
Manuscript accepted on :08-12-2025
Published online on: 22-12-2025
Plagiarism Check: Yes
Reviewed by: Dr. Tolmas Hamroyev and Dr. Ahmed Salah
Second Review by: Dr. Shail Modi
Final Approval by: Dr. Prabhishek Singh
Rasha Eldeeb1 , May Khalil1*, Mahir Jallo2, Jan Althea Ellao1and Tayyaba Fatima Kamal1
, May Khalil1*, Mahir Jallo2, Jan Althea Ellao1and Tayyaba Fatima Kamal1
1Biomedical Sciences Department, College of Medicine, Gulf Medical University, Ajman, UAE
2Internal Medicine department, Thumbay Teaching Hospital, Gulf Medical University, Ajman, UAE
Corresponding Author E-mail: dr.maykhalil@gmu.ac.ae
DOI : https://dx.doi.org/10.13005/bpj/3331
Abstract
The relationship between hemoglobin levels, anemia, and blood pressure remains insufficiently defined, particularly in Middle Eastern populations. This retrospective study evaluated 200 hypertensive adults treated at a tertiary hospital in the UAE between 2021 and 2025, using medical record data that included hemoglobin levels, anemia status based on WHO criteria, blood pressure according to ACC/AHA thresholds, and relevant demographic variables. Anemia was present in 44% of participants. Hemoglobin demonstrated modest positive correlations with systolic (r = 0.22, p = 0.0015) and diastolic blood pressure (r = 0.27, p < 0.001); however, this association did not remain significant in adjusted models, where hemoglobin was not an independent predictor of hypertension. Age emerged as the strongest determinant of elevated blood pressure, and hemoglobin levels showed no significant variation across antihypertensive medication classes. Overall, hemoglobin appears to contribute only modestly to blood pressure variation, while age-related factors exert a more dominant influence. These findings highlight the value of targeted anemia screening and age-specific approaches to hypertension management in similar populations.
Keywords
Anemia (AN); Blood Pressure (BP); Cardiovascular Risk (CVR), Hemoglobin (Hb); Hypertension (HTN)
Download this article as:| Copy the following to cite this article: Eldeeb R, Khalil M, Jallo M, Ellao J. A, Kamal T. F. Association Between Hemoglobin Levels, Anemia, and Blood Pressure in Hypertensive Adults: A Retrospective Study. Biomed Pharmacol J 2025;18(4). |
| Copy the following to cite this URL: Eldeeb R, Khalil M, Jallo M, Ellao J. A, Kamal T. F. Association Between Hemoglobin Levels, Anemia, and Blood Pressure in Hypertensive Adults: A Retrospective Study. Biomed Pharmacol J 2025;18(4). Available from: https://bit.ly/4aoUgL6 |
Introduction
Hypertension and anemia are two major global public health challenges, particularly in resource-limited settings, including countries in the Gulf region such as the United Arab Emirates (UAE). Hypertension remains a leading cause of cardiovascular morbidity and mortality worldwide, and it contributes significantly to adverse health outcomes such as myocardial infarction, stroke, and chronic kidney disease. At the same time, anemia, particularly iron deficiency anemia, is highly prevalent across various populations and is increasingly recognized as a risk factor for cardiovascular complications.1,2
Among individuals with hypertension, the presence of anemia may contribute to worse clinical outcomes by altering hemodynamic stability and increasing cardiac workload. Chronic anemia leads to a reduction in systemic vascular resistance and an increase in cardiac output, which can promote the development of left ventricular hypertrophy and progressive cardiac remodeling. Left ventricular hypertrophy itself is a well-established predictor of cardiovascular morbidity and all-cause mortality. 3,4
Recent research has highlighted the complex interaction between hemoglobin concentration, anemia, and the regulation of blood pressure. Some studies have proposed that lower hemoglobin levels may decrease blood viscosity and peripheral resistance, which could potentially result in reduced blood pressure. On the other hand, other studies have reported that elevated hemoglobin concentrations may increase vascular resistance and therefore contribute to elevated blood pressure. However, findings across existing literature remain inconsistent, with some studies reporting a positive association, others suggesting an inverse relationship, and several failing to identify any significant correlation. 5-9 In the context of the UAE, both hypertension and anemia are commonly observed health concerns. According to recent national health data, hypertension affects approximately 30 percent of adults in the UAE, while the prevalence of anemia ranges between 20 percent and 40 percent, depending on demographic variables such as age and gender.10,11 Despite the high prevalence of these conditions, there is a limited body of research investigating the potential connection between hemoglobin levels, anemia status, and blood pressure within the UAE population.
Understanding this relationship could offer critical insights into the underlying pathophysiology of hypertension and may help identify hematological markers that support early detection and risk stratification. Considering the public health burden of both conditions in the region, this study aims to assess the association between hemoglobin levels, anemia, and blood pressure among hypertensive adults in the UAE. The findings may contribute to future clinical guideline development and support targeted screening and prevention strategies for cardiovascular disease in similar populations.
Materials and Methods
This study was conducted to examine the relationship between hemoglobin levels, anemia, and blood pressure among hypertensive adults in the United Arab Emirates. The following methods were employed to ensure a comprehensive and reliable analysis.
Study Design
This study employed a retrospective, quantitative research design to examine the association between hemoglobin levels, anemia, and blood pressure among hypertensive patients in the United Arab Emirates. Data were extracted from the medical records of 200 adult patients aged 18 years and older, of both sexes, who were diagnosed with hypertension and received treatment at Thumbay Teaching Hospital, Gulf Medical University, Ajman. The study was conducted between January 2021 and March 2025 and received ethical approval from the Institutional Review Board of Gulf Medical University (Ref. No. IRB-COM-FAC-94-2025). Given that the investigation was based exclusively on anonymized retrospective medical records, the IRB granted a waiver of informed consent. All patient data were anonymized to uphold confidentiality and privacy requirements.
Inclusion and Exclusion Criteria
Inclusion criteria were adults aged 18 years or older, a documented clinical diagnosis of hypertension, availability of hemoglobin measurements, and complete demographic and clinical data. Exclusion criteria included pregnancy, active bleeding, recent blood transfusion within the past three months, hematologic malignancies, chronic inflammatory diseases, and incomplete blood pressure or hemoglobin records.
Diagnostic Thresholds
Hypertension was defined according to ACC/AHA 2017 guidelines as systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥80 mmHg. Anemia was defined using World Health Organization criteria, with hemoglobin concentrations <13 g/dL in males and <12 g/dL in females.
Data Collection Instrument
Data was collected using a structured data extraction form implemented through a spreadsheet. The form was designed to capture both categorical variables, including serial numbers, use of anti-hypertensive medications, and family history of hypertension, as well as quantitative variables such as age, height, weight, systolic and diastolic blood pressure, red blood cell (RBC) count, hemoglobin concentration, and additional hematological indices. Accuracy and reliability of the collected data were ensured through cross-verification procedures and routine data quality checks performed throughout the data collection process.
Data Analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 30. Descriptive statistics were applied to summarize categorical variables as frequencies and percentages, and numerical variables as means and standard deviations. Inferential statistical methods were employed to evaluate the relationship between dependent and independent variables. Chi-square tests were used for categorical data, and logistic regression was applied to assess associations involving binary outcomes. An independent samples t-test was used to compare hemoglobin levels between hypertensive males and females with anemia. In addition, multivariate regression analysis was performed to adjust for potential confounding variables. Statistical significance was defined as a p-value of less than 0.05 for all tests.
Results
The results of this retrospective study are presented according to the study’s objectives. Findings include descriptive statistics of the study population, the prevalence of hypertension and anemia, correlations between hemoglobin levels and blood pressure, as well as subgroup analyses by gender and antihypertensive medication use.
Descriptive Statistics and Prevalence
A total of 200 adult patients were included in the study. Among them, 52.0% had a clinical diagnosis of hypertension, and 44.0% were classified as anemic based on hemoglobin thresholds or documented anemia diagnoses. Notably, 21.0% of participants were presented with both hypertension and anemia in Table 1.
Table 1: Prevalence of Hypertension, Anemia, and Their Co-occurrence Among Study Participants
| Condition | Frequency (n) | Percentage (%) | 95% CI (%) |
| Hypertension only | 67 | 33.5 | 26.9–40.6 |
| Anemia only | 91 | 45.5 | 38.3–52.8 |
| Both Hypertension and Anemia | 42 | 21.0 | 15.5–27.4 |
Gender-based comparisons revealed that anemia was significantly more common in females than in males (χ² = 18.44, p < 0.0001). Additionally, hemoglobin levels were significantly higher among males compared to females (t = 7.20, p < 0.0000000001) in Figure 1.
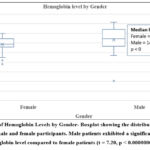 |
Figure 1: Boxplot of Hemoglobin Levels by Gender- Boxplot showing the distribution of hemoglobin concentrations in male and female participants. |
Correlation Between Hemoglobin and Blood Pressure
Pearson correlation analysis revealed a statistically significant but modest positive correlation between hemoglobin levels and systolic blood pressure (r = 0.22, p = 0.0015), as well as diastolic blood pressure (r = 0.27, p = 0.0001) in Table 2.
Table 2: Multivariable Linear Regression Predicting Systolic Blood Pressure
| Variable | Coefficient | Standard Error | p-value | 95% CI (Lower) | 95% CI (Upper) |
| Intercept | 88.73 | 8.43 | <0.001 | 72.10 | 105.36 |
| Hemoglobin (g/dL) | 1.35 | 0.62 | 0.030 | 0.12 | 2.57 |
| Age (years) | 0.39 | 0.08 | <0.001 | 0.23 | 0.54 |
| Gender (Male) | 4.32 | 2.75 | 0.118 | -1.10 | 9.74 |
Hemoglobin as a Predictor of Hypertension
An independent samples t-test was performed to compare hemoglobin levels between hypertensive and non-hypertensive participants. The analysis showed that mean hemoglobin levels were significantly higher among individuals with hypertension (t = 2.13, p = 0.035). This finding is illustrated in Figure 2, which presents the distribution of hemoglobin concentrations stratified by hypertension status.
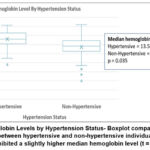 |
Figure 2: Hemoglobin Levels by Hypertension Status- Boxplot comparing hemoglobin concentrations between hypertensive and non-hypertensive individuals. |
To further explore this relationship, a multivariable logistic regression model was conducted using hypertension as the dependent variable, and hemoglobin, age, and gender as predictors. The results showed that hemoglobin (p < 0.001) and age (p < 0.001) were statistically significant predictors of hypertension, while gender was not (p = 0.200). Full model results are presented in Table 3.
Table 3: Logistic Regression Predicting Hypertension
| Variable | OR (95% CI) | p-value |
| Hemoglobin (g/dL) | 2.08 (1.55–2.75) | <0.001 |
| Age (years) | 1.09 (1.06–1.13) | <0.001 |
| Gender (Male) | 0.55 (0.22–1.38) | 0.200 |
Anemia and Hypertension Risk
Anemia could not be included as a predictor in the logistic regression model because the data exhibited quasi-complete separation, preventing stable and interpretable estimation.
Hemoglobin Levels by Antihypertensive Drug Class
A subgroup analysis was conducted among patients who were receiving antihypertensive pharmacologic treatment to evaluate differences in hemoglobin levels by drug class. Medications were categorized into four main groups based on their mechanism of action: angiotensin receptor blockers (ARBs), angiotensin-converting enzyme inhibitors (ACEIs), calcium channel blockers (CCBs), and beta-blockers. Due to small and unequal sample sizes, a non-parametric Kruskal-Walli’s test was applied. The analysis did not show a statistically significant difference in hemoglobin levels between drug classes (H = 4.12, p = 0.249). The distribution of treated patients and corresponding test results is summarized in Table 4.
Table 4: Hemoglobin (g/dL) Levels by Antihypertensive Drug Class
| Drug Class | n (%) | Hemoglobin (g/dL), Median (IQR) |
| ACEI | 9 (26.5%) | 14.00 (13.10–14.30) |
| ARB | 19 (55.9%) | 12.50 (12.20–14.65) |
| Beta-blocker | 3 (8.8%) | 12.00 (11.00–13.55) |
| CCB | 3 (8.8%) | 15.20 (14.15–15.65) |
Discussion
This study explored the relationship between hemoglobin levels, anemia, and hypertension among adult patients in the United Arab Emirates (UAE), with additional subgroup analysis based on gender and antihypertensive medication use. The findings demonstrated a statistically significant but modest positive correlation between hemoglobin concentration and both systolic and diastolic blood pressure. Although hypertensive individuals had significantly higher hemoglobin levels compared to non-hypertensive individuals, hemoglobin was not an independent predictor of hypertension in adjusted regression models. Age emerged as the most consistent and significant factor associated with elevated blood pressure. Furthermore, while females had a significantly higher prevalence of anemia, the analysis did not reveal a significant difference in hemoglobin levels across antihypertensive drug classes.
The observed modest positive correlation between hemoglobin levels and both systolic and diastolic blood pressure supports earlier evidence that hemoglobin concentration may influence vascular resistance and blood viscosity. Higher hemoglobin levels increase blood viscosity, which can elevate systemic vascular resistance and thereby contribute to elevated blood pressure .12 This finding is in agreement with previous research, including a cross-sectional study from Iran, which reported a significant positive correlation between hemoglobin and both systolic and diastolic blood pressure in adults, particularly in men.13 Similarly, a population-based study from Korea found that elevated hemoglobin levels were associated with a higher risk of hypertension, especially among individuals with metabolic syndrome.14 However, the strength of the correlation in the present study was modest, suggesting that hemoglobin may play a contributory, but not dominant, role in blood pressure regulation. This interpretation is consistent with evidence that the relationship may be secondary to shared underlying factors such as age, renal function, or cardiovascular risk profiles. 15
Although hypertensive patients in this study exhibited significantly higher hemoglobin concentrations compared to non-hypertensive individuals, this association did not remain statistically significant after adjusting for age and gender in the multivariable logistic regression model. This finding suggests that the initially observed relationship between hemoglobin and hypertension may have been confounded by age, which emerged as the most consistent and independent predictor of elevated blood pressure in this cohort. Similar findings have been reported in previous studies, where the association between hemoglobin levels and blood pressure was attenuated or eliminated after accounting for age and other clinical variables .16,17
Aging is associated with a series of complex physiological changes that contribute directly to the development of hypertension. Structurally, the arterial wall undergoes remodeling, characterized by increased collagen deposition, fragmentation, and loss of elastin fibers, and thickening of the intima-media layer. These changes reduce arterial compliance and increase pulse wave velocity, leading to isolated systolic hypertension in older adults. 18, 19 Functionally, age-related decline in endothelial function is a key contributor to impaired vascular homeostasis. This is primarily driven by a reduction in nitric oxide (NO) bioavailability, which results from increased oxidative stress, reduced endothelial nitric oxide synthase (eNOS) activity, and greater degradation of NO by reactive oxygen species. 20 The loss of NO-mediated vasodilation promotes increased vascular tone and resistance. In parallel, aging is also associated with activation of the sympathetic nervous system and a chronic pro-inflammatory state, characterized by elevated levels of inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which further exacerbate endothelial dysfunction and arterial stiffness .21,22 Together, these pathophysiological mechanisms contribute to progressive increases in blood pressure with advancing age and may outweigh the modest vascular effects attributable to hemoglobin concentration alone.
In this study, anemia was significantly more prevalent among female participants, and hemoglobin levels were substantially lower in females compared to males. These findings are consistent with global trends and can be attributed to both physiological and hormonal mechanisms. Menstruation is a well-established contributor to iron loss in premenopausal women, leading to gradual depletion of iron stores and increased vulnerability to iron deficiency anemia .23-25 Females also tend to have lower total body iron reserves and reduced hemoglobin mass compared to males, which may be compounded by differences in dietary iron intake and bioavailability .26 During pregnancy, iron demands increase significantly to support expanded plasma volume, placental development, and fetal erythropoiesis, further raising the risk of anemia in women of reproductive age .27 Estrogen has also been shown to modulate erythropoiesis and influence iron metabolism, potentially through suppression of hepatic hepcidin expression, although the underlying regulatory pathways are not yet fully understood.28 These biological factors, together with potential nutritional and socioeconomic disparities, likely account for the higher anemia prevalence observed among females in this cohort. The findings highlight the importance of gender-specific screening protocols and targeted interventions to address anemia in high-risk populations.
Hemoglobin levels did not significantly differ across antihypertensive drug classes in this study. Medications were categorized into angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), calcium channel blockers (CCBs), and beta-adrenergic blockers (beta-blockers). Statistical analysis using the Kruskal-Wallis test revealed no significant variation in hemoglobin concentrations among these groups. This finding aligns with existing literature indicating that most antihypertensive medications do not exert major or consistent effects on hemoglobin levels in patients without significant renal impairment .29
ACEIs and ARBs have been associated with mild anemia in patients with chronic kidney disease due to suppression of the renin-angiotensin-aldosterone system (RAAS) and consequent reduction in erythropoietin (EPO) synthesis .30,31 Angiotensin II plays a supportive role in stimulating EPO production in the renal peritubular interstitial cells. When RAAS is inhibited by these medications, particularly in individuals with impaired renal function, angiotensin II-mediated stimulation of EPO is reduced, potentially leading to decreased erythropoiesis and mild declines in hemoglobin. In patients with preserved kidney function, this effect is typically minimal and may not reach clinical significance (Figure 3).
Beta-blockers and CCBs are not known to influence erythropoiesis or iron metabolism and are rarely associated with hematologic changes. The absence of statistically significant differences in hemoglobin levels in the present analysis may also reflect the small sample size and unequal distribution of patients across drug categories. Further research involving larger cohorts and stratified analysis by renal function, comorbidity, and treatment duration is warranted to clarify whether specific antihypertensive agents exert differential effects on hemoglobin or anemia risk.
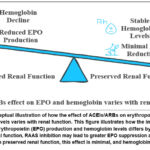 |
Figure 3: Conceptual illustration of how the effect of ACEIs/ARBs on erythropoietin (EPO) and hemoglobin levels varies with renal function. |
This study has several limitations that should be acknowledged. The retrospective design and reliance on medical records may have introduced information bias or incomplete data, particularly regarding medication adherence and treatment duration. The small sample size limits the ability to detect subtle differences between drug classes. Additionally, the study did not assess key confounders such as nutritional status, renal function, or iron markers, which may influence hemoglobin levels. These factors should be addressed in future research using prospective and stratified designs.
Conclusion
This study found that hemoglobin levels showed modest associations with both systolic and diastolic blood pressure; however, hemoglobin did not independently predict hypertension after adjusting for age and gender. Age emerged as the primary determinant of blood pressure variation. Given the high prevalence of anemia, particularly among females, routine screening for hemoglobin abnormalities may improve cardiovascular risk stratification in hypertensive populations. Future research incorporating renal function markers, iron indices, and prospective follow-up is recommended to better clarify potential causal pathways.
Acknowledgment
All authors are thankful to the management of Gulf Medical University and Thumbay Teaching Hospital for providing facilities.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
Ethical approval for this study was obtained from the Institutional Review Board of Gulf Medical University (Ref. No. IRB-COM-FAC-94-2025). The IRB waived the requirement for informed consent because the study involved retrospective review of fully anonymized medical records and posed minimal risk to participants.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources.
Not applicable.
Author contributions
- Rasha Eldeeb, May Khalil, and Mahir Jallo contributed to the conceptualization, methodology, writing original draft, supervision, and proofreading of the final draft.
- Jan Althea Ellao, Tayyaba Fatima Kamal contributed to data collection, analysis, writing review, and editing.
References
- Kario K, Okura A, Hoshide S, et al. The WHO global report 2023 on hypertension: warning of the emerging hypertension burden and treatment strategy. Hypertens Res. 2024;47:1099-1102. doi:10.1038/s41440-024-01622-w
CrossRef - Cappellini MD, Musallam KM, Taher AT. Iron deficiency anemia revisited. J Intern Med. 2020;287(2):153-170.
CrossRef - Anand IS, Gupta P. Anemia and iron deficiency in heart failure. Circulation. 2018;138(1):80-98.
CrossRef - Liu X, Lin B, Yao S, Pan Z. Impact of anemia on cardiovascular events and all-cause death among participants receiving intensive blood pressure treatment: a secondary analysis of SPRINT. Rev Cardiovasc Med. 2024;25(1):6. doi:10.31083/j.rcm2501006
CrossRef - Ghosh T, Rehman T, Ahamed F. Relationship between hemoglobin and blood pressure levels in chronic morbidity among older adults in a developing country: a community-level comparative cross-sectional study. Cureus. 2021;13(11):e19540. doi:10.7759/cureus.19540
CrossRef - Ni W, Yuan X, Sun Y, Zhang H, Zhang Y, Xu J. Anaemia, and associated factors among older adults in an urban district in China: a large-scale cross-sectional study. BMJ Open. 2022;12(3):e056100. doi:10.1136/bmjopen-2021-056100
CrossRef - Roca F, Iacob M, Remy-Jouet I, Bellien J, Joannides R. Evidence for a role of vascular endothelium in control of arterial wall viscosity in humans. Hypertension. 2018;71(1):143-150. doi:10.1161/HYPERTENSIONAHA.117.09870
CrossRef - Siddiqui SW, Ashok T, Patni N, et al. Anemia and heart failure: a narrative review. Cureus. 2022;14(7):e27167. doi:10.7759/cureus.27167
CrossRef - Taha Z, Elhag H, Hassan AA, Adam I. Association between hemoglobin level, anemia, and hypertension among adults in Northern Sudan: a community-based cross-sectional study. Vasc Health Risk Manag. 2024;20:323-331. doi:10.2147/VHRM.S472480
CrossRef - Al-Shamsi S, Al-Bluwi GSM, Al Shamsi M, et al. Prognostic impact of anemia on mortality in United Arab Emirates nationals with cardiovascular disease. Qatar Med J. 2022;2022(1):3. doi:10.5339/qmj.2022.3
CrossRef - Ministry of Health and Prevention. Annual Health Statistical Report. United Arab Emirates; 2022.
- Bazmandegan G, Abbasifard M, Ostadebrahimi H, et al. Positive association between hemoglobin concentration and blood pressure in adults: Rafsanjan Cohort Study. Int J Hypertens. 2023;2023:6283711. doi:10.1155/2023/6283711
CrossRef - Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206-1252.
CrossRef - Lee SG, Rim JH, Kim JH. Association of hemoglobin levels with blood pressure and hypertension: Korea National Health and Nutrition Examination Surveys 2008–2011. Clin Chim Acta. 2015;438:12-18. doi:10.1016/j.cca.2014.07.041
CrossRef - Liu X, Yang C, Zhang X, et al. Association between hemoglobin concentration and hypertension risk in native Tibetans at high altitude. J Clin Hypertens. 2024;26(1):17-23. doi:10.1111/jch.14726
CrossRef - Kim NH, Lee JM, Kim HC, et al. Cross-sectional and longitudinal association between hemoglobin concentration and hypertension: a population-based cohort study. Medicine (Baltimore). 2016;95(41):e5041. doi:10.1097/MD.0000000000005041
CrossRef - Muntner P, He J, Cutler JA, Wildman RP, Whelton PK. Trends in blood pressure among children and adolescents. JAMA. 2004;291(17):2107-2113.
CrossRef - Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease. Circulation. 2003;107(1):139-146.
CrossRef - McEniery CM, Yasmin, Hall IR, et al. Normal vascular aging: differential effects on wave reflection and aortic pulse wave velocity. Hypertension. 2005;45(5):714-718.
- Donato AJ, Morgan RG, Walker AE, Lesniewski LA. Cellular and molecular biology of aging endothelial cells. J Mol Cell Cardiol. 2015;89(Pt B):122-135.
CrossRef - Franceschi C, Campisi J. Chronic inflammation (inflammaging) and its contribution to age-associated diseases. J Gerontol A Biol Sci Med Sci. 2014;69(suppl 1):S4-S9.
CrossRef - Seals DR, Jablonski KL, Donato AJ. Aging and vascular endothelial functions in humans. Clin Sci. 2011;120(9):357-375.
CrossRef - Bothwell TH. Iron requirements in pregnancy and strategies to meet them. Am J Clin Nutr. 2000;72(1)(suppl):257S-264S. doi:10.1093/ajcn/72.1.257S
CrossRef - Camaschella C. Iron deficiency. Blood. 2019;133(1):30-39.
CrossRef - Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harb Perspect Med. 2013;3(7):a011866.
CrossRef - Hou Y, Zhang S, Wang L, et al. Estrogen regulates iron homeostasis through hepatic hepcidin expression via an estrogen response element. Gene. 2012;511(2):398-403. doi:10.1016/j.gene.2012.09.060
CrossRef - Alquaiz AJ, Khoja TA, Alsharif A, et al. Prevalence and correlates of anemia in adolescents in Riyadh city, Kingdom of Saudi Arabia. Public Health Nutr. 2015;18(17):3192-3200. doi:10.1017/S1368980015001214
CrossRef - Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for cardiovascular disease. Circulation. 2003;108(17):2154-2169.
CrossRef - Badura K, Janc J, Wasik J, et al. Anemia of chronic kidney disease: pathophysiology, diagnosis, and management. Biomedicines. 2024;12(6):1191. doi:10.3390/biomedicines12061191
CrossRef - Molnar MZ, Czira ME, Ambrus C, et al. Anemia in kidney transplant recipients: impact on outcomes and association with immunosuppressive therapy. Transplantation. 2011;91(3):294-301.
- Nakhaie S, Yazdani R, Shakibi M, et al. Effects of antihypertensive medications on severity and outcomes of hypertensive patients with COVID-19. J Hum Hypertens. 2022;37(7):511-518.
CrossRef

