
Manuscript accepted on :August 05, 2016
Published online on: --
Balachander, L. Malathi, J. Jenita Jacobina and N. Aravindha Babu
Department of Oral Pathology, Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, Chennai – 600100.
DOI : https://dx.doi.org/10.13005/bpj/1017
Abstract
Gorlin-Goltz syndrome is a rare autosomal dominant disorder with high penetrance and variable expressivity.It involves multiple organ systems.Pathogenesis of this syndrome is attributed to mutations in the PTCH-1gene. Diagnosis of this syndrome is based on major and minor criteria. The most common finding of this syndrome is multiple odontogenic keratocysts in the jaws. Recurrence of this lesion is most characteristic. A case report of33 years male patient with Gorlin-Goltz syndrome is presented here.
Keywords
Calcification of falx cerebri; Gorlin-Goltz syndrome; Odontogenic Keratocyst
Download this article as:| Copy the following to cite this article: Balachander B, Malathi L, Jacobina J. J, Bab N. A. Gorlin-Goltz Syndrome (Nevoid Basal Cell Carcinoma Syndrome)-A Case Report. Biomed Pharmacol J 2016;9(2). |
| Copy the following to cite this URL: Balachander B, Malathi L, Jacobina J. J, Bab N. A. Gorlin-Goltz Syndrome (Nevoid Basal Cell Carcinoma Syndrome)-A Case Report. Biomed Pharmacol J 2016;9(2). Available from: http://biomedpharmajournal.org/?p=8145 |
Introduction
Gorlin-Goltz syndrome, which is commonly known as Nevoid basal cell carcinoma syndrome (NBCCS) is a rare multisystemic disease that is inherited as an autosomal dominant trait.This disorder shows very high level of penetrance and variable expressivity1.Though its occurrence has been observed in ancient Egyptian skeletons of the eleventh Dynastic period, it was Ancell, who in 1841 first reported this syndrome in a patient with multiple benign cysts of the jaw2.In 1894 Jarisch and White presented a case of a patient who had the syndrome, emphasising the presence of basocellular carcinomas3.Later, in 1965 when Gorlin catalogued the related findings of 150 patients andreported multiple nevoid basal cell carcinomas(BCC) of the neck and face, rib and spine anomalies, multiple cysts of the jaw and lamellar calcifications of the falx cerebri as most common manifestations of this syndrome; this condition took on its name as Gorlin syndrome2.The syndrome is also known as multiple basal cell carcinoma syndrome (NBCCS), hereditary cutaneomandibular polyonocosis, multiple nevoid basal cell epithelioma-jaw cysts, or bifid rib syndrome2,4.Pathogenesis of this syndrome is attributed to mutations or micro deletion ofPTCH-1 gene located in the long arm of chromosome- 9. The prevalence of this syndrome is 1 in 50000 to 150000 in general populations though it may vary region wise. Male and female are equally affected3.Asper medical literatures over a period of 34 years (1977-2010), only 17 cases ofNevoid basal cell carcinoma syndrome have been reported from India5.
A case of Gorlin-Goltz syndrome is presented here in which various findings of the syndrome are evident.
Case Report
A 33 year male patient reported to our department with the complaint of painless swelling in the right lower jaw for past one month. The patient also gave a history of multiple jaw surgeries for cyst enucleation in the past. An intra-oral examination revealed thatthe swelling was approximately 3.5×3 cm in size and firm on palpation.
On general examination, the patientwas found to be well built without any apparent facial deformity.
Further evaluation was done with facial bone CT, which revealed a well- defined cystic expansile lesion, measuring 3.7×3.0x2.0 cm with areas of cortical breach involving posterior body and ramus of mandible on the right side.Another well-defined cystic expansile lesion was seen extending on the anterior maxillary alveolus.(Fig 1)
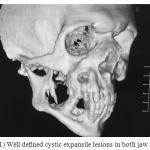 |
Figure 1: Well defined cystic expansile lesions in both jaw
|
Dense calcification was seen in falx cerebri as well as in bilateral tentorium cerebri. (Fig 2)
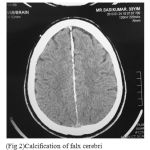 |
Figure 2a: Calcification of falx cerebri
|
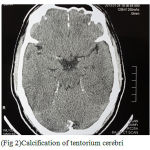 |
Figure 2b: Calcification of tentorium cerebri
|
Considering the possibility of the Gorlin- Goltz syndrome, further evaluation was done with chest radiographs, which revealed an expansile right anterior 4th rib.Mild upper dorsal scoliosis with convexity towards right side was also noticed.(Fig 3)
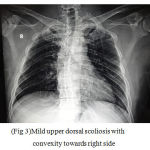 |
Figure 3: Mild upper dorsal scoliosis with convexity towards right side
|
An incisional biopsy of the jaw lesion was done for histopathological examination, which revealed odontogenic lining epithelium of four to five cell layer thickness and fibrous connective tissue stroma.(Fig 4) Basal layer of the lining epitheliumwas composed of palisading columnar cells. Detachment of epithelium from the connective tissue was observed in few areas.(Fig 5) These findings confirmed those jaw cysts were odontogenic keratocysts.
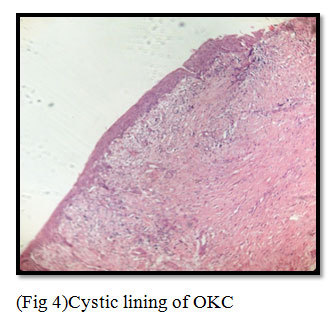 |
Figure 4: Cystic lining of OKC
|
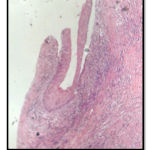 |
Figure 5: Epithelial split in OKC
|
Discussion
Pathogenesis of this syndrome is attributed to mutations or micro deletion of PTCH-1 gene located in the 9q22.3–q31 chromosome1,6.PTCH-1gene is a tumor suppressor gene thatprovides instruction to form a receptor protein called patched-1.Into this receptor protein Sonic Hedgehog ligand fits like keys into lock. The protein patched-1 blocks cell proliferation as long as Sonic Hedgehog ligand is attached within it.
Due to mutation of this gene, production of patched-1 gets prevented or an abnormal version is produced. As a result, uncontrolled proliferation of cells takes place.The oncogenic potential in nevoid basal cell carcinoma syndrome can be explained by Knudsons2 -hit hypothesis theory. According to this hypothesis, normal cells require 2 mutagenic hits to produce cancer. Patients with Gorlin-Goltz syndrome have a germ line defect either on one of the two copies of this specific gene. If loss of the normal remaining allele or second injury happens, the cell may become malignant, as these changes act as second hit4,5.
Though Gorlin syndrome shows a high level of penetrance, great variability in its expressivity is noticed, and no single component is present in all patients.
The most common and significant features include6
50 % or greater frequency
Multiple basal cell carcinomas
Odontogenic keratocysts (OKC’s)
Epidermal cysts of the skin
Palmar/plantar pits
Calcified falx cerebri
Enlarged head circumference
Rib anomalies (splayed, fused, partially missing, bifid)
Mild ocular hypertelorism
Spina bifida occulta of cervical or thoracic vertebrae
15%to 49% frequency:
Calcified ovarian fibromas
Short fourth metacarpals
Kyphoscoliosis or other vertebral anomalies
Pectus excavatum or carinatum
Strabismus (exotropia)
Less than 15% frequency (but not random):
Medulloblastoma
Meningioma
Lymphomesenteric cysts
Cardiac fibroma
Fetal rhabdomyoma
Marfanoid build
Cleft lip and /or palate
Hypogonadism in males
Mental retardation
In order to make a diagnosis of the Gorlin-Goltz syndrome, diagnostic criteria should be taken into consideration. The diagnostic criteria for nevoid BCC were established by Evans et al. and modified by Kimonis et al. They divided the diagnostic criteria as major criteria and minor criteria.To establish a positive diagnosisof nevoid basal cell carcinoma syndrome two major or one major and two minor criteria should be satisfied4,5,7.
Kimoni et al’s major and minor criteria for diagnosis5
Major criteria
Multiple (More than 2) BCCs or 1 younger than 20 years.
Odontogenic keratocysts of the jaws proven by histopathology.
Three or more palmar or plantar pits.
Bilamellar calcification of the falx cerebri.
Bifid, fused or markedly splayed ribs.
First-degree relatives with NBCCs.
Minor criteria
Macrocephaly after adjustment for height.
Congenital malformation:
Cleft lip or palate,frontal bossing, “coarse face,” moderate or severe hypertelorism.
Other skeletal abnormalities:
Marked pectus deformity, marked syndactyly of the digits.
Radiological abnormalities: bridging of sella turcica, vertebral anomalies, such as hemivertebrae, fusion or elongation of the vertebral bodies, modeling defecta of the hands and feet, or flame-shaped lucencies of the hands or feet.
Ovarian fibroma
Medulloblastoma
In our case the patient had multiple odontogenic keratocysts in the jaw,calcification of the falx cerebri, calcification of tentorium cerebri, expansile rib and scoliosis. Presence of these findings confirm our case to be a case of the Gorlin-Goltz syndrome.
Though less than10% of people with multiple OKCs have other manifestations of this syndrome,it has been suggested that multiple OKCs alone may be confirmatory finding for this syndrome.The term “multiple cysts”denotes the occurrence of cyst over lifetime of the patient rather than more than one cyst at a particular time3,7,8.
Various authors found significant differences between syndromic keratocyst and solitary keratocysts.
It has been found that syndrome associated OKCs are multiple in number,occurs at an early age with equal frequencies of both jaws, whereas solitary OKCs occur as isolated cysts,in middle or older aged individuals and shows predilection for lower jaw.Recurrence rate is higher in syndromic OKCs(82%) when compared to solitary OKCs(61%)7.
Histopathologically, syndromic OKCs were found to have smaller epithelial height, fewer total and basal nuclei, markedly increased number of satellite cysts, more solid islands of epithelial proliferation, maximum odontogenic rests within the capsule and more mitotic figures in the epithelial lining of the main cavity compared to solitary OKCs.The aggressive behaviour and high recurrence rate of syndromic OKCs is due to higher rate of proliferation of epithelial lining9.
According to Katase et al, heparanase expression can be correlated with the aggressive behaviour of syndromic OKCs10.
Though laboratory tests are not specific for Gorlin syndrome, syndromic patients have high levels of cyclic adenosine monophosphate and impaired phosphate dieresis on parathormone challenge7.
Keratocysts of Gorlin Goltz syndrome should be treated surgically. For recurrent lesion, cyst removal is done with a bone boxing. In this procedure, a layer of bone at the margin of the cyst is removed. This ensures removal of any daughter cysts. Overlying surface epithelium should be excised along with cystic lining to prevent recurrence. In addition,use of Carnoyi’s solution and cryosurgery is advocated7,8.
A patient with Gorlin syndrome should be monitored regularly and a periodic recall is very essential to evaluate potential cyst recurrences, new cyst formation and development of basal cell carcinomas2.
Conclusion
Nevoid basal cell carcinoma syndrome is rare in Indian population or may be unreported. The occurrence of multiple OKCs may be the first and only manifestation. Multiple OKCs may occur a decade before other symptoms and clinical manifestations of the syndrome. Hence a dentist may be the first person to detect this syndrome. As clinical and radiographic features of this syndrome vary in different ethnic groups, a clinician should be well aware of the manifestations seen in Indian population.As reported in our case,multiple OKCs, skeletal anomalies, and calcification of falx cerebri could be helpful in diagnosis of NBCCS in Indian patients5.
References
- Alfio José Tincani; Antônio Santos Martins; Ricardo Gomes Andrade; Edgar José Franco Mello Jr.; Marco Antônio Camargo Bueno, Nevoid Basal-Cell Syndrome: literature review and case report in a family, Sao Paulo Med. J. vol.113 no.3 São Paulo May/June 1995
- Scott H . Rosen, Delayed dental development in a patient with Gorlin syndrome :a case report, AmericanA cademyo f Pediatric Dentistry, -20:5, 1998, 355-358.
- Ashutosh Agrawal, Aditi Murari, Sunil Vutukuri, Arun Singh, Gorlin-Goltz Syndrome: Case Report of a Rare Hereditary Disorder, Case Reports in Dentistry, Volume 2012 (2012), Article ID 475439, 4 pages.
- Lorenzo Lo Muzio, Nevoid basal cell carcinoma syndrome (Gorlin syndrome), Orphanet Journal of Rare Diseases, 2008, 3:32.
- Shalini R. Gupta, Vipul Jaetli, Sujata Mohanty, Rakesh Sharma, Anand Gupta, Nevoid basal cell carcinoma syndrome in Indian patients:a clinical and radiological study of 6 cases and review of literature, Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:99-110.
- Neville, Damm, Allen, Bouquot, Oral and Maxillofacial Pathology,3rd Edition,Saunders Elsevier Inc.
- Ajit Auluck, Setty Suhas, Keerthilatha M. Pai, Multiple odontogenic keratocysts: report of a case, JCDA , www.cda-adc.ca/jcda , September 2006, Vol. 72, No. 7 ,page- 651- 656.
- Chandra Shekar. L , Sathish. R , Beena. S , Sachin Ganeshan, Gorlin Goltz Syndrome, Journal of Dental Sciences and Research Vol. 2, Issue 2, Pages 1-5.
- Shear M. Odontogenic keratocyst: natural history and immunohisto¬chemistry. Oral Maxillofac Surg Clin N Am 2003; 15:377–82.
- Priya Shirish Joshi, Vijay Deshmukh,and Someshwar Golgire , Gorlin syndrome, Dent Res J (Isfahan). 2012 Jan-Mar; 9(1): 100–106.

