmacy practice, 17(3). doi: 10.18549/PharmPract.2019.3.1501. Epub 2019 Aug 21.
CrossRef - Assiri G A, Alkhenizan A H, Al-Khani S M, Grant L M, Sheikh A (2019). Investigating the epidemiology of medication errors in adults in community care settings: A retrospective cohort study in central Saudi Arabia. Saudi medical journal, 40(2), 158. doi: 10.15537/smj.2019.2.23933
CrossRef - Al-Shara M. Factors contributing to medication errors in Jordan: a nursing perspective. Iran J Nurs Midwifery Res. 2011 Spring;16(2):158-61. PMID: 22224100; PMCID: PMC3249766.
- World Health Organization (2016) Consultative meeting planning for the global patient safety challenge: medication safety, 19-20 April 2016, WHO Headquarters Geneva, Switzerland: meeting report. World Health Organization. https://apps.who.int/iris/handle/10665/254990
- HeffernanL, K. (2013). The cross-cultural field excursion initiative:an educational approach to promote cultural competency in student pharmacists. Curr Pharm Teach Learn, 155–166.doi: 10.5688/ajpe77476
CrossRef - Mohammed I (2014) Medical errors on the rise. Arab News. https://www.arabnews.com/news/51980
- Thompson DC, Nuffer W, Brown K. Characteristics valued by the pharmacy practice community when hiring a recently graduated pharmacist. Am J Pharm Educ. 2012 Nov 12;76(9):170. doi: 10.5688/ajpe769170. PMID: 23193334; PMCID: PMC3508484.
CrossRef - Healthcare Research and Quality; October 2012; updated April 2014. AHRQ Publication No. 12(13)-0085. www.ahrq.gov/qual/patientsafetyculture/ pharmsurvindex.htm.
- Agency for Healthcare Research and Quality AHRQ . (2019). Community Pharmacy Database from: https://www.ahrq.gov/sites/default/files/wysiwyg/sops/surveys/2019-pharmacy-sops-database-report-parti.pdf
- Bourgeault, IRD et al (2010). The SAGE Handbook of Qualitative Methods in Health Research. London: SAGE.
CrossRef - Anderson JG, Ramanujam R, Hensel DJ, Sirio CA. Reporting trends in a regional medication error data-sharing system. Health Care Management Science. 2010 Mar;13(1):74-83. doi: 10.1007/s10729-009-9111-1. PMID: 20402284.
CrossRef - Austin, Z., & Sutton, J. (2014). Qualitative research: getting started. The Canadian journal of hospital pharmacy, 67(6), 436–440. https://doi.org/10.4212/cjhp.v67i6.1406
CrossRef - Anderson JG, Ann Friesen M, Fabian J, Swengros D, Herbst A, Mangione L. Examination of the Perceptions of Registered Nurses Regarding the Use of Healing Touch in the Acute Care Setting. J Holist Nurs. 2016 Jun;34(2):167-76. doi: 10.1177/0898010115592744. Epub 2015 Jun 29. PMID: 26130464.
CrossRef - Tong A, Winkelmayer WC, Craig JC. (2014) Qualitative research in CKD: an overview of methods and applications. American Journal of Kidney Disease. Sep;64(3):338-46.doi: 10.1053/j.ajkd.2014.02.026. Epub 2014 Apr 24. PMID: 24768353.
CrossRef - Vessal G, M. Z. (2009). Knowledge, attitudes, and perceptions of pharmacists to adverse drug reaction reporting in Iran. Pharma World & Science, 183-7. doi: 10.1007/s11096-008-9276-6. Epub 2008 Dec 31.
CrossRef - Austin Z, Sutton J. (2018). Research Methods in Pharmacy Practice: Methods and Applications Made Easy. New York: Elsevier Health Sciences. https://www.elsevier.com/books/research-methods-in-pharmacy-practice/austin/978-0-7020-7426-
- Plutínská, Z., &Plevová, I. (2019). Measures to prevent medication errors in intensive care units. Central European Journal of Nursing and Midwifery, 10(2), 1059-1067.
CrossRef

