
Manuscript accepted on :December 15, 2016
Published online on: --
Plagiarism Check: Yes
Alagarsamy Venkatesh1, B. Anuradha2, A. Karthick1, P. E. Chandra Mouli3 and M. Ramasamy4
1Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Pallikaranai, Chennai-600100.
2Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Pallikaranai, Chennai-600100.
3Department of Oral Medicine and Radiology, Sri Venkateswara Dental College and Hospital, Thalambur, Chennai. Tamil Nadu, India.
4Department of Orthodontics, Sri Venkateswara Dental College and Hospital, Chennai, Tamilnadu, India.
Corresponding Author E-mail: denvenkat@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1047
Abstract
Binder’s syndrome is an uncommon congenital condition which develops in the first trimester of pregnancy and has characteristic effects on the facial features. Those effects are: arhinoid face, intermaxillary hypoplasia (associated with malocclusion), abnormal position of the nasal bones, nasal mucosa atrophy, anterior nasal spine agenesis and (in most cases) a lack of frontal sinuses. Other deformities, as well as mental retardation, are also possible. Due to the clinical appearance, patients require surgical and orthodontic treatment. The main surgery performed in these patients is nose reconstruction with bone or cartilage grafts. Usually patients require more than one surgical procedure due to graft resorbtion and an unsatisfactory appearance. Orthodontic treatment is based on Class III treatment (pseudo-mesio-occlusion) and relieving dental crowding. The treatment of malocclusion may require combined orthodontic and surgical treatment. In younger patients maxillary protraction with rapid palatal expansion could be an adequate approach. We present a rare case of Binder’s syndrome in a 15 years old male patient and discuss about the various treatment modalities available.
Keywords
Binder’s syndrome; maxillofacial hypoplasia; pseudoprognathism
Download this article as:| Copy the following to cite this article: Venkatesh A, Anuradha B, Karthick A, Mouli P. E. C, Ramasamy M. Binder’s Syndrome – A Rare Case Report and Review of Literature with Detailed Treatment Plan. Biomed Pharmacol J 2016;9(3). |
| Copy the following to cite this URL: Venkatesh A, Anuradha B, Karthick A, Mouli P. E. C, Ramasamy M. Binder’s Syndrome – A Rare Case Report and Review of Literature with Detailed Treatment Plan. Biomed Pharmacol J 2016;9(3). Available from: http://biomedpharmajournal.org/?p=11866 |
Introduction
The facial features of a new syndrome were first described by Noyes in 1939, although it was von Binder who (in 1962) identified and defined all the features of the syndrome. Von Binder, who called this syndrome “maxillonasal dysostosis”, reported the six most characteristic features of the syndrome: arhinoid face, intermaxillary hypoplasia (associated with malocclusion), abnormal position of the nasal bones, nasal mucosa atrophy, anterior nasal spine agenesis and (in most cases) a lack of frontal sinuses [1–4].
Case Report
A 15 years old male patient complained of difficulty in speech and breathing since childhood. History of the presenting illness revealed difficulty in breathing since child hood due to nasal obstruction and is more aggravated during common cold attacks. There is difficulty in speech with nasal twang and there is difficulty in pronouncing some words since child hood and he is much concerned about both these conditions and seeked medical help and was instructed to undergo surgery 2 years back but refused for that and now he has came with the same complaints to our hospital.
His parents give the history of decreased intelligence and decreased hearing capacity and was not able to go to school more than 5 years and stopped going to school.
There is difficulty in pronouncing T, D, S, and X. There is nasal twang in the voice and the patient is not uttering the words in a continuous manner and takes some time to think for the answers and sometime gives irrelevant answers to the questions asked. Intra orally, high arched palate was present. (Fig 3) Extra orally there is downward slanting of both the palpebral fissures. There is deficiency in the mid face with depression in the malar prominence with slight depression in the nasal bridge. In the profile view there is pronounced depression in the nasal bridge and the malar prominence with flat mid face. The pinnas of the ears are small. (Fig 1)
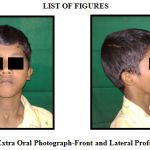 |
Figure 1: Extra Oral Photograph-Front and Lateral Profile View |
There is class III maxillo mandibular relation which is shown as forwardly placed mandible.
In the neck there is 5cm X 7cm diffuse swelling seen in the region of thyroid gland that moves along with the thyroid gland on swallowing. The swelling is superiorly 2cm from the base of the mandible, inferiorly 5cm from the sternum, 3cm from the midline on the both the side of the midline. The surface is smooth and margins are diffuse. (Fig 2)
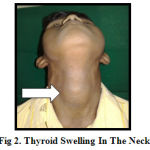 |
Figure 2: Thyroid Swelling In The Neck |
Inspectory findings are confirmed by palpation. There is no raise in temperature over the swelling. The swelling is non tender on palpation and the margins are well defined and soft to firm in consistency. Intra orally the palatal vault is high.
 |
Figure 3: Intra Oral Photograph-High Arched Palate |
A provisional diagnosis of Mid face deficiency was made.
OPG and Chest radiograph showed no abnormalities. (Fig 5) Lateral Cephalogram revealed deficiency in the formation of nasal septal cartilage and deficiency in the zygomatic bones. (Fig 4) The mandible is placed forwardly depicting a Class III maxillo mandibular relation.
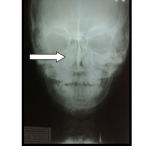 |
Figure 4: Pa View-Skull- shows deviated Nasal Septum |
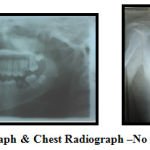 |
Figure 5: Orthopantomograph and Chest Radiograph –No Abnormalities Detected |
Correlating all the clinical and radiographic features, a final diagnosis of Binder’s Syndrome was made.
Discussion
Binder’s syndrome (also known as maxillofacial hypoplasia) is characterized by hypoplasia of the nasomaxillary structures. This feature is caused by a disturbance of growth in the pros- encephalic induction center. The process of nose formation normally takes place during the third month of pregnancy [2, 5]. Males and females are equally affected by Binder’s syndrome. The syndrome is quite rare, which may be a reason for the lack of knowledge of its true etiology, inheritance patterns and real prevalence. Beside hypoplasia of the nose, patients may present bilateral loss of hearing and mental retardation (although there is no proof that Binder’s syndrome is associated with lower intelligence) [1]. The majority of cases are isolated, but there are some reports of family recurrence of the syndrome (among siblings or parents and children); a positive family history was reported in 36% of the subjects of one study [6, 7]. This suggests that the inheritance pattern is either autosomal recessive with reduced penetrance or multifactorial [1, 2, 6, 7]. There are reports that Binder’s syndrome has a direct association with vitamin K deficiency [2, 8]. In some cases other congenital diseases and abnormalities (such as Down syndrome, autonomic neuropathy and strabismus) are observed [1]. According to Nedev, 5% of patients are found to present hearing loss and the same number of patients presents congenital heart diseases [2].
Facial Features
The main facial feature in Binder’s syndrome is arhinoid face with a flat and vertical nose as a result of hypoplasia of the nasomaxillary structures [1, 3]. Other characteristic facial features of the syndrome are maxillary hypoplasia (and hypoplastic midface profile) with severe malocclusion, reduced nasal spine, nasal mucosa atrophy and abnormal position of nasal bones. Sometimes a lack of frontal sinuses is observed, but it is not obligatory [2, 3].
Besides the flat nose, a concave facial profile is one of the characteristics of Binder’s syndrome [9]. The naso-frontal angle is reduced [10]. Hypertelorism can also be observed [2]. The columnella / lip junction is short and retracted [1, 5]. A lack of the normal triangular shape in the lower part of the columnella is observed. The nostrils, observed from below, have a semi-lunar (half moon) or crescent shape. If the hypoplasia is severe, the nostrils may be triangular [1–5]. Skeletal hypoplasia in the nasal floor, around the excavations-fossae prenasales and piriform aperture, is observed bilaterally [9].
Perialar flatness is also typical for individuals with Binder’s syndrome [2]. The soft tissues are of the normal length; no shortage is observed [9]. Maxillary hypoplasia causes a convex upper lip [2]. The nasolabial angle, measured between the tip of the nose and upper lip, is acute. According to Holmstroem et al., in Binder’s syndrome it has a value of 76–88° instead of the normal 103–117° (according to Segner and Hasund’s cephalometric analysis). The acute nasolabial angle is mainly a result of the convexity of the upper lip, a deep fold or fossa between the nose and the upper lip, and a flat philtrum [1–5].
Skeletal and Dental Abnormalities
The skeletal changes in Binder’s syndrome have a direct impact on patients’ facial features. The anterior crest separating the floor of nasal cavity is missing, and the anterior nasal spine can be either hypoplastic or missing. This results in a flat profile without nasal prominence [1, 11]. The scaphoid depression that researchers observe lies in the anterior floor of the nasal cavity; although observed clinically, it is not seen on radiographs [1].
The nasal bones, however, are of a normal length [9]. According to most of the studies, one of the most common characteristics of Binder’s syndrome is hypoplasty or lack of the frontal sinuses (seen in 40–50% of the cases) [1, 2].
The anterior cranial base is short (a reduced sella-nasion distance), and the maxilla is positioned posteriorly, which leads to Class III malocclusion and relative prognathism [1, 3]. Beside this, the convexity of the maxilla is abnormal [11]. Some patients may present a cleft palate in association with the syndrome [1]. Delaire et al. observed that most Binder’s syndrome patients suffer from microdontia of the central upper incisors; a lack of lateral incisors has also been observed, but rarely [1, 11]. Dental anomalies are often present, usually secondary to malocclusion, and may result in dental crowding and changes in tooth positions [1]. Amelogenesis imperfecta was observed in one patient [5]. In addition to skeletal changes in the skull, about 44.2% of Binder’s syndrome patients present irregularities in the cervical spine, which arise during those structures’ development in the third month of pregnancy – the same period as nose formation. This highlights the importance of environmental factors in the development of this deformity. Most frequently the C1 and C2 vertebrae are affected: Their hypoplastic arches may present abnormal patterns of ossification [1, 2, 6]. The most frequent anomalies in vertebral structures are odontoid process, a short posterior arch, spina bifida occulta and blocked vertebrae [2]. It is believed that patients with Binder’s syndrome often suffer from mild arhinencephaly. However, there have been no reports of difficulties with the sense of smell [1].
Differential Diagnosis
The differential diagnosis for Binder’s syndrome is based on similar facial features in other syndromes. This should include Warfarin embryopathy, Down syndrome, Apert syndrome, Stickler syndrome, Keutel syndrome and Acrodysostosis. These syndromes can frequently be misdiagnosed during fetal ultra sonogram (USG) examinations. Binder’s syndrome can be easily diagnosed by using 2D and 3D ultrasounds, beginning with the 21st week of pregnancy. Early diagnosis is important, as nasal malformations are present in 1:1600 fetuses and may play an essential role in the early diagnostics of congenital diseases and syndromes [1, 10–14]. It should also be considered that Down syndrome is often associated with Binder’s syndrome. It has been reported that 12% of patients with trisomy 21 lack a nasal bone [2, 15]. Among aborted fetuses with Down syndrome, the index is even higher – anomalies in the nasal bone are observed in 60% of those (in 26% the nasal bone is absent, and in 36% it is hypoplastic) [2, 16]. It is also believed that Binder syndrome may be a mild form of chondroplasia punctata [17].
Treatment
Surgical Treatment
Surgical treatment for Binder’s syndrome is usually performed by plastic surgeons and is limited to nasal dorsum reconstruction – elevation of the tip of the nose and lengthening of the nasal dorsum [2, 18]. After the surgical procedure the nasolabial angle increases from 76–88° to the correct 100–106°, but a slight relapse is subsequently observed [5, 9]. The convexity of face at the tip of the nose (the glabella-pronasale-pogonion angle) improves after surgery. The type of surgical procedure depends on the facial malformation – in case of a depressed nasal dorsum, an L-shaped bone graft is the favored procedure, while repositioning the septum is indicated if the upper section of the nose is found normal. A cartilage graft requires secondary correction more rarely than a bone graft. As much as 28% of the volume of a transplant is resorbed. According to Rune et al., nose length decreases by an average of 13 mm from its length the day after the surgery. The main resorbtion takes place within the first two years after surgery. It is probable that the short arm of an L-shaped bone graft is replaced by fibrous tissue.
Due to the graft’s resorbtion or a lack of bone reorganization after surgery (mainly in the nose tip projection) relapse is observed. Therefore revision of the surgery and a secondary bone or cartilage graft is necessary in one fourth of the patients [5, 9, 18]. Bone and cartilage grafts are usually carried out from 14 years of age, and precede osteotomy of the maxilla and/or nose (performed at the age of 18 or later) [2]. If the appearance of the nose after surgery is not sufficiently satisfactory, nasolabial flaps may be used to resurface the lining [19].
In some cases, if mandibular length is increased, true prognathism may be observed [1, 20]. The most severe cases of malocclusion require Le Fort I or Le Fort II osteotomy, which is performed on adult patients in addition to the nasal grafting. Therefore combined orthodontic and surgical treatment is required [1, 2]. Sometimes only otolaryngological procedures (such as open-structure rhinoplasty) are necessary. In more severe the cases, though, complicated surgical procedures are necessary – first transmaxillary segmentary osteotomy, followed by nasal reconstruction (lenghthening of the nose and improving the tip projection) in the second stage of surgery [21].
Orthodontic Treatment Planning
Surgical correction of nasal and maxillary abnormalities is usually followed by orthodontic treatment. Planning the orthodontic treatment depends on the severity of the malocclusion. In mild cases, when compensatory effects in dental arches are present, orthodontic treatment may not be necessary [2, 3, 26]. Most Binder’s syndrome patients
present Class III malocclusion with prominent lower incisors [22]. In 5% of cases pseudoprognathism is observed; as noted above, in some cases mandibular length is increased and true prognathism is observed [1, 3, 20]. Proclination of the upper incisors is a kind of compensation for a short, retrogenic maxilla that “masks” malocclusion. The proclination of lower incisors does not have any specific trend [3]. No correlation has been observed between the severity of malocclusion and the presence of spine abnormalities in patients with Binder’s syndrome [1]. In mild cases of Class III malocclusion, orthodontic therapy with an upper and lower fixed appliance with Class III elastics is conducted [3]. As noted above, the most severe cases of malocclusion require Le Fort I or Le Fort II osteotomy combined with orthodontic treatment. Therefore, braces to decompensate malocclusion are fixed to the teeth to prepare the patient for the osteotomy [1, 2]. In these cases orthodontic treatment should be performed after the patient’s growth has finished [3].
In younger patients facemask therapy may be a successful treatment modality. In this case it is a good idea to use rapid maxillary expansion in order to achieve maxillary suture disruption. For the procedure to have the best results, the skeletal age of the individual should be established (for example by analyzing a hand-wrist radiograph or cephalograms). The best timing for this procedure is before the “growth peak”, when there is greater positive reaction to the protraction forces. The use of facemask therapy at this stage may eliminate the need for LeFort I and LeFort II osteotomy in adulthood. It is important to bear in mind that protraction of the maxilla should be carried out carefully in high-angle patients and can be combined with maxillary expansion, if necessary. Often, bone augmentation in the growth phase of the treatment contributes to better treatment results [23–26].
The premolars are usually extracted to relieve dental crowding, and these extractions are justified in both the upper and lower arches. In some cases, when the lower incisors are proclined, only the lower premolars are extracted and orthodontic camouflage is conducted. The H angle is a cephalometric angle describing the relation of the soft tissue to the bone structures (between the lines H and NB). After orthodontic camouflage the H angle is reduced to less than 9.2° (the average in the general population), which means that although this therapy technique improves occlusion, it has a negative impact on facial esthetics [3, 27].
Conclusion
Binder’s syndrome is a rare congenital malformation that mainly affects facial features. Treatment planning requires nose reconstruction first of all, but sometimes other medical care (such as orthodontic and orthognatic treatment) is also necessary. From the day the child is born he or she should be under the care of a plastic surgeon and orthodontist. The timing and types of procedures involved in the treatment of patients with maxillonasal dysplasia depend on the severity of the malformation and are planned individually.
References
- Quarrell OWJ, Koch M, Hughes HE: Maxillonasal dysplasia (Binder’s Syndrome). J Med Genet 1990, 27, 384–387.
- Nedev PK: The Binder syndrome: review of the literature and case report. Int J Pediatr Otorhinolaryngol 2008, 72, 10, 1573–1576.
- Dyer FMV, Willmot DR: Maxillo-nasal dysplasia, Binder’s syndrome: review of the literature and case report. J Orthod 2002, 29, 15–21.
- von Binder KH: Dysostosis maxillo-nasalis, ein arhinencephaler Missbildungs complex. Deutsch Zahnaertzl Z 1962, 17, 438.
- Holmstroem H, Gewalli F: Long-term behavior of three different grafts in nasomaxillary reconstruction of Binder syndrome: an analysis by digitalized measurements. Plast Reconstr Surg 2008, 122, 5, 1524–1534.
- Olow-Nordenram M, Valentin J: An etiologic study of maxillonasal dysplasia – Binder’s syndrome. Scand J Dent Res 1988, 96, 69–74.
- Olow-Nordenam M, Radberg CT: Maxillonasal dysplasia (Binder Syndrome) and associated malformations of the cervical spine. Acta Radiol Diagn 1984, 25, 353–360.
- Howe AM, Webster WS, Lipson AH, Halliday JL, Sheffoeld LJ: Binder’s syndrome due to prenatal vitamin K deficiency: a theory of pathogenesis. Austr Dent J 1992, 37, 6, 453–460.
- Gewalli F, Berlanga F, Monasterio FO, Holmstroem H: Nasomaxillary reconstruction in Binder syndrome: bone versus cartilage grafts. A long-term intercenter comparison between Sweden and Mexico. J Craniofac Surg 2008, 19, 5, 1225–1236.
- Cook K, Prefumo F, Presti F, Homfray T, Campbell S: The prenatal diagnosis of Binder syndrome before 24 weeks of gestation: a case report. Ultrasound Obstet Gynecol 2000, 16, 578–581.
- Levailland JM, Moeglin D, Zouiten K, et al. Binder phenotype: clinical and etiological heterogeneity of the so-called Binder maxillonasal dysplasia in prenatally diagnosed cases, and review of literature. Prenat Diagn 2009, 29, 2, 140–150.
- Meier M, Weng LP, Alexandrakis E, Rueschoff J, Goeckenjan G: Tracheobronchial stenosis in Keutel syndrome. Eur Respir J 2001, 17, 3, 566–569.
- Al Kaissi A, Radler C, Klaushofer K, Grill F: Advanced ossification of the carpal bones and monkey wrench appearance of the femora, features suggestive of a probable mild form of desbeqious dysplasia: a case report and review of the literature. Cases J 2009, 13, 2, 1, 45.
- Ziêtek M, Grzebieluch W, Kobierska-Brzoza J, Malicka B, Sk³adnik-Jankowska J: Selected parameters of saliva at Down’s syndrome children – preliminary study. Dent Med Probl 2008, 45, 2, 165–168.
- Kisling E: Cranial morphology in Down’s syndrome. Thesis, Munksgaard, Copenhagen 1966.
- Samdikcioglu M, Molsted K, Kjaer I: The prenatal development of the human nasal and vomeral bones. J Craniofac Genet Dev Biol 1994, 14, 124–134.
- Sheffield LJ, Halliday JL, Jensen F: Maxillo-nasal dysplasia (Binder syndrome) and chondrodysplasia punctata. J Med Genet 1991, 28, 503–504.
- Rude B, Aberg M: Bone Grafts to the Nose in Binder’s Syndrome (Maxillonasal Dysplasia): A Follow-Up of Eleven Patients with the Use of Profile Roentgenograms. Plast Reconstr Surg 1998, 101, 297–304.
- Banks P, Tanner B: The mask rhinoplasty: A technique for the treatment of Binder’s syndrome and related disorders. Plast Reconstr Surg 1993, 92, 1038.
- Delaire J, Tessier P, Tulasne JF, Resche F: Clinical and radiological aspects of maxillonasal dysostosis (Binder syndrome). Head Neck Surg 1980, 3, 105–122.
- Kansu L, Akkuzu B, Avci S: Case report and surgical solution for nasal spine agenesis in a woman with Binder syndrome. Eur Arch Otorhinolaryngol 2008, 265, 847–849.
- Carach B, Woods M, Scott P: Maxillonasal dysplasia (Binder syndrome): a lateral cephalometric assessment. Aust Orthod J 2002, 18, 82–91.
- Buga³a-Musiatowicz B, Szarmach I, Kaczyñska J, Grodzka I: Comparative analysis of dental and skeletal changes in the maxillofacial complex followed by the maxilla deficiency treatment: rapid maxillary expansion and rapid expansion and protraction. Dent Med Probl 2009, 46, 3, 284–290.
- Gupta VK, Utreja A: A different look at treating patient with Binder syndrome. Am J Orthod Dentofac Orthop 2008, 134, 718.
- Cha KS: Skeletal changes of maxillary protraction in patients exhibiting skeletal class III malocclusion: a comparison of three skeletal maturation groups. Angle Orthod 2003, 73, 1, 26–35.
- Bhatt YC, Vyas KA, Tandale MS, Panse NS, Bakshi HS, Srivastava RK: Maxillonasal dysplasia (Binder’s syndrome) and its treatment with costal cartilage graft: A follow-up study. Indian J Plast Surg 2008, 41, 151–159.
- Downarowicz P, Mikulewicz M, Matthews-Brzozowska T: Analysis of morphometric changes following to patients with skeletal class III malocclusion treated with orthodontic method. Dent Med Probl 2009, 46, 3, 301–305.

