
Manuscript accepted on :03-12-2025
Published online on: 23-12-2025
Plagiarism Check: Yes
Reviewed by: Dr. Emmanuel Dike and Dr. Pratheepa Sivashankari N
Second Review by: Dr. Rahul Sable
Final Approval by: Dr. Anton R Keslav
Anisyah Achmad1* , Umar Idris Ibrahim2Thomas Erwin Christian, Junus Huwae3, Herman Tolle4 Arsy Arundina1Ardaleni Frista1and Nuraida Fara Rahmani1
, Umar Idris Ibrahim2Thomas Erwin Christian, Junus Huwae3, Herman Tolle4 Arsy Arundina1Ardaleni Frista1and Nuraida Fara Rahmani1
1Department of Pharmacy, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia.
2 Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, Universiti Sultan Zainal Abidin, Besut Campus, Terengganu, Malaysia.
3Department of Orthopaedics and Traumatology, Faculty of Medicine, Universitas Brawijaya and Saiful Anwar Hospital, Malang, Indonesia.
4Department of Informatics Engineering, Faculty of Computer Science, Universitas Brawijaya, Malang, Indonesia.
Corresponding Author E-mail: 3littleangels@ub.ac.id
DOI : https://dx.doi.org/10.13005/bpj/3314
Abstract
Osteoarthritis (OA) is a chronic degenerative condition affecting the joints. SEPO is a digital application designed for therapeutic management with the goal of enhancing the QoL OA patients. This study aimed to establish reliable and valid measurement tools for assessing the content and application. The validation and realization test SEPO content using google forms was carried out at primary health facilities in Malang, Indonesia with total 30 OA patients. Assessment of validity and reliability of SEPO content using Pearson Product Moment (r > 0.3) and Crobach’s Alpha (r > 0.6). Meanwhile, the validation SEPO application using FGD by eight raters by zoom meeting with a CVR value of > 0.71. The results of the SEPO content validity test were r count > 0.3 and reliability results were obtained for VAS r = 0,8 , for WOMAC r = 0.755 , for sodium diet compliance questionnaire r = 0.840 so that questionnaire was also valid and reliable, while for SEPO application validity test the results of CVR value = 0.99 so that the SEPO digital app is worth to use. The SEPO digital application can be used as a measurement tool to improve the QoL of OA patients.
Keywords
Content validity; Digital Health; Indonesia; Osteoarthritis; Self-management
Download this article as:| Copy the following to cite this article: Achmad A, Ibrahim U. I, Huwae T. E. C. J, Tolle H, Arundina A, Frista A, Rahmani N. F, Creation and Validation of the SEPO Digital Application for Osteoarthritis Self-Management in Indonesia. Biomed Pharmacol J 2025;18(4). |
| Copy the following to cite this URL: Achmad A, Ibrahim U. I, Huwae T. E. C. J, Tolle H, Arundina A, Frista A, Rahmani N. F, Creation and Validation of the SEPO Digital Application for Osteoarthritis Self-Management in Indonesia. Biomed Pharmacol J 2025;18(4). Available from: https://bit.ly/3MIxC6N |
Introduction
Osteoarthritis (OA) is the most prevalent form of degenerative joint disease and a leading cause of disability in aging populations.1 OA primarily affects load-bearing joints, especially the knees, hips, and spine, but can also involve the hands and other joints.2, 3 Its impact is particularly profound among older adults, though younger individuals with risk factors such as joint injuries, obesity, and metabolic disorders are also susceptible.4,5 The progressive nature of OA makes early intervention and long-term management essential to preserving joint function and maintaining patient independence.6,7
In Indonesia, OA poses a growing public health concern. National epidemiological data indicate a prevalence rate of 5% in men and 12.7% in women, as determined by radiological examinations of the knee.3, 8 This gender disparity reflects hormonal, anatomical, and lifestyle differences that contribute to disease onset and progression.9, 10 The prevalence of OA increases significantly after the age of 45 and affects nearly 40% of individuals over 70 years, as reported by global data from the Centers for Disease Control and Prevention.11, 12 This trend mirrors a broader demographic shift toward aging populations, where the burden of non-communicable, chronic conditions such as OA continues to rise.13, 14 With its progressive nature and lack of curative treatments, OA represents a substantial challenge to both individual well-being and national healthcare systems.
Clinical management of OA relies on a combination of pharmacologic and non-pharmacologic strategies.15-17 Pharmacological interventions, including nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, and analgesics, primarily target symptom relief but do not halt disease progression.18, 19 Moreover, long-term use of such medications is associated with adverse effects, particularly in elderly patients with comorbidities.20 Consequently, non-pharmacologic approaches are emphasized in clinical guidelines as first-line interventions due to their potential for sustainable benefit and minimal risk. These approaches include weight management, structured physical activity, lifestyle modification, and patient education. Among these, education and self-management have garnered increasing attention as they empower patients to take active roles in their care, improve treatment adherence, and support behavior change.21-23
Self-management is essential in osteoarthritis (OA) care, included diet pattern. A high-sodium diet is also a risk factor for OA and increased pain. This mechanism is associated with increased secretion of IL-17A, TNF-alpha, and IL-6, as well as the opening of sodium channels. In Indonesia, where high-sodium diets are common, reducing sodium intake is crucial in OA management.7, 10 The manual Self-Education Program for Osteoarthritis (SEPO) previously showed success in improving dietary habits and reducing pain but lacked scalability. With rising smartphone use, digital health tools offer a more accessible alternative. A digital version of SEPO now delivers interactive, multimedia content and supports patient engagement through self-assessment and personalized feedback, making it a promising tool for effective and scalable OA self-management.4, 10
The SEPO program has since been adapted into a digital application designed to enhance OA self-management in a scalable and user-friendly manner. This application includes modules on OA pathophysiology, symptom control strategies, sodium reduction practices, and exercise guidance.16, 23 It incorporates visual and audio elements to cater to varying levels of literacy and learning styles. Embedded within the application are three validated assessment tools: the Visual Analog Scale (VAS) for pain intensity, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) for functional limitation, and a sodium diet compliance questionnaire tailored for the Indonesian context. These tools are supported by visual cues to enhance user understanding and accuracy.15, 19, 24
To ensure the effectiveness of this digital intervention, a mixed-method validation approach is employed. Quantitative analysis evaluates the psychometric properties of the assessment tools using Pearson’s correlation and Cronbach’s Alpha, while qualitative feedback from expert panels informs the application’s content relevance and usability through the Content Validity Ratio (CVR). Together, these efforts aim to establish SEPO as a reliable, culturally relevant digital resource for OA self-management in Indonesia.
This work directly aligns with Sustainable Development Goal (SDG) 3, which emphasizes ensuring healthy lives and promoting well-being for all at all ages. By enhancing patient education, improving musculoskeletal self-management, and increasing access to digital health tools, the SEPO application contributes particularly to SDG 3.4 in reducing the burden of non-communicable diseases through prevention and long-term disease management.
Materials and Methods
Researchers determined 30 participants for digital SEPO validation who diagnosed with osteoarthritis (OA), aged between 26 and 62 years, who voluntarily provided written informed consent. To ensure a homogenous sample and minimize confounding variables, inclusion criteria specified that all subjects must be non-smokers (defined as consuming fewer than one pack of cigarettes per day), have abstained from alcohol intake for at least one month prior to enrolment, and exhibit no history of comorbid inflammatory or autoimmune joint disorders, including rheumatoid arthritis, spondylitis, psoriasis, or gout. Furthermore, individuals with a prior history of joint surgery or intra-articular injections were excluded to prevent interference with baseline functional or pain assessments.
Individuals who were taking medications known to affect pain perception, joint function, or inflammatory response such as systemic corticosteroids, opioid analgesics, disease-modifying antirheumatic drugs (DMARDs), recent intra-articular steroid injections (within 3 months), or regular NSAID use were excluded to prevent drug-related bias in pain and functional assessment.
Ethical clearance was sought from the Health Research Ethics Commission of the Faculty of Medicine, University of Brawijaya, (No. 280 / EC / KEPK / 09 / 2023). Additionally, informed consent was obtained from all participants prior to data collection after all necessary information about the study was provided.
Content of Validation and Reliability
The SEPO digital application includes three primary assessment instruments, each of which was subjected to validity and reliability testing: the Visual Analog Scale (VAS) for pain intensity, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) for functional activity, and a sodium diet compliance questionnaire. These tools were chosen for their relevance to osteoarthritis self-management and were adapted into user-friendly digital formats to enhance accessibility and comprehension.
The VAS is presented as a numeric scale ranging from 0 to 10, accompanied by emotive facial illustrations to help participants accurately rate their pain levels. The WOMAC index evaluates functional impairment across three domains, pain, stiffness, and physical function, with each item supported by clear, context-specific images to facilitate understanding. The sodium diet compliance questionnaire consists of ten dichotomous (yes/no) items, each supplemented with visual cues to clarify the intent of the questions and support accurate responses. All three instruments were administered via Google Forms, with image-based enhancements integrated throughout to accommodate varying levels of health literacy and improve participant comprehension.
Participants accessed the SEPO digital application once during the validation session. Each subject completed the VAS, WOMAC, and sodium diet compliance questionnaires in a single sitting, which took approximately 15–20 minutes. No repeated measures were conducted, as the objective of this phase was to evaluate content validity, usability, and initial reliability in one-time use
To evaluate the psychometric properties of these tools, two statistical methods were employed. The Pearson Product Moment correlation coefficient (r) was used to assess the validity of each questionnaire, determining the extent to which the items accurately measured the intended constructs. A correlation coefficient of r > 0.36 was established as the threshold for acceptable validity, acceptable relationship to external criteria. In parallel, the Cronbach’s Alpha coefficient was applied to examine internal consistency, ensuring that the instruments reliably measured participants’ perceptions and attitudes. A reliability coefficient of r > 0.60 was considered indicative of acceptable internal consistency
This dual analysis ensured that each instrument within the SEPO application demonstrated both construct validity and internal reliability, supporting its use as a standardized and effective tool for assessing key aspects of osteoarthritis management in a digital format.
Validation of digital SEPO application
In addition to content validation and reliability testing, the SEPO digital application underwent a qualitative evaluation through a structured Focus Group Discussion (FGD)25. The SEPO application was further evaluated through an expert Focus Group Discussion (FGD), as described in the following section.
 |
Figure 1: Methodology and validation flowchart of the SEPO digital application. The diagram outlines the sequential phases of the study, beginning with participant selection based on strict inclusion and exclusion criteria, followed by the deployment of digital assessment tools,Click here to view Figure |
Figure 1. Methodology and validation flowchart of the SEPO digital application. The diagram outlines the sequential phases of the study, beginning with participant selection based on strict inclusion and exclusion criteria, followed by the deployment of digital assessment tools, statistical validation using Pearson’s r and Cronbach’s alpha, expert evaluation through a Focus Group Discussion (FGD) using Content Validity Ratio (CVR), and culminating in the development of a validated digital application for osteoarthritis (OA) self-management.
Results
Participant demographics
A total of 30 participants diagnosed with osteoarthritis (OA) were enrolled in the study. The demographic distribution included 22 females (73.3%) and 8 males (26.7%), reflecting the higher prevalence of OA among women, as commonly reported in epidemiological studies. The age ranged from 26 to 62 years, with a mean age indicative of middle-to-late adulthood, a demographic in which OA is frequently observed. All participants met the study’s inclusion criteria, which excluded individuals with comorbid inflammatory joint diseases or recent surgical interventions, ensuring a focused and homogenous sample. Participants demonstrated sufficient digital literacy to interact with the SEPO application independently, supporting the feasibility of digital intervention in this age group. As Figure 2 shows, most participants were female, and the age distribution was balanced across the defined age ranges, with the highest concentration observed in the 46–55-year group, aligning with the known epidemiological peak of OA onset.
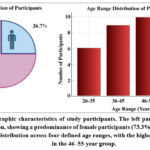 |
Figure 2: Demographic characteristics of study participants. The left panel illustrates the gender distribution, showing a predominance of female participants (73.3%). Click here to view Figure |
Validity testing of the SEPO assessment tools
The SEPO application incorporates three self-assessment tools: the Visual Analog Scale (VAS) for pain, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) for functional activity, and a sodium diet compliance questionnaire designed to assess dietary behavior. These instruments were administered in a digital format using Google Forms, with each question supplemented by illustrative images to improve clarity and facilitate understanding particularly for participants with lower health literacy levels.
To evaluate construct validity, the Pearson Product Moment correlation coefficient (r) was applied to each instrument. The analysis demonstrated that all three tools achieved r count values exceeding 0.3, which is generally accepted as the minimum threshold for construct validity. Specifically, the VAS, WOMAC, and sodium diet compliance questionnaire each showed significant correlations with their respective constructs, affirming their effectiveness in measuring pain severity, functional limitations, and dietary compliance.
These findings indicate that the SEPO assessment tools are well-aligned with the conceptual framework of osteoarthritis self-management. The integration of visual elements appears to enhance user comprehension, contributing to the strength of the observed correlations. As illustrated in Figure 3, all instruments performed above the validity threshold, thereby confirming their appropriateness for use in a digitally delivered self-education and monitoring platform.
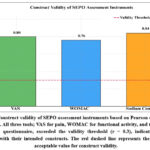 |
Figure 3: Construct validity of SEPO assessment instruments based on Pearson correlation coefficients. All three tools; VAS for pain, WOMAC for functional activity, and the sodium compliance questionnaire, Click here to view Figure |
Reliability testing of the SEPO assessment tools
Internal consistency of the SEPO questionnaires was evaluated using Cronbach’s Alpha to determine their reliability. The Visual Analog Scale (VAS) achieved a coefficient of r = 0.800, indicating strong internal consistency for measuring perceived pain. The WOMAC index yielded a value of r = 0.755, reflecting good reliability across its domains of pain, stiffness, and physical function. The sodium diet compliance questionnaire produced the highest reliability score, r = 0.840, signifying excellent consistency in capturing dietary behaviours related to sodium intake. These values surpass the generally accepted reliability threshold of r > 0.6, confirming that all three instruments demonstrate robust internal consistency. The integration of visual aids within digital questionnaires likely contributed to this consistency by improving user comprehension and reducing the likelihood of misinterpretation. This enhancement is particularly beneficial in diverse populations with varying levels of health literacy, supporting the utility of visual augmentation in digital health tools. As illustrated in Figure 4, all SEPO assessment tools demonstrated reliability coefficients well above the established threshold, reinforcing their dependability for accurately capturing patient-reported outcomes in a digital format.
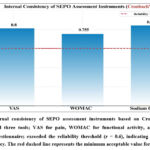 |
Figure 4: Internal consistency of SEPO assessment instruments based on Cronbach’s Alpha coefficients. All three tools; VAS for pain, WOMAC for functional activity, and the sodium compliance questionnaire; exceeded the reliability threshold (r = 0.6),Click here to view Figure |
Expert validation of the SEPO application via focus group discussion
To complement the quantitative analysis, a Focus Group Discussion (FGD) was conducted with eight expert raters, including physicians, pharmacists, nutritionists, and digital health developers. The FGD was held virtually via Zoom and spanned approximately 120 minutes. During the session, the facilitator introduced the SEPO application, outlined the objectives of the discussion, and guided a structured evaluation of the app’s content, design, usability, and educational efficacy. Participants were encouraged to provide open and candid feedback on all elements of the application.
The qualitative input gathered during the FGD was subsequently quantified using the Content Validity Ratio (CVR) method. Experts rated each item on a standardized three-point scale: “Essential,” “Useful but not essential,” and “Not necessary.” These ratings were then used to calculate the CVR for individual components, resulting in an overall CVR of 0.99, significantly surpassing the minimum acceptance threshold of 0.71. This high score indicates near-unanimous expert agreement regarding the relevance and appropriateness of the application’s content.
In addition to validating content quality, experts highlighted several practical strengths of the SEPO digital platform. The transition from manual to digital delivery was viewed as a major advancement, allowing for greater scalability and ease of dissemination. Participants praised the inclusion of multimedia elements such as text, images, and videos which supported varied learning preferences and improved user engagement. Features such as ease of navigation, cultural relevance, and integration of assessment tools were also recognized as enhancing the app’s overall usability and impact.
As illustrated in Figure 5, expert agreement across the evaluated domains ranged from 92% to 100%, with particularly high ratings for content relevance, educational value, and scalability. This strong consensus underscores the application’s potential to serve as an effective, user-centered, and culturally adapted tool for supporting OA self-management on a large scale.
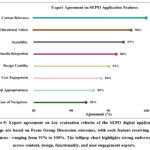 |
Figure 5: Expert agreement on key evaluation criteria of the SEPO digital application. Ratings are based on Focus Group Discussion outcomes, with each feature receiving high consensus—ranging from 92% to 100%. Click here to view Figure |
Discussion
Osteoarthritis (OA) is a prevalent degenerative joint disease marked by the progressive deterioration of articular cartilage, leading to chronic pain, stiffness, and functional limitation. It commonly affects weight-bearing joints such as the knees, hips, and spine, although the hands and other joints may also be involved. Risk factors include aging, genetic predisposition, joint injuries, obesity, and repetitive mechanical stress.26, 27 As the disease advances, the breakdown of cartilage results in bone-on-bone contact, inflammation, and reduced joint mobility, which can severely compromise an individual’s quality of life.3
In the absence of curative treatment, current OA management emphasizes symptom control and functional improvement. Non-pharmacological interventions are recommended as first-line therapy, including lifestyle modification, physical exercise, and patient education.6 A critical element in this approach is self-management, which empowers patients to actively participate in managing their condition. Self-management strategies have been shown to improve health outcomes by promoting behavioral change, enhancing adherence, and reducing dependency on clinical services.22
The Self-Education Program for Osteoarthritis (SEPO) was initially developed as a manual intervention, delivered through face-to-face counselling, WhatsApp communication, and educational videos. This model showed promising outcomes, particularly in reducing sodium intake and improving OA symptomatology.4 However, manual implementation presented several limitations, including scalability issues, inconsistent access to materials, and dependency on direct provider interaction.
To address these challenges and align with evolving digital health trends, the SEPO intervention was transformed into a digital application. The app offers an integrated educational experience through multimedia content, including videos, infographics, and dietary posters, which cover OA pathophysiology, clinical symptoms, risk factors, and preventive strategies. One key innovation is the inclusion of structured audiovisual modules on low-impact exercises tailored for knee OA patients, as well as detailed dietary guidance for reducing sodium intake an identified modifiable risk factor for OA-related inflammation.
Moreover, the SEPO digital platform enables structured self-assessment using validated tools: the Visual Analog Scale (VAS) for pain intensity, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) for functional capacity, and a sodium diet compliance questionnaire. These instruments were integrated with visual enhancements to aid comprehension, especially among users with varying levels of health literacy. The use of pre- and post-intervention comparisons allows for the evaluation of behavioural and clinical changes over time, supporting personalized monitoring and feedback.
The transition to digital format has the potential to significantly expand the reach and impact of SEPO by overcoming barriers of time, geography, and provider availability. The platform aligns with WHO recommendations promoting the use of mobile health (mHealth) tools to enhance chronic disease management, particularly in resource-constrained settings. By providing accessible, user-cantered, and evidence-based education, the SEPO application addresses the core needs of OA patients and holds promise for large-scale deployment in public health initiatives focused on musculoskeletal disorders.
VAS
The Visual Analogue Scale (VAS) is a widely utilized instrument for assessing pain intensity and has consistently demonstrated strong validity and reliability in both clinical and research settings. It is particularly effective for capturing subjective pain experiences in a simple and scalable format.13 In the context of the SEPO digital application, the VAS is presented using pictorial emoticons aligned along a numeric scale ranging from 0 to 10, allowing patients to visually indicate their perceived pain levels. The interpretation of VAS scores is standardized as follows: 0 indicates no pain, 1–3 represents mild pain, 4–6 corresponds to moderate pain, 7–9 reflects very severe pain, and 10 denotes the worst pain possible as mentioned in figure 5.28
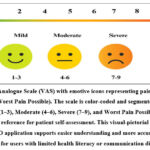 |
Figure 6: Visual Analogue Scale (VAS) with emotive icons representing pain intensity from 0 (No Pain) to 10 (Worst Pain Possible). The scale is color-coded and segmented into five levels: Click here to view Figure |
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is a widely recognized and validated instrument used to evaluate functional impairment in individuals with osteoarthritis. It measures three primary domains: pain, stiffness, and physical function, offering a comprehensive profile of the patient’s ability to perform daily tasks and the severity of their symptoms3
In the context of the SEPO digital application, the WOMAC questionnaire is adapted into a user-friendly digital format. To enhance comprehension and minimize confusion, especially among users with limited literacy or digital experience, each question is accompanied by a clear, context-specific illustration. This visual support allows participants to better interpret the question and relate it to their daily experiences, thereby improving response accuracy. The pain domain assesses how much pain is experienced during various activities as mentioned in Table 1.
Table 1: Domains and itemized questions of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) used in the SEPO digital application. The table outlines the assessment of pain, stiffness, and physical function to evaluate the impact of osteoarthritis on daily living activities.
| Domain | Question |
| Pain | How painful is it when walking? |
| How painful is it when climbing stairs? | |
| How painful is it at night before going to bed? | |
| How painful is rest such as sitting or lying down? | |
| How painful is it when carrying goods or loads? | |
| stiffness | How heavy is stiffness felt after walking in the morning? |
| How severe is the stiffness felt after sitting, waking up and after resting in daily life? | |
| Physical Functions | How difficult is it when climbing stairs? |
| How difficult is it when going downstairs? | |
| How difficult is it when standing up from sitting? | |
| How difficult is it when standing upright? | |
| How hard is it when bending over to touch the floor? | |
| How difficult is it when traveling on a flat surface? | |
| How difficult is it to get on or off a vehicle (motorcycle, car, public transport)? | |
| How hard is it when going shopping? | |
| How hard is it when wearing socks? | |
| How hard is it when lying in bed? | |
| How hard is it when taking off socks? | |
| How hard is it when getting out of bed? | |
| How difficult is it when entering or exiting the bathroom? | |
| How difficult is it when sitting? | |
| How hard is it to go to the toilet to defecate? | |
| How difficult is it when performing light household tasks (such as washing dishes, ironing, cooking, sweeping and mopping)? | |
| How difficult is it when doing heavy household tasks (such as moving heavy furniture, babysitting, carrying children, and active play with children)? |
Each item is scored on a 5-point Likert scale, ranging from 0 (none) to 4 (very severe). The total score is obtained by summing all individual item scores. The interpretation of the total WOMAC score is categorized as follows: scores between 0–24 reflect mild impairment, 25–48 moderate impairment, 49–72 severe impairment, and 73–96 very severe impairment.
This digital and visually supported version of WOMAC within SEPO enhances patient engagement, improves response accuracy, and ensures consistent evaluation of functional outcomes in OA self-management interventions.
Sodium diet compliance questionnaire
The sodium diet questionnaire was developed to assess the dietary behavior of osteoarthritis (OA) patients regarding sodium intake. It consists of ten questions designed to evaluate daily habits related to sodium consumption. Each question has two possible responses: Yes or No. For scoring purposes, each correct (healthy) behavior is awarded 1 point, while an incorrect response receives 0 points (see Table 2).
Table 2: Sodium Diet Compliance Questionnaire Items
| Question | Answer |
| Do you put table salt on the dining table? | Yes or No |
| Do you put packaged condiments (tomato sauce, soy sauce, sesame oil, flavouring, etc.) on the dining table? | Yes or No |
| Do you usually use fresh herbs to add Savory flavour to dishes? | Yes or No |
| Do you cook without using salt and only add to each person’s plate as needed? | Yes or No |
| Do you use ready-to-eat seasonings when cooking? | Yes or No |
| Do you avoid foods made by adding excess salt (pickles, salted fish, trasi)? | Yes or No |
| Do you usually read nutrition labels before consuming processed products and reduce foods labelled with “sodium” content? | Yes or No |
| Do you consume salt according to the recommendation which is a maximum of 1.5 teaspoons or about 1.500mg per day? | Yes or No |
| Do you usually cook your own food at home without buying ready-to-eat food from outside? | Yes or No |
| Do you usually use fresh ingredients instead of frozen or packaged food? | Yes or No |
To enhance comprehension and reduce misinterpretation, each question is accompanied by an illustrative image in the SEPO digital application. This visual support helps standardize the perception of each question across diverse users, particularly those with limited health literacy or varying cultural interpretations.
The questionnaire score is calculated based on the total number of correct answers. A higher score indicates greater adherence to recommended sodium intake practices, suggesting better dietary behaviour and reduced sodium consumption. Conversely, a lower score implies poor compliance and higher sodium intake risk, which may exacerbate OA symptoms due to inflammation and comorbid conditions such as hypertension.
Incorporating this questionnaire into the SEPO digital platform represents a significant advancement from the manual SEPO intervention. The digital version allows for easier access, personalized feedback, and visual engagement. This integration also benefits medical professionals, particularly pharmacists, by supporting pharmaceutical care services that extend beyond medication management to encompass lifestyle and dietary counselling. By enabling continuous self-monitoring of dietary habits, medication compliance, and OA symptoms, the SEPO application supports early intervention and empowers patients to adopt long-term self-management strategies. This, in turn, contributes to improved health outcomes and enhanced quality of life for individuals living with osteoarthritis. These findings support global health priorities under Sustainable Development Goal (SDG) 3 by improving access to digital self-management tools for chronic musculoskeletal conditions
It is important to clarify that this study focused solely on validating the SEPO digital application and its embedded assessment tools. The study did not assess clinical outcomes such as changes in pain severity, functional improvement, or sodium intake reduction. Although previous manual SEPO interventions demonstrated clinical benefits, the present validation study is limited to establishing the validity, reliability, and usability of SEPO as a digital educational and self-management tool. Future interventional studies are required to evaluate SEPO’s clinical effectiveness.
Conclusion
The SEPO digital application is a validated, reliable tool for osteoarthritis management, integrating accurate assessments of pain, physical function, and dietary behaviour through the Visual Analogue Scale, WOMAC index, and sodium diet compliance questionnaire. By combining evidence-based educational content with interactive self-assessment, SEPO empowers patients to actively manage their condition, improve symptoms, and adopt healthier behaviours. Its accessible, scalable design overcomes common barriers to care, making it particularly valuable in resource-limited settings. SEPO offers a practical, patient-cantered model for integrating digital health into musculoskeletal care, supporting healthcare professionals and improving quality of life for individuals with osteoarthritis.
Acknowledgement
We would like to express my deep gratitude to all the participants for their assistance in completing this research project successfully.
Funding Source
The author(s) received no financial support for the research, authorship, and/or publication of this article
Conflict of interest
The author(s) do not have any conflict of interest
Data Availability Statement
This statement does not apply to this article
Ethics Statement
Ethical clearance was sought from the Health Research Ethics Commission of the Faculty of Medicine, University of Brawijaya, (No. 280 / EC / KEPK / 09 / 2023). Additionally, informed consent was obtained from all participants prior to data collection after all necessary information about the study was provided.
Informed Consent Statement
Written informed consent was obtained from all participants at the beginning of the study.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not applicable.
Author Contributions
- Anisyah Achmad: Data collection, Analysis, Conceptualization, Methodology, Writing – Original Draft.
- Umar Idris Ibrahim: Analysis, Visualization, Review & Editing
- Thomas Erwin C. J. Huwae: Data collection, Review & Editing
- Herman Tolle: Data collection, Review & Editing
- Arsy Arundina: Data collection, Review & Editing
- Ardaleni Frista: Data collection, Review & Editing
- Nuraida Fara Rahmani: Data collection, Review & Editing
References
- Akhmetshin E. M, Ibatullin R. R, Gapsalamov A. R, Vasilev V. L, Bakhvalov S. Y. Audiovisual aids application in the secondary-level vocational education establishments: Efficiency analysis and assessment. J. Educ. Manag. 2019; 33:374-92.
CrossRef - Ou J, Zhang J, Alswadeh M, et al. Advancing osteoarthritis research: the role of AI in clinical, imaging and omics fields. Bone Res. 2025; 13:48.
CrossRef - Sananta P, Ariyanti N. T, Widasmara D, Fuzianingsih E. N. Is there any correlation between physical activity and severity of knee osteoarthritis in secondary referral hospitals in Indonesia? 2022; 42:1014-7.
CrossRef - Achmad A, Suharjono S, Soeroso J, etal. Self-education Program for Osteoarthritis Reduces Sodium Intake, Knee Joint pain, and Serum Interleukin-17A level in Osteoarthritis Patients. OAMJMS. 2022; 10:2633-8.
CrossRef - Jin X, Ackerman I. N, Ademi Z. Loss of productivity‐adjusted life‐years in working‐age Australians due to knee osteoarthritis: a life‐table modeling approach. AC&R. 2023; 75:482-90.
CrossRef - Allen K. D, Thoma L. M, Golightly Y. M. Epidemiology of osteoarthritis. OA&C. 2022; 30:184-95.
CrossRef - Hiruthyaswamy S. P, Bose A, Upadhyay A, et al. Molecular signaling pathways in osteoarthritis and biomaterials for cartilage regeneration: a review. Bioengineered. 2025; 16:2501880.
CrossRef - Mekariya K, Vanitcharoenkul E, Chotiyarnwong P, Adulkasem N, Unnanuntana A. High prevalence of symptomatic knee osteoarthritis among patients who have fragility hip fractures. Pain Res Manag. 2025;
CrossRef - Guan M, Zhang X, Li X, et al. Research Progress of Osteoarthritis Treatment by Low Intensity Pulsed Ultrasound. Smart Med. 2025;4: e70003.
CrossRef - Sulistyaning A. R, Farida F. Overview of high sodium eating habits before and after covid-19 pandemic in indonesia. Gizi Indonesia. 2021; 44:133-44.
CrossRef - Fuggle N, Laslop A, Rizzoli R, et al. Treatment of osteoporosis and osteoarthritis in the oldest old. Drugs. 2025; 85, 343–360.
CrossRef - Goyal M, Santhanam S. Epidemiology of rheumatic diseases in tropical populations. Best Pract Res Clin Rheumatol. 2025; 39:102059.
CrossRef - Begum M. R, Hossain M. A. Validity and reliability of visual analogue scale (VAS) for pain measurement. Med. Case Rep. 2019;2 (11).
- Silver S. R, Li J, Saydah S. H. Burden of Selected Chronic Conditions Among Adults of Prime Working Age (25–54) by 2022 Self‐Reported COVID‐19 and Long COVID History Compared to 2019 Pre‐Pandemic Baseline Prevalence: Behavioral Risk Factor Surveillance System. Am J Ind Med. 2025; 68: 620–630.
CrossRef - Bashiri H, Mohammadi F, Soltani H, et al. Comparative Efficacy of Topical Meloxicam and Diclofenac in Primary Knee Osteoarthritis: a Randomized Double-Blind Controlled Trial. Compr Clin Med. 2025; 7:134.
CrossRef - Devigili G, Di Stefano G, Donadio V, et al. Therapeutic approach to fibromyalgia: a consensus statement on pharmacological and non-pharmacological treatment from the neuropathic pain special interest group of the Italian neurological society. Sci. 2025; 46:2263-88.
CrossRef - Eckstein F, Mobasheri A, Boesen M. P. Multifaceted imaging strategies for clinical trials of knee osteoarthritis—a tightly interlinked value and precision chain. Skeletal Radiol2025:1-4.
CrossRef - Allgood J. E, Whitney L, Goodwin J, Chong B. S, Brooks A, Pullan J. The role of pain medications in modulating peripheral nerve injury recovery. Clin. Pharmacol. 2025; 65:411-23.
CrossRef - Ryan M, Megyeri S, Nuffer W, Trujillo J. M. The potential role of GLP‐1 receptor agonists in osteoarthritis. Pharmacotherapy. 2025; 45:177-86.
CrossRef - Fedorchenko Y, Fedorchenko M, Yessirkepov M, Bekaryssova D. Sauna therapy in rheumatic diseases: mechanisms, potential benefits, and cautions. Int. 2025; 45:94.
CrossRef - Mora J. C, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: pathophysiology and current treatment modalities. Pain Res. 2018:2189-96.
CrossRef - Todorovic S. T, Cicovacki S, Popovic D, Hanna F. The Need for a Multidisciplinary Approach in Patients with Hip and Knee Osteoarthritis. 2023; 13:1-4.
- Zhang Q, Li J, Yao Y, et al. The development of a clinical nomogram to predict medication nonadherence in patients with knee osteoarthritis. Medicine. 2023;102(31): e34481.
CrossRef - Östlind E, Eek F, Stigmar K, Ekvall Hansson E. Effects of self-monitoring physical activity with wearable activity trackers on perceived joint function and health-related quality of life in people with hip and knee osteoarthritis: a secondary analysis of a cluster-randomised clinical trial. BMC Musculoskelet. Disord. 2025; 26:33.
CrossRef - Nyumba T, Wilson K, Derrick C, Mukherjee N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018;9(1):20-32.
CrossRef - Kongdang P, Chokchaitaweesuk C, Tangyuenyong S, Ongchai S. Proinflammatory effects of IL-1β combined with IL-17A promoted cartilage degradation and suppressed genes associated with cartilage matrix synthesis in vitro. Molecules. 2019; 24:3682.
CrossRef - Platini H. Self-management program of client with artritis literature review. Jurnal Kesehatan Bakti Tunas Husada: Jurnal Ilmu-ilmu Keperawatan, Analis Kesehatan dan Farmasi. 2018; 18:7-13.
CrossRef - Bielewicz J, Daniluk B, Kamieniak P. VAS and NRS, same or different? Are visual analog scale values and numerical rating scale equally viable tools for assessing patients after microdiscectomy? Pain Res Manag. 2022; 2022:5337483.
CrossRef

