A Comparative Study of Efficacy and Safety of Ondansetron, Glycopyrrolate and Dexamethasone for Post Operative Nausea and Vomiting Following General Aneasthesia
1Department of Pharmacology, University of Hafr Al Batin, Saudi Arabia.
2Department of Pharmacology, Bangalore Medical College and Research Institute, Bengaluru, Karnataka, India.
Corresponding Author E-mail: drafreen89@gmail.com
DOI : http://dx.doi.org/10.13005/bpj/2068
Download this article as:
![]()
Postoperative nausea and vomiting (PONV) is a common distressing problem in patients undergoing surgery under general anaesthesia which requires frequent medical interventions. This was a prospective, randomized study conducted in Victoria hospital, Bengaluru. Study subjects were randomly assigned into four groups of twenty patients in each. Group A received inj. Ondansetron 8 mg i.v, Group B received inj Glycopyrrolate 0.2 mg i.v, Group C received inj Dexamethasone 10 mg i.v and Group D received 1ml normal saline i.v, just before induction of anaesthesia with inj fentanyl and inj propofol. Number of patients having nausea & vomiting was assessed for 24 hrs after surgery. Out of eighty patients 47 (58.7%) patients had nausea and vomiting in the postoperative period. Six (30%) patients in group A, eleven (55%) in group B, thirteen (65%) in group C and seventeen (85%) patients in group D. Use of rescue antiemetic was higher in normal saline group followed by dexamethasone group. Headache was reported as an adverse effect in less than 10% of the patients. Our study showed that prophylactic use of ondansetron is more effective for prevention of PONV with lesser requirement of rescue medication and fewer side effects, followed by glycopyrrolate and dexamethasone.
KEYWORDS:Dexamethasone; General Anaesthesia; Glycopyrrolate; Ondansetron; Postoperative Nausea; Vomiting
Introduction
Post operative nausea and vomiting (PONV) is defined as nausea and/or vomiting occurring within 24 hours after surgery which significantly contribute to patient’s discomfort, distress and dissatisfaction.1 It affects 20-30% of patients and the incidence can be as high as 70% to 80% among high-risk group such as female and obese patients, patients with previous history of PONV and patients with history of motion sickness etc.2 Nausea, vomiting and retching are among the most common postoperative complaints following general anesthesia
Patients report that avoidance of PONV and postoperative pain is of equal concern. When severe, PONV is associated with bleeding, electrolyte imbalance, dehydration, pulmonary aspiration and wound dehiscence resulting in prolonged hospital stay & increased health care cost3.There is a constant search for an agent to reduce its incidence & severity. A number of anti-emetics have been studied for the prevention and treatment of PONV and are grouped according to the type of receptors at which they act, usually as an antagonist like anticholinergic, antihistaminic, dopamine receptor antagonist, 5HT3 receptor antagonist and corticosteroids4.
Ondansetron is a 5-HT3 antagonist, exerts its antiemetic & antinauseant effect by blocking serotonin induced depolarization of vagal afferent nerves. It was developed to control cancer chemotherapy/ radiotherapy induced vomiting but later found to be effective in PONV.5
Glycopyrrolate is potent & long acting quaternary antimuscarinic with no central effects. Its antisecretory action on the bronchial & salivary secretions is an additional feature and hence it is preferred agent in anaesthetic practice.6
Dexamethasone is a potent and highly selective long acting glucocorticoid. The precise mechanism of its antiemetic action is not known but may be due to prostaglandins antagonism, serotonin inhibition in the gut and release of endorphins. It augments the efficacy & reduce the side effects of other antiemetics.7
Since 1981, dexamethasone has been reported to be effective in reducing the incidence of emesis in patients undergoing chemotherapy. A study done by Laiq N et al showed the antiemetic effect of dexamethasone to be equal to or better than the 5-HT3 receptor antagonists, such as ondansetron and granisetron8. A systematic review by Assente J9 et al showed that use of single perioperative dose of dexamethasone does not affect wound healing and can be use for prophylaxis of PONV.
Hence the present study was taken up to compare the efficacy and safety of three widely used drugs with different mechanism of action with placebo as prophylactic antiemetic for control of PONV in patients undergoing surgery under general anesthesia.
Methods
This was a prospective, single blind randomized, placebo-controlled study conducted at department of Anaesthesiology in Victoria hospital attached to Bangalore Medical College and Research Institute, Bengaluru. The study duration was from September 2017 to December 2017.
After taking institutional ethics committee approval, eighty patients of age group 18-50 years and ASA (American Society of Anesthesiology) physical status of grade I and II scheduled for various elective and emergency procedures under general anesthesia were enrolled in the study. Patients with high risk of PONV such as patients with history of motion sickness, previous history of PONV, and obese females were excluded from the study.
After pre-anaesthetic evaluation and investigations, the patients were explained about the procedure and written informed consent was obtained. Standard pre-operative procedure was followed and baseline vital parameters were recorded. Patients were randomly assigned into four groups of 20 patients in each group.
Group A (n=20): received inj Ondansetron 4 mg i.v
Group B (n= 20): received inj Glycopyrrolate 0.2 mg i.v
Group C (n=20): received inj Dexamethasone 10 mg i.v
Group D (n=20): received Normal saline i.v
All the study drugs were given intravenously just before induction with injection fentanyl 2 mcg/kg intravenously+ inj Midazolam 0.02 mg/kg iv, followed by intravenous propofol 2 mg/kg + inj Vecoronium 0.1 mg/kg iv. They were pre oxygenated with 100% oxygen for 3 minutes. Anaesthesia was maintained with N2O: O2= 50:50 @ 3 lts/min+ isoflurane 0.8- 1.2 % and reversal of neuromuscular blockade was done with Neostigmine 0.05 mg/kg + Atropine 15 mcg/ kg iv
During the follow up period of 24 hours after surgery, Heart rate, Blood Pressure, Respiratory rate and severity of nausea and vomiting was monitored and recorded at 0, 15, 30, 60 min and 2 hr in the recovery room and 4, 6, 12, 18, 24 hours in the post operative ward.
Rescue antiemetic metoclopramide 10 mg iv was given if any episodes of nausea or vomiting occurred. The incidence of side effects was recorded in the adverse drug reaction form.
Statistical Analysis
Statistical analysis was performed using Kruskal Wallis test. Continuous variables were expressed as mean ± SD (patient’s age, weight and duration of surgery) and discrete variables were expressed as the number of episodes of nausea, vomiting and the number of adverse events in each group. Mann Whitney test was used for post hoc analysis. Categorical data such as ASA grade & gender was compared using chi square test. P value of <0.05 was considered statistically significant
Results
Table 1: Demographic details of patients in all groups
|
Characteristic
|
Normal saline
(n=20) |
Ondansetron
(n=20) |
Glycopyrrolate
(n=20) |
Dexamethasone (n=20) | P value |
|
Age(Mean±SD)(yrs)
|
37.1 ± 7.4 | 36.5 ± 11.9 | 39.4 ± 9.8 | 38.05 ± 8.9 | 0.11*
|
|
Sex M:F |
13/7
|
12/8 |
10/10 |
12/8 |
0.98# |
|
Weight (mean±SD) (kgs) |
54.33 ± 5.23 | 53.85 ± 5.79 | 56.9 ± 5.17 | 53.45 ± 6.42 | 0.56*
|
|
ASA Grade (I/II) |
13/7
|
12/8 |
16/4 |
11/9 |
0.42# |
| Duration of surgery (mean±SD) (min) | 72 ± 24.8 | 71.5 ± 18 | 75 ± 23.05 | 70.75 ± 17 | 0.92* |
| Statistical method used was*ANOVA & #Chi square | |||||
The demographic characteristics of all the patients with respect to age, sex, weight, ASA grade, duration of surgery are summarized in Table 1
Table 2: Incidence of Post operative nausea and vomiting
| Study groups | No PONV reported | PONV reported | Comparison group | P value |
| Ondansetron
n=20 |
14(70%) | 6(30%) | Ondansetron vs Glycopyrrolate | 0.30 |
| Glycopyrrolate
n=20 |
09(45%) | 11(55%) | Ondansetron vs Dexamethasone | 0.04* |
| Dexamethasone
n =20 |
07(35%) | 13(65%) | Ondansetron vs normal saline | 0.001* |
| Normal saline
n =20 |
03(15%) | 17(85%) | Glycopyrrolate vs Dexamethasone | 0.34 |
|
_
|
_ |
_ |
Glycopyrrolate vs
normal saline |
0.01* |
|
_ |
_ |
_ |
Dexamethasone vs
normal saline |
0.09 |
|
A Kruskal Wallis test showed statistically significant difference in the number of events of post operative nausea & vomiting among the different treatment groups Χ2 (3) = 13.992, p= 0.003. Mann-Whitney U test was used as a post hoc test for analysis between the test groups. P value <0.05* was considered as statistically significant |
||||
In this study patients in ondansetron group had least number of episodes of nausea and vomiting as compared to glycopyrrolate and dexamethasone group, with lesser requirement of rescue medication. (table 2 & figure 1)
On post hoc analysis, we found no statistically significant difference between ondansetron and glycopyrrolate with a p value 0.3 (table 2)
 |
Figure 1: Time to event analysis |
Figure 1 shows the time for requirement of rescue antiemetic in all the groups. It is seen from the graph that in normal saline group the first rescue antiemetic was required earlier (within 30 mins) postoperatively and it is most often used as compared to that in ondansetron group in which the first rescue medication was used very late (after 120 mins) and it is less often used.
Adverse drug reaction was seen in all the groups, headache being the most common. The other symptoms such as dry mouth and constipation were seen in glycopyrrolate group because of its antisecretory property. (figure 2)
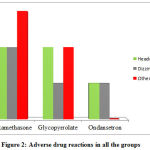 |
Figure 2: Adverse drug reactions in all the groups |
Discussion
Post operative nausea and vomiting are common distressing complications of anaesthesia. Despite the rapid progress in the field of modern anaesthesia, it is continued to be a major factor interfering with postoperative convalescence.8
The etiology of PONV is multi-factorial and includes factors both related to anaesthesia and unrelated to anaesthesia. The later include age, gender, weight, history of motion sickness and previous history of PONV. Operative factors include type and duration of surgery, surgical skill, post operative pain which along with anaesthetic management further contributes to increased incidence of PONV. Intra operative nausea and vomiting hampers surgical procedure, while post operative nausea and vomiting creates risk of wound dehiscence, besides causing discomfort to patients.
In the present study, the treatment groups were similar in terms of patient demographic characteristics, anaesthetic administered and postoperative rescue medication. In addition, patients with a history of motion sickness, obese females and previous history of PONV had been excluded from the study. Therefore, the difference in incidence of PONV between the groups might be attributable to the variation in antiemetic drugs administered.
In the present study, all the three study medications, ondansetron, glycopyrrolate, dexamethasone had significant antiemetic effect as compared to placebo. Ondansetron had significantly higher antiemetic efficacy than dexamethasone, but similar to glycopyrrolate. The efficacy of glycopyrrolate and dexamethasone was similar.
Ondansetron is 5-HT3 receptor antagonist, which is effective in preventing PONV. The effectiveness of intravenous (i.v.) ondansetron as prophylactic postoperative antiemetic was evaluated by McKenzie 9,10 and colleagues in dose ranging study, which showed that ondansetron in a dose of 4mg as well as 8 mg was equally effective in prophylaxis of PONV. A dose response study by Sadhashivam SK11 et al also highlighted that the efficacy of different doses of ondansetron as a prophylaxis for PONV
A study by Khalid Ahsan12 et al and Suvalka U13 et al reported that 72% and 75% of patients undergoing laproscopic surgery under general anaesthesia were free of emesis with Ondansetron 4-8 mg given iv for prophylaxis, which was comparable with the results of the present study.
In this study the efficacy of ondansetron was better than glycopyrrolate but was not found to be statistically significant in preventing PONV which is akin to the previous study done by Jain R14 et al which showed that the effect of glycopyrrolate on nausea and vomiting during caesarean section are comparable to ondansetron, but with an increased incidence of dry mouth.
A study by Suvalka U13 et al and Vrinda O15 et al showed that efficacy of ondanseteron was better than dexamethasone with lesser side effects which is similar with the results of the present study.
In this study, on comparison of glycopyrrolate with dexamethasone, both showed similar efficacy in preventing PONV (p value =0.34), which is not in consistent with the study done by Biswas B N et al16 which reported that the efficacy of glycopyrrolate was higher when compared to dexamethasone.
Glycopyrrolate unlike atropine, is a quaternary ammonium anticholinergic. By inhibiting the action of acetylcholine on muscarinic receptors, it decreases the gastric secretions besides decreasing pharyngeal, tracheal, and bronchial secretions, hence it is an antiemetic and anti secretory.
Our findings between glycopyrrolate and normal saline was found to be statistically significant (55% vs 85%) which confer with the results by Ure D et al 17. and Biswas BN et al 16 which also showed glycopyrrolate was superior to placebo.
This study also demonstrated decreased incidence of nausea and vomiting with dexamethasone but significant levels were not reached (p value =0.09) as compared to normal saline, which is in consistent with a placebo controlled study conducted by Khatiwada S et al18 which showed that the use of dexamethasone prior to subarachnoid block in patients undergoing total abdominal hysterectomy significantly reduces the incidence of nausea and vomiting and the requirement of antiemetic in the postoperative period, with better patient satisfaction.
Dexamethasone was first reported as an antiemetic in patients receiving cancer chemotherapy in 1981, it is a glucocorticoid that produces a strong antiemetic effect by an undetermined mechanism 19,20. A wide range of doses of dexamethasone (8-32 mg) has been used in the management of PONV and emesis associated with chemotherapy. Among these doses 8-10 mg has been used most frequently in the prevention of PONV, hence 8 mg dose was chosen for the present study 21
Strength of the present study is that, we compared the antiemetic efficacy of 3 drugs with different mechanism of action. For reversal of anaesthesia, along with neostigmine, atropine was used in order to avoid bias instead of glycopyrrolate which is otherwise used routinely which further adds to the strength of the study. Limitation of the present study was we included all types of surgeries under general anaesthesia.
Conclusion
This study concludes that the prophylactic use of ondansetron and glycopyrrolate was more effective with fewer side effects in reducing the incidence of nausea and vomiting postoperatively than with dexamethasone.
Acknowledgements
The authors would like to thanks the faculty and post graduate students of department of Aneasthesiolgy, Victoria Hospital attached to Bangalore Medical College & Research Institute, Bengaluru, for their help in conducting the research project.
Funding Source
There is no Funding Source.
Conflict of Interest
There is no Conflict of Interests.
Ethical Approval
Obtained
References
- Kovac AL. Prevention and treatment of postoperative nausea and vomiting. Drugs 2000;59: 213–43.
CrossRef - Gan TJ. Post operative nausea and vomiting can it be eliminated? JAMA. 2002;287:1233-1236
CrossRef - Ramanathan, Augustus, Thiruvengadam, Sundaram M, Deepalakshmi. Efficacy of propofol in preventing postoperative nausea and vomiting: single blind randomized control study. The Int J of Anaesthesiol. 2003; 7:1092-406.
CrossRef - Dalvi N P, Chimalwar S. A Prospective, Randomised, Double-Blind Comparative Study of IV Granisetron Vs Dexamethasone as Antiemesis Prophylaxis in Patients Undergoing Elective Abdominal Laparoscopic Surgery. IJSR.NET. 2016;5(7): 1721-1726.
CrossRef - Sharkey KA, Wallace JL. Treatment of disorders of bowel motility and water flux; antiemetics; agents used in biliary and pancreatic disease. In: Brunton L, Chabner B, Knollman B. Goodman & Gilman’s the pharmacological basis of therapeutics,12th New York: Mc Graw Hill;2011.p1227-1228
- Brown JH, Laiken N. Muscarinic receptor agonist and antagonist. In: Brunton L, Chabner B, Knollman B. Goodman & Gilman’s the pharmacological basis of therapeutics,12th New York: Mc Graw Hill;2011.p237-238
- Apfel CC, Kranke P, Katz MH, Goepfert C, Papenfuss T, Rauch S, et al. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth 2002;88:659–68
CrossRef - Gupta P, Jain S. Post operative nausea and vomiting prophylaxis: a comparative study of ondansetron, granisetron and granisetron & dexamethasone combination after modified radical mastectomy. Saudi J Anaesth 2014; 8(1):67-71
CrossRef - McKenzie R, Tantisira, Boonrak , Karambelkar, Deepa J, Riley et al: Comparison of ondansetron with ondansetron plus dexamethasone in the prevention of postoperative nausea and vomiting. Anaesthesia Analgesia 1994; 79: 961-4.
CrossRef - Paventi S, Santevecchi A, Ranieri R. Efficacy of a single-dose ondansetron for preventing post-operative nausea and vomiting after laparoscopic cholecystectomy with sevoflurane and remifentanil infusion anaesthesia. Eur Rev Med Pharmacol Sci. 2001; 5: 59-63
- Sadhasivam Sk, Shende D, Madan R .Prophylactic Ondansetron in Prevention of Postoperative Nausea and Vomiting following Pediatric Strabismus Surgery. A Dose-Response Study. Anaeathesiol. 2000;92(4):1035-1042.
CrossRef - Ahsan K, Abbas N, Nadeem Naqvi S M, Murtaza G, Tariq S et al.Comparison of efficacy of Ondansetron and Dexamethasone combination and Ondansetron alone in preventing postoperative nausea and vomiting after laparoscopic cholecystectomy. J Pak Med Assoc. 2014;64(3):242-246.
- Suwalka U, Parmar D, Doshi S, Jha P. Efficacy comparison of ondansetron with dexamethasone in preventing nausea and vomiting in post laparoscopic surgeries. Indian J res rep med sci. 2013;3 (1): 20-22.
- Jain R, Sharma S. A comparative study of effects of glycopyrrolate and ondansetron on nausea and vomiting in cesarean section under spinal anesthesia. Anesth Essay Res. 2015;9(3) :348-352
CrossRef - Vrinda Oza ,Srinivasa S, Abhijeet I, Jigisha B, Chhaya A V. Comparison of ondansetron & dexamethasone in prevention of postoperative nausea & vomiting in laparoscopic surgery. Int J Biomed Res. 2014;5(2): 110-112
CrossRef - Biswas BN, Rudra A, Das SK, Nath S, Biswas SC. A comparative study of glycopyrrolate, dexamethasome and metoclopramide in control of nausea and vomiting after spinal anesthesia for caesarean delivery. Indian J Anaesth. 2003;47:198–200.
- Ure D, James KS, McNeill M, Booth JV. Glycopyrrolate reduces nausea during spinal anaesthesia for caesarean section without affecting neonatal outcome. Br J Anaesth. 1999;82:277–9
CrossRef - Khatiwada S, Bhattarai B, Biswas BK, Pokharel K, Acharya R, Singh SN et.al. Postoperative Nausea and Vomiting in Patients Undergoing Total Abdominal Hysterectomy Under Subarachnoid Block: a Randomized Study of Dexamethasone Prophylaxis. Kathmandu Univ Med J. 2012; 38(2):41-45.
CrossRef - Wang J. J.,Ho S. T., Liu H.S., Ho C.M.: Prophylactic antiemetic effect of dexamethasone in women undergoing ambulatory laparoscopic surgery. British Journal of Anaesthesia 2000; 84(4):459-62.
CrossRef - Gupta P, Jain S. Post operative nausea and vomiting prophylaxis: a comparative study of ondansetron, granisetron and granisetron & dexamethasone combination after modified radical mastectomy. Saudi J Anaesth 2014; 8(1):67-71
CrossRef - Bano F, Zafar S, Aftab S , Haider S. Dexamethasone Plus Ondansetron for Prevention of Postoperative Nausea and Vomiting in Patients Undergoing Laparoscopic Cholecystectomy: A Comparison with Dexamethasone Alone. J Coll Physicians Surg Pak. 2008; 18 (5): 265-269.




