
Manuscript accepted on :27-05-2025
Published online on: 09-07-2025
Plagiarism Check: Yes
Reviewed by: Dr. Emmanuel Dike
Second Review by: Dr. Christian Aimé Njeumen
Final Approval by: Dr. Shubham Mahajan
Mansi Butola1 , Bhawna Chhabra2, Abhishek Gupta3, Meenu Chaudhary4, Sanjeev Kumar Shah5, Praveen Kumar6, Neha Kukreti2, Arif Nur Muhammad Ansori7, Ravinesh Mishra8and Vikash Jakhmola9
, Bhawna Chhabra2, Abhishek Gupta3, Meenu Chaudhary4, Sanjeev Kumar Shah5, Praveen Kumar6, Neha Kukreti2, Arif Nur Muhammad Ansori7, Ravinesh Mishra8and Vikash Jakhmola9
1Department of Pharmaceutics, Uttaranchal Institute of Pharmaceutical Sciences, Uttaranchal University, Dehradun, Uttarakhand, India
2Department of Pharmacology, Amity Institute of Pharmacy, Amity University, Noida, Uttar Pradesh, India
3Department of Electrical Engineering, Dr. B.R. Ambedkar Institute of Technology, Sri Vijaya Puram, A and N Islands
4Department of Chemistry, School of Pharmaceutical Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India
5Department of Computer Sciences, Uttaranchal Institute of Technology, Uttaranchal University, Dehradun, Uttarakhand, India
6Department of Chemistry, Himalayan Institute of Pharmacy and Research, Dehradun, Uttarakhand, India
7Deaprtment of Virology and Bioinformatics, Postgraduate School, Universitas Airlangga, Surabaya, Indonesia, Virtual Research Centre for Bioinformatics and Biotechnology, Surabaya, Indonesia
8Department of Chemistry, School of Pharmacy and Emerging Sciences, Baddi University of Emerging Sciences and Technology, Baddi, Solan, Himachal Pradesh, India
9Department of Pharmaceutical Chemistry, Uttaranchal Institute of Pharmaceutical Sciences, Uttaranchal University, Dehradun, Uttarakhand, India.
Corresponding Author E-mail:mansibutola1995@gmail.com
Abstract
The integration of Artificial Intelligence (AI) and neuroscience is transforming our comprehension of the brain, revealing new opportunities in study, diagnosis, and treatment. The article explores how advanced AI methods, including deep learning and neuromorphic computing, are transforming neuroscience by facilitating the analysis of complex brain datasets. This article also seeks to educate healthcare professionals on pertinent topics of AI, that is, machine learning (ML) and deep learning, to explore the development of AI-powered technological innovation, and to clarify how ML can revolutionize the treatment of neurological disorders. This article explores the unsupervised aspects of ML and its possible use in precision neurology to increase patient outcomes. We have talked about various types of current AI, past research, results, advantages and limitations of AI, efficient accessibility, and the future of AI, keeping in view the current burden of neurological diseases. The intelligent device system for tremor monitoring and phenotyping of tremors is intended to improve results of deep brain stimulation. It encompasses uses for the evaluation of fine motor skills, AI-based electroencephalogram analysis for the diagnosis of epilepsy and psychological non-epileptic seizures, outcome prediction of seizure surgeries, detection of patterns of autonomic instability to prevent sudden unexpected death in epilepsy (SUDEP), detection of complex algorithm patterns in neuroimaging to classify cognitive impairment, discrimination and classification of concussion phenotypes, smartwatches to monitor atrial fibrillation to prevent stroke, and prognosis prediction in dementia. These are various situations of experimental uses of AI in the neurology practice. Despite the apparent limitations of AI, the overwhelming consensus among several national researches is that such new technology could improve the prediction of neurological illnesses and, accordingly, should be incorporated into the medical practice. AI enables the examination of medical information for disease prevention, diagnosis, monitoring of patients, and creation of new procedures, as well as assisting doctors in handling large amounts of data with greater accuracy and efficiency.
Keywords
Artificial intelligence; Epilepsy; Neurological disorders; Seizures; Technology
| Copy the following to cite this article: Butola M, Chhabra B, Gupta A, Chaudhary M, Shah S. K, Kumar P, Kukreti N, Ansori A. N. M, Mishra R, Jakhmola V. Artificial Intelligence as an Emerging Technique in the Contemporary Management of Neurological Disorders. Biomed Pharmacol J 2025;18(August Spl Edition). |
| Copy the following to cite this URL: Butola M, Chhabra B, Gupta A, Chaudhary M, Shah S. K, Kumar P, Kukreti N, Ansori A. N. M, Mishra R, Jakhmola V. Artificial Intelligence as an Emerging Technique in the Contemporary Management of Neurological Disorders. Biomed Pharmacol J 2025;18(August Spl Edition). Available from: https://bit.ly/4llPzV6 |
Introduction
AI is now necessary in addressing the challenging problems of neuroscience, a field devoted to knowledge of the complex dynamics of the human brain. Comprising more than 86 billion neurons, the brain is a highly dynamic, non-linear structure with trillion of synaptic connections. Understanding its purposes ranging from basic reflexes to sophisticated cognition requires the study of large amounts of data using modalities including neuroimaging, electrophysiological, and behavioural studies. Although effective in a limited area, conventional analytical methods may overlook the complex, multi-scale patterns seen in brain data.1 This disparity has rendered AI a significant instrument for neuroscientific inquiry. The examination of the structure and cognitive processes of the brain with respect to information processing, judgment, interaction with the environment, and behaviour in terms of the brain is referred to as neuroscience. It connects among other disciplines physiology, anatomy, cytology, molecular biology, psychology, physics, computer science, chemistry, medicine, statistics, and mathematical modeling.2 Neuroscientists investigate the entire nervous system to better understand various neurological, psychiatric, and neurodevelopmental disorders in addition to studying the brain for cognitive function. Neuroscience establishes what aspects of the human nervous system are susceptible to disease, accidents, and disorders to contribute to the design of effective cures.3 It is also important to recognize that advances in neuroimaging technology have significantly enhanced our understanding of brain structure and function. Scientific breakthroughs have been the key driving force for neuroscience development. These advances enabled one to image the brain both at high and low resolutions through enabling the high-resolution examination of genes, chemicals, synapses, and neurons and the low-resolution imaging of the whole brain. Radiologists employed convolutional neural networks in analyzing images using complex reasoning to conduct detection and prediction due to its numerous hidden layers. In addition, beneficial information can be obtained, saved, processed, displayed, and controlled with computer-based neuroimaging methods.4 The hierarchical relationship is given in figure 1.
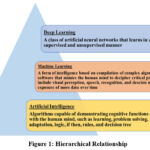 |
Figure 1: Hierarchical Relationship Click here to view Figure |
AI is used in the healthcare industry to analyze medical data to prevent disease, diagnose conditions, monitor patients, and create new practices. However, AI has the potential to alleviate the burden that clinicians are currently experiencing due to the sheer volume of data they are required to manage. Since health care data began to be digitalized in the middle of the 1960s and the American Recovery and Reinvestment Act of 2009 included the electronic health record (EHR), new opportunities are being created by the growing availability and development of analytical tools. Neurological disorders are defined by structural, biochemical, or electrical brain, spinal cord, and nerve abnormalities. As more people age and the population expands, the impact of chronic neurological disorders has increased strongly even as the death rates from stroke and other infectious neurological disorders have receded.5 The most prevalent neurological disorders, such as dementia, stroke, epilepsy, Parkinson’s disease (PD), multiple sclerosis, migraine, and tension-type headache, resulted in an estimated $789 billion economic loss for the US in 2014.6 AI is the fundamental principle of precision medicine, which will ultimately translate to neurological management.7 The treatment and prevention of disease are the focus of this emerging approach, which considers a diverse array of factors, such as heredity, lifestyle, and the environment. It is capable of operating at an unprecedented pace without the necessity of human programming, using substantial quantities of computer power. In every subject, but especially in neurology, the future of AI appears encouraging. The future seems bright, from the prediction of seizure disorder outcomes to the classification of brain tumors, the improvement of neurosurgical techniques, the rehabilitation of stroke patients, and the tracking of patient symptoms and advancement via smartphone applications.
The principal aim of the present review is to bring attention to the recently developed AI technologies that are revolutionizing the management of neurological diseases and improving the overall functional outcome of the patients. We have established the numerous forms of AI that are utilized and available presently, along with the prevalence of neurological disease. We have also elaborated on past research, findings, benefits, and shortcomings of AI and its potential future and useful accessibility.
Artificial intelligence technology types and their applications
The implementation in clinical practice has been challenging, despite the extensive research that has contributed to the diagnosis of a wide range of disorders. Smartwatches, smartphones, and tablets are among the smart devices that researchers are employing to classify and identify complex movement disorders and arrhythmias, including atrial fibrillation. Moreover, these gadgets are used to improve medication adherence in patients under anticoagulant treatment and forecast aspiration pneumonia in subjects with swallowing difficulties caused by stroke and dementia.8 To establish differential diagnoses and treatment regimens for rare epilepsy diseases, smart devices with wrist-mounted sensors are being used by epileptologists to recognize seizure activity and iPads with AI functionality. ML has great promise for bridging the gap between accurate clinical diagnosis and the translation of important clinical data. Table 1 illustrates the various AI technologies and their respective applications.
Table 1: Enumerates many AI technologies and their therapeutic applications in neurological diseases
| Type of models | Description | Uses | Reference |
| Smart Devices | these wearable gadgets track swallowing and evaluate proficiency. | analyse, and visualize swallowing skills in stroke and advanced Alzheimer’s patients, reducing aspiration pneumonia. | 9 |
| Frideswide AIalgorithm | it analyses clinical data, reports, communications, and requests. | Used to facilitate the rapid diagnosis of frontotemporal dementia | 10 |
| Imaging Services | classifies Magneticresonance imaging (MRI) and CT images by clinical information and severity. | Assists in the rapid and effortless assessment of imaging | 11 |
| Epifinder AIintegrated application | Its goal was to help identify and classify rare epilepsy, triage decision-making, and find better treatments. | By contrasting the aggregate composite of symptoms with the knowledge representation of the ILAE guideline, the program generates a list of differential diagnoses for epilepsy syndromes. | 12 |
| Health applications (MEDITECH MHealth, VizAI) | This software analyse CT images, identify stroke indications, and interact with neurologist. | These applications serve as essential for stroke patients since they reduce the treatment time, hence improving outcomes. | 9 |
| Smartwatches | Each test analyzes and infers tremor amplitude and frequency from accelerated wearable data to help diagnose movement disorders. | AI diagnoses various movement disorders and captures high-resolution tremors, then transfers the results to the examiner’s smartphone. | 13 |
| ML integrated with handheld electrocardiography (ECG) | The portable Electrocardiogram (ECG) sensor device consists essentially of an external ECG component mobile phone app. | Many arrhythmias, such as atrial fibrillation, anomalies of the ST segment, atrial flutter, bundle branch blockages, atrial and ventricular premature pulses, can be detected with handheld ECGs. | 14 |
| Tablet baseddevice | During the neurological test, a two-minute iPad examination is used to gauge patient pressure and Archimedean spiral sketching. | The diagnosis of different movement illnesses will be predicted using the sum of all the data. | 13 |
| Augmented EEGs learning | the machines use many models including support vector machines (SVM), power spectrum, independent component analysis (ICA) | Predicting the prognosis of epilepsy surgery using AI by evaluating clinical, pathological, and cognitive aspects among other elements. | 15 |
| Mobile phone-based photoplethysmography (PPG) | This optical technique uses light absorption and skin color analysis to identify heartbeats. | For the paramedics, considerably the stroke team, mobile device-oriented PPG makes it easier to detect heart rate, atrial fibrillation, heart rate variability. | 14 |
| Smartphone | patients’ demographics, medical and family history, drug usage, and non-motor symptoms is integrated into the Apple-based smartphone application. | aids in the classification and stratification of tremor. | 13 |
Since random forest methods apply neuroimaging information in small sample sizes with large-dimensional parameter spaces, they are more robust compared to other algorithms. They have been successful in the classification of dementia, including mild cognitive impairment (MCI)16 and Alzheimer’s,17 as well as in other conditions like psychogenic non-epileptic seizures (PNES),16 PD ,18 and schizophrenia. Similar disorders, like dementia, have been classified using a similar algorithm. To recognize different phenotypes in patients with concussions, a team of researchers has implemented the algorithms of the self-organizing map. To create more effective stroke treatment tools, clinicians have started using deep learning algorithms to predict and detect the time since stroke onset (TSS).10 In adult patients who experience episodes, Epifinder algorithms help in the diagnosis of seizures. These instruments may help in the identification of disorders and prevent the delay of diagnosis and treatment.12 Table 2 provides a comprehensive list of studies that have implemented AI in the field of neurocare.
Table 2: Lists of prior studies that have employed AI in neurological care
| Clinical condition | Sample size and timeline of study | Results | Reference |
| Ischemic stroke | 181 patients | The best classifier outperformed earlier methods, according to cross-validation, with an AUC of 0.765, sensitivity of 0.788, and negative predictive value of 0.609. | 9 |
| Temporal lobeepilepsy (TLE) | 21 patients with TLE, 21 with control | Fisher’s linear discriminant analysis (FLDA) identified 3/42 patients correctly with 73.8% accuracy, 81.0% sensitivity, and 66.7% specificity. | 15 |
| PD and essentialTremor (ET) | 120 patients of ET, 954 patients of PD followed by 21 months | Validates smart wearable medical usage, provides deeper tremor understanding. | 13 |
| Psychogenic nonepileptic seizures (PNES) | There were 23 patients with PNES and a 21-patient age-adjusted control group. | PNES is predominant in the limbic and motor inhibition systems and has a mean accuracy of 74.5% compared to controls. | 19 |
| Sports related concussion syndrome | 212 patients | Group (n=38) and group 2 (n=58) were the numbers. Notably, group 1’s caloric summary score at the maximum slow phase along was 30.7% lower than group 2’s. |
20 |
| Epilepsy | 57 patients from January to June 2017 | In comparison to video EEG, Epi Finder performs with 86.8% accuracy, 86.4% sensitivity, and 85.1% specificity. | 12 |
| Frontotemporal dementia (FTD) | 47 patients | FwA helps diagnose FTD clinically, deviating 7.37 times from the standard range. | 10 |
Tumours
The most common way to detect a brain tumor is via an MRI scan. Tumor identification, segmentation, and grade estimation are the three primary uses of machine and deep learning approaches in MRI imaging. A survey clearly identified four categories of brain tumor segmentation and classification methods: classic ML approaches, image transformer-based methods, capsule neural network-based methods, and convolutional neural networks (CNN)-based methods.21 Several ML techniques, such as histogram-oriented gradient, gray-level co-occurrence matrix, and first-order statistical feature extraction, use texture information to classify tumors. A study proposed a multigrading brain tumor classification system based on CNN proposes a variety of deep CNNs that rely on user-defined hyperactive values to classify brain tumors introduces multiscale grade estimation via 3D multilayer neural networks. Still, picture rotations affect the accuracy of CNN, despite its successful use in brain tumor analysis. Moreover, CNN required a substantial amount of training data. Capsule neural network-based approaches addressed these two problems. CNNs are incapable to record the long-range information inherent in temporally consecutive picture sequences because to their limited kernel size. Nonetheless, vision transformer (ViT) neural networks can effectively handle these sequences.22,23
Epilepsy
Misdiagnosis rates range from 20 to 40 percent in general settings and 26 percent in epilepsy centres due to a variety of clinical abnormalities. This frequently results in pointless inquiries and actions. Applications of ML involve its diagnosis, psychogenic non-epileptic seizures (PNES), and novel epilepsy subtypes, as well as prophylaxis of SUDEPECG and decreasing inter-observer variability in EEG interpretation. Although there are no visible interictal epileptiform discharges on the EEG, ML-detected alterations in microstate C with 76.1% accuracy indicate a possible misactivation of alpha activity. Rajagopalan et al., 24,25 showed that instead of using ictal or interictal variations in replicated scalp EEG, can classify temporal epilepsy by detecting microstate changes which are affected by pharmacological drugs, sleep deprivation, and observer variability etc. The Epifinder algorithm at a tertiary centre effectively generated a differential diagnosis of seizure types and epileptic syndromes from other events. Early investigation with wristband sensors showed more electrodermal activity (EDA) during epileptic seizures. Relative to complex partial seizures (CPS), generalized tonic-clonic seizures (GTCS) presented with a highly increased EDA. Comparable findings were recorded by Van Buren (1958), and increased plasma level of catecholamines prior to GTCS supported it. They suggest that the autonomic instability of sympathetic surges during episodes of seizures may contribute to SUDEP.
Seizure
Epileptic seizures arise from an unpredicted, abnormal increase in electrical activity in the CNS, and their identification is difficult owing to the variety of their patterns. This research used ML methods to examine electroencephalography recordings for the efficient detection of seizures. The characteristics from EEGs were obtained via discrete wavelet processing and K-means clustering that were analysed via machine learning program to detect seizures. Methods use local neighbor’s descriptive patterns and 1D local gradient patterns, as used in for feature extraction. The collected properties were further analysed using an artificial neural network to detect seizures. Likewise, articles pertain to the automated identification of seizures. Unlike the approaches that extract features from single-channel EEG data, used automated feature extraction by merging a 2D deep multilayer autoencoder with a neural network to categorize the retrieved features for seizure identification in children.26
Stroke
In the US, stroke ranks as the fifth most common cause of death and the primary cause of disability. A new or recurrent stroke affects 795,000 Americans annually, resulting in direct medical costs of about $24 billion. Intravenous thrombolytic treatment is administered to 5% or less of patients, despite its essential role in tissue preservation during acute ischemic stroke. This can result from inadequate medical expertise in administering thrombolytics, a 6% haemorrhagic risk linked to thrombolytics, patients in isolated areas lacking sufficient services, and strokes that are undetected, occur upon waking.27 Consequently, it is essential to improve therapy and advance technology to tackle this complex issue and mitigate increasing expenses. Within a year after a transient ischemic attack (TIA) or mild stroke, ML has demonstrated its capacity to forecast the risk of recurrent stroke, while estimating the duration since the onset of the stroke. It works better for people with indeterminate TSS (wake-up strokes or unwitnessed strokes) than the current DWI–FLAIR mismatch, helping healthcare providers in developing more effective treatment strategies.4 To help prevent embolic stroke, smart devices that use photoplethysmography and more accurate portable electrocardiograph recorders are used to monitor heart rate, as well as to detect asymptomatic atrial fibrillation and heart rate variability.28
Developmental and Intellectual Disabilities
Attention-deficit/hyperactivity disorder, cerebral palsy, Down syndrome, autism spectrum disorders, fragile X syndrome, and other intellectual and developmental disabilities sometimes occur in children under the age of 18. Neuroimaging, genetic, genomic, electronic health record, clinical, and behaviour data obtained using a variety of approaches are some of the multimodal inputs required to examine intellectual impairment (ID) and developmental disability. In kids it is determined by examining neuroimaging information based on a DNN. Schizophrenia SCZ has been recognized by a deep neural network with the evaluation of functional connectivity patterns in fMRI information. FMRI data has been evaluated here to recognize autism using a deep neural network in terms of autoencoders.29 An SVM algorithm was applied in to analyze EEG data to identify children’s attention-deficit/hyperactivity problems. Other medical records, such as circulatory, endocrine, metabolic, and genitourinary variables, are associated with fragile X syndrome. This faith has led to the creation of AI-augmented screening instruments that scan individuals’ electronic health data to identify fragile X syndrome. In terms of sensitivity and specificity measures, the random forest approach surpassed K-nearest neighbors, support vector machines, backpropagation, and deep learning in the classification of autism spectrum disorders (ASDs) among children and adolescents.30 High-risk children can receive focused testing if ASDs are detected early on. ML can detect ASDs by studying a toddler’s gaze patterns. ASD detection is also improved by using a ML strategy that is dependent on maternal auto-antibody markers and blood testing.
Concussion
Concussion is a multifaceted challenge without conventional diagnostic criteria, leading to differences among examiners. The clinical presentation encompasses several cognitive and non-cognitive domains, such as sleep and balance. Prior research has focused on imaging, symptoms, and psychological assessments, despite the varied symptomatology. ML has effectively differentiated between concussed and control participants, improving diagnosis with individual data that includes traditional imaging, clinical presentation, eye movement, cognitive domains. Additionally, it has enabled the investigation of complex and poorly understood pathologies, like vestibular impairments, which has improved understanding and recognition of a variety of phenotypes, such as headaches, cardiovascular and vestibular abnormalities, oculomotor dysfunction, affective disorders, cervical spine conditions, and cognitive deficits.31
Dementia
Twenty percent of young-onset dementia is frontotemporal dementia (FTD), a neurodegenerative illness with a higher risk of misdiagnosis. This frequently results in less patient satisfaction and well-being, needless imaging, lab work, and clinic visits, as well as higher healthcare expenses. It has a lower life expectancy and the poorest prognosis when compared to other dementias. According to UK research, by improving clinical practice standards, deep learning algorithms may minimize needless investigations, maximize expenses, and improve patient satisfaction.32
Challenges and Limitations
Although AI is revolutionizing the fields of neuroscience and healthcare, its implementation presents a multitude of obstacles that necessitate mindful solutions.33 To completely realize the transformative potential of AI, it is important to address a variety of obstacles, including ethical concerns, technical constraints, and data quality and interpretability
Data Ethics
The core domains of data ethics, which support AI, are informed consent, transparency, privacy and data protection, impartiality, ownership. Can we assign monetary values to our own health data? Unfortunately, data exchanges of this kind are prevalent; for example, the Royal Free London Foundation Trust and DeepMind engaged in data sharing. This vast collection of personal health data belongs to whom? According to Canadian regulations, the “information custodians” of patients’ confidential health information are medical professionals. while individuals are true proprietors of information. This “guardianship” serves as proof that patients’ medical records are protected by legal interests. Therefore, patients possess the authority to scrutinize the procedures and use their recordings and personal health data, since they are the proprietors of this information.34
Legal issues
The recruitment of healthcare professionals is dependent upon the successful completion of rigorous evaluations, and they must comply with established rules of behaviour in their everyday practices. At now, there are no universally standardized legislation or regulations governing the conduct of practitioners in the implementation of AI in healthcare. AI-crime, an innovative and harmful violations, may arise if criminals use AI. Consequently, it is imperative to implement thorough and extensive AI legislation. However, we must consider many considerations. The formulation of such legislation will not rest only with legal specialists. Stakeholder contributions are essential for the creation or development of AI-based therapeutic solutions. Secondly, it is essential to identify the proper person responsible for AI-related infringement, whether it be the AI maker, user, or maintenance. What is the scope of each stakeholder’s responsibility? What proportion of responsibility should be assigned to doctors in complicated cases, rather than necessitating that they bear each risk involved with AI medical treatment? At the end, it is essential that we continually improve the existing legislation. Research has shown that health-related data has greatly surpassed the initial objectives of privacy protection regulations, such as the Health Insurance Portability and Accountability Act (HIPAA) passed by the US Congress in 1996. We are lucky to see the introduction of many new regulations that regulate the preservation of AI data, the attribution of duty, and oversight.35
Hardware Security
At now, a range of electronic equipment, like as computers, mobile phones, and gadgets, is required for the operation of all AI products. Three significant problems about the security of this system must be addressed. Initially, extrinsic variables like as electromagnetic interference, temperature variations, and cost will impact even the most physically unclonable operations. Second, the intricacy and proficiency of medical knowledge and information technology hinder engineers’ and doctors’ attempts to adopt AI that incorporates many technologies. Engineers must receive retraining to access and handle data from medical systems. Failure to do so may cause data leaks and disrupt medical workflow. However, doctors may not fully comprehend the workings of AI products in practice, which could lead to a decrease in productivity and an increase in errors. Third, the security concern with AI networks must be addressed. A global cascading effect could be triggered by a malfunction or attack on critical nodes in the intricate transmission network.36
Software Security
Even algorithmic computing methods with strong features are extremely vulnerable to design attacks. Although the AI system worked outstandingly well in the initial design test, its performance is often inadequate in a targeted design conflict. If the attacker had complete knowledge of the trained neural network model, such as training data, model structure, hyperparameters, number of layers, activation function, and model weights, then each phase of the AI algorithm development process would be in jeopardy. System classification uncertainty may result from false-positive attacks that generate a negative sample or false-negative attacks that generate a positive sample. The target model’s architecture, parameters, or training dataset is not necessarily known by the attacker. Despite intervention from outside the system and prevention efforts, system faults can occur internally as well. Because autonomous updates are subject to faults, loss of data, and variability of illness trends, the initial solution will continue to deviate progressively from track.37
Fairness
The primary ethical issue is the pervasiveness of bias in data sources. When it comes to sociological, environmental, or economic issues, gender, sexual orientation, or race, all data sets will exhibit bias to varied degrees. Current data is used to create AI algorithms that learn and offer relevant insights. Historical data has shown demonstrated bias in healthcare, and machine learning models derived from this data may exacerbate these disparities. According to US research, physicians may have disregarded good results for African Americans because they believed the model had limited predictive value for this group. The limited participation of African Americans in the initial trial led to the low positive rate, increasing the likelihood of false-positive results. Injustices can also arise in the creation, application, and assessment of models. For patients displaying specific signs, such extremely preterm birth or neurological impairment, clinicians always stop treatment. AI assimilates the variations in human interests, possibly leading to substantial moral issues that might adversely affect patients. That idea will overlook those in poor areas who endure lengthy medical visits owing to financial limitations or significant distances. The method might unjustly give patients from affluent areas access to case management resources. The practical application of AI may be restricted by the existence of automated differences. AI discoveries based on complex characteristics that are unknown to humans exacerbate the problem. By neglecting to challenge these findings, the lack of local specialists in areas with limited resources may make automation bias more dangerous.38
Possible Solutions
Artificial Intelligence-driven ecological network
AI algorithms for clinical application emerge from a complicated process that starts with the first collection of complex clinical data or incidents. We provide a publicly accessible big data sample database that integrates the complete ecological network, using AI. The framework offers a thorough explanation of all the relationships that AI produces and the concerns that need consideration. It may be categorized into three separate stages.
The preliminary phase (preclinical) as shown in figure 2, aims to discover significant issues from clinical research or large data sample repository. An initial algorithm will be developed by collecting data and technical progress, and it will then be evaluated using a specially developed attack software. The public big data sampling library will simulate and implement the algorithms that withstand scrutiny to discover AI applications that are authentically safe and reliable.39
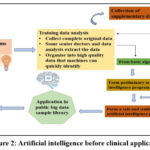 |
Figure 2: Artificial intelligence before clinical application Click here to view Figure |
The second phase is clinical application; shown in figure 3 the execution of small-scale clinical applications is feasible after a series of evaluation processes. The algorithm’s use and optimization procedures are outlined, followed by the implementation of a large-scale clinical application. Ultimately, a clinically viable AI algorithm is constructed for real-world use.40
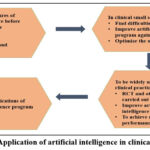 |
Figure 3: Application of artificial intelligence in clinical practiceClick here to view Figure |
As seen in figure 4, we combine high-quality data sets and safely extract them using big data, blockchain, and other technologies in the third phase (creation of a public large data sample database). The huge data sample database must be regularly updated and maintained daily. This includes managing its data storage state, data security, and other features. The AI program goes through another verification step after the database update. If the software contains errors or does not satisfy the necessary requirements, re-debugging is necessary. A specialized supervising department is also necessary to keep an eye on the entire procedure and offer suitable complaint channels for prompt problem solving.41
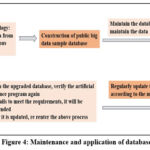 |
Figure 4: Maintenance and application of databaseClick here to view Figure |
Case Studies
Case Study 1: AI-Assisted Stroke Identification and Therapy Enhancement
A 65-year-old man who was experiencing stroke symptoms showed up at the emergency room. The hospital had installed Viz.ai, an AI-powered imaging system, in place of time-consuming traditional diagnostic techniques. In a matter of seconds, the AI identified a major vascular occlusion in the patient’s CT scan and warned the stroke team. The patient’s impairment was greatly decreased by the prompt mechanical thrombectomy that followed this early identification. He recovered his mobility in a matter of weeks, demonstrating the significant improvement in stroke outcomes that AI-assisted diagnostics may provide.42
Case Study 2: AI-Enhanced EEG Analysis for Early Epilepsy Detection
Anxiety was first mistakenly recognized as the cause of recurrent fainting episodes in a 10-year-old girl. An AI-integrated EEG system, however, picked up on tiny seizure patterns that traditional readings would have missed. Doctors looked at these anomalies further after the AI identified them as possibly being focal epilepsy. Because of the early diagnosis, she was able to get customized anti-epileptic drugs, which significantly decreased the frequency of her seizures and enhanced her quality of life. This instance demonstrates how AI can improve diagnosis and avoid protracted suffering due to incorrect diagnoses.43
Case Study 3: Using Smartwatches to Manage Parkinson’s Disease Symptoms
With PD, a 55-year-old lady experienced erratic tremors and trouble scheduling her medicine. An AI-powered motion monitoring smartwatch tracked her movements continually and detected patterns of tremor. Her neurologist was able to improve symptom control by adjusting her medication regimen and dosage thanks to the AI-generated reports. Her tremors subsided considerably in a matter of months, restoring her independence in day-to-day tasks. This illustrates how customized treatment regimens are improved by wearable AI technology.44
Case Study 4: Surgical Precision and AI-Assisted Brain Tumor Diagnosis
An MRI scan of a 42-year-old guy who had been experiencing headaches for a long time showed what appeared to be a tumor. The scans were evaluated using AI-assisted imaging software, which accurately distinguished between benign and cancerous areas. By using this knowledge, neurosurgeons were able to plan a minimally invasive procedure that would remove cancerous tissues while maintaining vital brain processes. AI-powered rehabilitation programs helped him recover cognitively after surgery, hastening his return to work. This instance demonstrates how AI affects post-operative care and surgical accuracy.45
Case Study 5: Using ML to Forecast the Course of Alzheimer’s Disease
AI-powered cognitive tests that examined speech patterns and brain scans were performed on a 72-year-old lady who had mild memory problems. The ML model suggested early pharmacological and lifestyle therapies and indicated a high probability of Alzheimer’s development. Her cognitive decline was considerably slowed using AI-monitored therapy and systematic cognitive training, enabling her to continue living an active lifestyle for several additional years. AI’s ability to change neurology care toward proactive disease management is demonstrated by this case. 46
Emerging AI Technologies in Neuroscience
Brain-Computer Interfaces (BCIs) for Communication and Mobility Recovery
By facilitating direct connection between the brain and external equipment, brain-computer interfaces, or BCIs, are transforming the field of neuroscience. Neuralink’s high-resolution implant, which enables paralyzed people to operate computers and robotic limbs with just their thoughts, is a noteworthy innovation. A quadriplegic patient recently regained their sense of independence by using a BCI system to play video games and type letters. Through thought-driven text production and movement aid, developments in AI-driven BCIs are also enhancing the quality of life for patients who are confined and facilitating communication.47
Prosthetics Driven by AI for Neural-Controlled Limb Motion
By decoding neural signals and translating them into precise movements, AI integrated prosthetic limbs are revolutionizing amputee mobility. Researchers have created AI-powered myoelectric prosthetics that employ ML to adjust to the user’s will. The LUKE Arm is one such invention that uses sensors to identify muscle activation and convert it into organic hand motions. An AI-powered prosthetic helped a patient who lost his arm in an accident regain near-natural dexterity, enabling him to carry out difficult activities including playing musical instruments and gripping delicate objects.48
Neural Decoding in Real Time for Predicting Seizures
Patients with epilepsy may now forecast seizures in real time thanks to AI-powered neural decoding technologies. Early warnings before an episode happens are made possible by ML models that examine EEG signals to detect pre-seizure activity. To avoid seizures, devices such as NeuroPace’s RNS System continuously monitor brain activity and provide focused electrical stimulation. Patients in clinical studies reported a 60% decrease in seizure frequency, proving AI’s capacity to treat neurological conditions in real time.
Using Quantum Computing to Perform More Complex Brain Analysis
By analysing enormous neurological datasets at previously unheard-of rates, the nexus of quantum computing and AI has the potential to completely transform neuroscience. Quantum algorithms are better able to manage the non-linear dynamics of the brain than traditional AI models, which find it difficult to simulate whole neural networks. IBM and Google researchers are investigating quantum-enhanced ML to speed up brain mapping, which could lead to the development of novel therapies for neurodegenerative illnesses. Future uses might involve real-time brain function simulation and extremely quick medication development for neurological conditions, which could result in advances in customized treatment.
Future Perspectives
A skilled method for enhancing the quality of life for those with tremors, such as those with PD and essential tremor (ET), is deep brain stimulation (DBS). Since a neurologist currently evaluates DBS leads, individual variability may have an impact. AI could be useful in this situation by facilitating an unbiased assessment, if it complies with legal requirements and obtains medical authorization. 49 Traditional audits and statistics are confined to assessing predetermined hypotheses; however, modern algorithms may rapidly assess several hypotheses and generate a priori assumptions beyond human capability. This has potential applicability across various diseases and specializations. ML can analyze large datasets with enhanced speed and precision to investigate enigmatic phenomena.47 To increase the validity of research within a more complicated framework, non-vestibular factors, such as prior concussions, neuropsychological outcomes, and other variables, may be included into ML approaches, such as self-organizing maps (SOM). By finding traits in different patient populations, this also helps to improve diagnostic criteria. The advancement of data standards and intelligent gadgets is optimally facilitated using open data portals. To facilitate their replication in later research, some scholars have released study models, frameworks, algorithms, and anonymized data samples open source.50 Their use is increased by publicly available, reasonably priced devices with customizable apps. The first FDA-approved ECG reader for smartwatches is the Kardiaband app from AliveCor.
Conclusion
The. present neurologic care system burdens the US economy with increased overall cost and a detrimental impact on disability-adjusted life years. The capacity of AI and ML to process medical information in the avoidance of disease, diagnosis, tracking of the patient, and the development of new procedures will benefit physicians in the management of huge amounts of data with. more precision and rapidity. AI will not replace doctors. Usage of AI will not be harmful to physicians, and biochemical analysers will not turn into substitutes for laboratory specialists. Rather, it will compel the physician to reframe the role of the physician. The topic of disease and its etiology and pathogenesis must be of concern to the research in AI and not so much precision and sensitivity in the report. These researches will also play the role of broadening our perception regarding biology. AI can reduce interobserver variations, detect asymptomatic atrial fibrillation, diagnose epilepsy, psychogenic non-epileptic seizures (PNES), concussion, and movement disorders, and detect faulty autonomic function to avoid sudden unexpected death in epilepsy (SUDEP). AI use is limited owing to a variety of reasons such as physicians’ reluctance to adopt it. State-of-the-art technology, billing, and reimbursement concerns, pan USA license complications, malpractice litigation, and the up-front expense of technology implementation can render it a powerful means for neurological therapy.
Acknowledgment
The authors expressed their gratitude to Mr. Jitender Joshi, President and Prof. (Dr.) Dharam Buddhi, Vice Chancellor of Uttaranchal University Dehradun, for their encouragement and guidance in publishing this review work.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Author contributions
Mansi Butola and Bhawna Chhabra: Data collection and manuscript
Meenu Chaudhary, Praveen Kumar, Vikash Jakhmola, Neha Kukreti, Arif Nur Muhammad Ansori, Sanjeev Kumar Shah, Abhishek Gupta and Ravinesh Mishra: Reviewed and corrected
References
- Hassabis D, Kumaran D, Summerfield C, Botvinick M. Neuroscience-Inspired Artificial Intelligence. Neuron. 2017;95(2):245-258.
CrossRef - Sautha V, Butola M, Chaudhary M, et al. Overview of 3D Printing Technology with Pharmaceutical Applications, Challenges and Future Aspects. Biomed Pharmacol J. 2025; 18:17-32.
CrossRef - Pantelopoulos A, Bourbakis NG. A survey on wearable sensor-based systems for health monitoring and prognosis. IEEE Trans Syst Man Cybern C Appl Rev. 2010;40(1):1-12.
CrossRef - Henricks WH. “Meaningful use” of electronic health records and its relevance to laboratories and pathologists. J Pathol Inform. 2011;2(1):7. doi:10.4103/2153-3539.76733.
CrossRef - Murray CJL, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197-2223.
CrossRef - Gooch CL, Pracht E, Borenstein AR. The burden of neurological disease in the United States: a summary report and call to action. Ann Neurol. 2017;81(4):479-484.
CrossRef - Mesko B. The role of artificial intelligence in precision medicine. Expert Rev Precis Med Drug Dev. 2017;2(5):239-241.
CrossRef - Varghese J, Niewöhner S, Soto-Rey I, et al. A smart device system to identify new phenotypical characteristics in movement disorders. Front Neurol. 2019; 10:48.
CrossRef - Ho KC, Speier W, Zhang H, Scalzo F, El-Saden S, Arnold CW. A machine learning approach for classifying ischemic stroke onset time from imaging. IEEE Trans Med Imaging. 2019;38(7):1666-1676.
CrossRef - Brzezicki MA, Kobetić MD, Neumann S, Pennington C. Diagnostic accuracy of frontotemporal dementia: An artificial intelligence-powered study of symptoms, imaging, and clinical judgement. Adv Med Sci. 2019;64(2):292-302.
CrossRef - Chan KL, Leng X, Zhang W, et al. Early identification of high-risk TIA or minor stroke using artificial neural network. Front Neurol. 2019; 10:171.
CrossRef - Okazaki EM, Yao R, Sirven JI, et al. Usage of EpiFinder clinical decision support in the assessment of epilepsy. Epilepsy Behav. 2018; 82:140-143.
CrossRef - Varghese R, Shringi H, Efferth T, Ramamoorthy S. Artificial intelligence driven approaches in phytochemical research: trends and prospects. Phytochem Rev. 2025:1-16.
CrossRef - Li KH, White FA, Tipoe T, et al. The current state of mobile phone apps for monitoring heart rate, heart rate variability, and atrial fibrillation: narrative review. JMIR Mhealth Uhealth. 2019;7(2): e11606.
CrossRef - V KR, Rajagopalan SS, Bhardwaj S, et al. Machine learning detects EEG microstate alterations in patients living with temporal lobe epilepsy. Seizure. 2018; 61:8-13.
CrossRef - Sarica A, Cerasa A, Quattrone A. Random Forest algorithm for the classification of neuroimaging data in Alzheimer’s disease: a systematic review. Front Aging Neurosci. 2017; 9:329.
CrossRef - Rathore S, Habes M, Iftikhar MA, Shacklett A, Davatzikos C. A review on neuroimaging-based classification studies and associated feature extraction methods for Alzheimer’s disease and its prodromal stages. Neuroimage. 2017; 155:530-548.
CrossRef - Amoroso N, La Rocca M, Monaco A, Bellotti R, Tangaro S. Complex networks reveal early MRI markers of Parkinson’s disease. Med Image Anal. 2018; 48:12-24.
CrossRef - Vasta R, Cerasa A, Sarica A, et al. The application of artificial intelligence to understand the pathophysiological basis of psychogenic nonepileptic seizures. Epilepsy Behav. 2018; 87:167-172.
CrossRef - Visscher RMS, Feddermann-Demont N, Romano F, Straumann D, Bertolini G. Artificial intelligence for understanding concussion: Retrospective cluster analysis on the balance and vestibular diagnostic data of concussion patients. PLoS One. 2019;14(4): e0214525.
CrossRef - Titano JJ, Badgeley M, Schefflein J, et al. Automated deep-neural-network surveillance of cranial images for acute neurologic events. Nat Med. 2018;24(9):1337-1341.
CrossRef - Vieira S, Pinaya WHL, Mechelli A. Using deep learning to investigate the neuroimaging correlates of psychiatric and neurological disorders: Methods and applications. Neurosci Biobehav Rev. 2017; 74:58-75.
CrossRef - Sivaranjini S, Sujatha CM. Deep learning-based diagnosis of Parkinson’s disease using convolutional neural network. Multimed Tools Appl. 2020;79(21-22):15467-15479.
CrossRef - Ravi D, Wong C, Deligianni F, et al. Deep learning for health informatics. IEEE J Biomed Health Inform. 2017;21(1):4-21.
CrossRef - Pereira S, Pinto A, Alves V, Silva CA. Brain tumor segmentation using convolutional neural networks in MRI images. IEEE Trans Med Imaging. 2016;35(5):1240-1251.
CrossRef - Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Z Med Phys. 2019;29(2):102-127.
CrossRef - Arbabshirani MR, Plis S, Sui J, et al. Single subject prediction of brain disorders in neuroimaging: Promises and pitfalls. Neuroimage. 2017; 145:137-165.
CrossRef - Pereira T, Tran N, Gadhoumi K, et al. Photoplethysmography based atrial fibrillation detection: a review. NPJ Digit Med. 2020;3(1):3.
CrossRef - Kubben PL, Dumontier M, Dekker A. Fundamentals of Clinical Data Science. Springer; 2019.
CrossRef - Rundo L, Militello C, Vitabile S, et al. Combining convolutional neural networks and handcrafted features for prostate cancer detection in multi-parametric MRI. Comput Med Imaging Graph. 2019; 77:101647.
- Wang J, Yang X, Cai H, Tan W, Jin C, Li L. Discrimination of breast cancer with microcalcifications on mammography by deep learning. Sci Rep. 2016; 6:27327.
CrossRef - Esteva A, Kuprel B, Novoa RA, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542(7639):115-118.
CrossRef - Shen D, Wu G, Suk HI. Deep learning in medical image analysis. Annu Rev Biomed Eng. 2017; 19:221-248.
CrossRef - LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015;521(7553):436-444.
CrossRef - Litjens G, Kooi T, Bejnordi BE, et al. A survey on deep learning in medical image analysis. Med Image Anal. 2017; 42:60-88.
CrossRef - Zhou SK, Greenspan H, Shen D. Deep learning for medical image analysis: challenges and future directions. In: Deep Learning for Medical Image Analysis. Academic Press; 2017:1-16.
- Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med. 2019;25(1):24-29.
CrossRef - Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44-56.
CrossRef - Lee CS, Nagy PG, Weaver SJ, Newman-Toker DE. Cognitive and system factors contributing to diagnostic errors in radiology. AJR Am J Roentgenol. 2013;201(3):611-617.
CrossRef - Pesapane F, Codari M, Sardanelli F. Artificial intelligence in medical imaging: threat or opportunity? Radiologists again at the forefront of innovation in medicine. Eur Radiol Exp. 2018;2(1):35.
CrossRef - Erickson BJ, Korfiatis P, Akkus Z, Kline TL. Machine learning for medical imaging. Radiographics. 2017;37(2):505-515.
CrossRef - Oakden-Rayner L. Exploring large-scale public medical image datasets. Acad Radiol. 2020;27(1):106-112.
CrossRef - Kelly CJ, Karthikesalingam A, Suleyman M, Corrado G, King D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019;17(1):195.
CrossRef - Beam AL, Kohane IS. Big data and machine learning in health care. JAMA.2018;319(13):1317-1318.
CrossRef - Rajpurkar P, Irvin J, Zhu K, et al. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv. 2017.
- Badura P, Brůha P, Dušek L, et al. Big data in healthcare: management, analysis, and future prospects. Int J Data Sci Anal. 2021;11(2):123-140.
- Zeng X, Luo X, Zhang L, et al. Development of a machine learning model to predict outcome after traumatic brain injury: A multicenter analysis. J Neurotrauma. 2020;37(17):1930-1938.
- Senders JT, Arnaout O, Karhade AV, et al. Natural and artificial intelligence in neurosurgery: a systematic review. Neurosurgery. 2018;83(2):181-192.
CrossRef - Roski J, Bo-Linn GW, Andrews TA. Creating value in health care through big data: opportunities and policy implications. Health Aff (Millwood). 2014;33(7):1115-1122.
CrossRef - Vellido A. Societal issues concerning the application of artificial intelligence in medicine. Kidney Dis (Basel). 2019;5(1):11-17.
CrossRef

