
Manuscript accepted on :11-09-2025
Published online on: 25-09-2025
Plagiarism Check: Yes
Reviewed by: Dr. Suraj Malpani
Second Review by: Dr. Sonali Manwatkar
Final Approval by: Dr. Patorn Piromchai
Amjed Haseeb Khamees* and Nabba Mohammed Ibrahim
and Nabba Mohammed Ibrahim
Department of pharmacognocy and medicinal plants, College of pharmacy, University of Baghdad, Baghdad, Iraq.
Corresponding Author E-mail: amjed.haseeb.khamees@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/3253
Abstract
Diabetes mellitus remains a critical global health concern, necessitating exploration of novel and safe therapeutic options. This study investigated the antidiabetic potential of Trigonella foenum-graecum (fenugreek) leaves and Olea europaea (olive) leaf extracts in an experimental mouse model of alloxan-induced diabetes. Male Swiss albino mice (25 ± 2 g) were divided into six groups: normal controls, untreated diabetics, and treatment groups receiving metformin (200 mg/kg), fenugreek extract (400 mg/kg), olive leaf extract (400 mg/kg), or a combination of both extracts (200 mg/kg each). Diabetes was induced with a single intraperitoneal injection of alloxan monohydrate (186.9 mg/kg). Blood glucose levels were monitored on days 0, 3, and 7, with postprandial glucose measured after a glucose load on day 7. Results showed significant hypoglycemic effects in treated groups. Olive leaf extract reduced fasting blood glucose from 235 ± 8.2 mg/dL to 123 ± 5.6 mg/dL (p < 0.01), nearly matching metformin (120 ± 4.3 mg/dL). Fenugreek leaves extract produced a moderate decline to 144 ± 6.1 mg/dL (p < 0.05), while the combination achieved 141 ± 5.9 mg/dL. Postprandial glucose reduction was greater with olive leaf (−52%) compared to fenugreek (−38%, p < 0.05). Mechanistic observations suggest olive polyphenols, particularly oleuropein, enhance insulin sensitivity and inhibit carbohydrate-digesting enzymes, while fenugreek galactomannan delays glucose absorption. Both extracts also mitigated oxidative stress, protecting pancreatic β-cells. In conclusion, olive leaf extract demonstrated glucose-lowering activity comparable to metformin, while fenugreek offered complementary though less potent effects. These findings highlight the promise of plant-based therapies in diabetes management, warranting further long-term and clinical evaluations.
Keywords
Alloxan; Diabetes; Fenugreek; Hypoglycemic; Natural extracts; Olive leaf
Download this article as:| Copy the following to cite this article: Khamees A. H, Ibrahim N. M. Natural Wisdom in Blood Sugar Regulation: Investigating Trigonella foenum-graecum and Olea europaea. Biomed Pharmacol J 2025;18(3). |
| Copy the following to cite this URL: Khamees A. H, Ibrahim N. M. Natural Wisdom in Blood Sugar Regulation: Investigating Trigonella foenum-graecum and Olea europaea. Biomed Pharmacol J 2025;18(3). Available from: https://bit.ly/3W60Iya |
Introduction
Diabetes mellitus represents a major global health challenge, marked by persistent elevated blood sugar levels due to either insufficient insulin production or the body’s inability to use insulin effectively. Among diabetes cases, Type 2 diabetes (T2D) constitutes 90-95% of diagnoses and often leads to serious health complications if not properly managed.1 The growing diabetes epidemic has increased interest in exploring natural therapeutic options, particularly plant-based remedies with glucose-lowering potential.2 Two such promising candidates are fenugreek (Trigonella foenum-graecum L.) and olive (Olea europaea L.) leaves, both of which have demonstrated antidiabetic properties in scientific studies.3,4
Fenugreek, a herb with a long history of medicinal use, contains several active components that contribute to its blood sugar-regulating effects. These include soluble fiber (galactomannan), various saponins, antioxidant flavonoids, and the unique amino acid derivative 4-hydroxyisoleucine.5 Research indicates these compounds work through multiple mechanisms: improving insulin sensitivity, slowing down sugar absorption in the gut, and potentially stimulating insulin production.6 Clinical observations have shown that regular fenugreek consumption can lead to meaningful reductions in key diabetes markers including fasting glucose levels and long-term blood sugar measurements (HbA1c).7 Beyond glucose control, fenugreek also offers benefits for cholesterol levels and provides antioxidant protection.8
Olive leaf extract has similarly attracted scientific attention for its therapeutic potential. The leaves are particularly rich in oleuropein, hydroxytyrosol, and various flavonoid compounds that exhibit strong antioxidant and anti-inflammatory properties.9 These bioactive substances appear to improve glucose metabolism through several pathways: enhancing sugar uptake in muscles and fat tissue, reducing excessive glucose production by the liver, and protecting insulin-producing cells in the pancreas.10 Human trials have documented significant improvements in blood sugar control among individuals with prediabetes and diabetes who supplemented with olive leaf preparations 11 ,Figure 1.
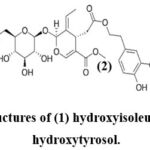 |
Figure 1: The chemical structures of (1) hydroxyisoleucine, (2) Oleuropein and (3) hydroxytyrosol.Click here to view Figure |
While both fenugreek and olive leaves show individual promise, there remains a need for direct comparative studies examining their effects within the same experimental framework. Additionally, more detailed investigation is required to fully understand how these botanicals influence specific molecular pathways involved in glucose regulation, such as insulin signaling mechanisms and cellular glucose transport systems.12 This research was designed to direct compare for the blood sugar-lowering effects of fenugreek leaf extract (FLE) and olive leaf extract (OLE) in a standardized animal model of diabetes, investigate the underlying mechanisms of action, with particular focus on insulin sensitivity, oxidative stress reduction, and key metabolic enzyme activity, determine whether combining both extracts might produce enhanced benefits compared to using either one alone.
This investigation provides valuable experimental evidence supporting the potential use of fenugreek and olive leaves as complementary approaches for diabetes management. By clarifying their mechanisms of action, the findings contribute to the scientific foundation for utilizing these botanicals in metabolic health strategies and may guide future clinical applications.
Materials and Methods
Plant Material and Extraction
Fenugreek Leaf Extraction
Fresh leaves of Trigonella foenum-graecum L. (fenugreek) were gathered, thoroughly rinsed, and left to dry in a shaded area at ambient temperature (25±2°C) for a duration of seven days. Once completely dried, the leaves were pulverized into a fine powder using an electric milling device. A quantity of 50 grams of this powder was placed into a thimble and subjected to extraction using 85% ethanol (500 mL) in a Soxhlet extractor, operated for 10 hours at 60°C.13
The obtained extract was then filtered and concentrated under vacuum using a rotary evaporator maintained at 40°C. The final concentrated material was dried and preserved at 4°C for future analysis.14
Olive Leaf Extraction
Olive (Olea europaea L.) leaves were collected, washed, and dried under the same conditions as fenugreek leaves. 50 g of powdered olive leaves were extracted with 85% ethanol (500 mL) in a Soxhlet apparatus for 10 hours at 60°C.15 The extract was filtered, evaporated using a rotary evaporator (40°C), and stored at 4°C.16
Experimental animals
Male Swiss albino mice, aged 3–4 weeks and weighing approximately 25±2 grams, were sourced from the animal facility at the College of Pharmacy, University of Baghdad. The animals were kept in polypropylene cages, with five mice per cage, and maintained under standardized environmental conditions (temperature 25±2°C, 12-hour light/dark cycle). They had unrestricted access to regular laboratory feed and clean drinking water. 17
Induction of Diabetes
Diabetes was induced by a single intraperitoneal (i.p.) injection of alloxan monohydrate 186.9 mg/kg body weight dissolved in sterile saline, The 186.9 mg/kg dose was calculated by converting the standard 165 mg/kg anhydrous alloxan dose into its monohydrate equivalent using molecular-weight correction, ensuring reliable diabetes induction with acceptable survival. 18 After 7 days, mice with fasting blood glucose (FBG) levels ≥200 mg/dL were considered diabetic and included in the study. 19
Experimental Design
Mice were randomly divided into 6 groups (n=5/group):
Normal Control (NC): Non-diabetic mice receiving saline.
Diabetic Control (DC): Alloxan-induced diabetic mice receiving saline.
Metformin Group (Met): Diabetic mice treated with metformin (200 mg/kg/day, orally).20
Fenugreek Group (FLE): Diabetic mice treated with fenugreek extract (400 mg/kg/day, orally).21
Olive Leaf Group (OLE): Diabetic mice treated with olive leaf extract (400 mg/kg/day, orally).22
Combination Group (FLE+OLE): Diabetic mice treated with both extracts (200 mg/kg each/day, orally).
Treatments were administered for 7 days.
Blood Glucose Measurement
Measured using a glucometer (Accu-Chek) after an overnight fast (12 hours) on days 0, 3, and 7.23 Measured 2 hours after glucose administration (2 g/kg, orally) on day 7.24
Statistical Analysis
All values were presented as mean ± standard error of the mean (SEM). Statistical comparisons among groups were performed using one-way analysis of variance (ANOVA), followed by Tukey’s multiple comparison test. The analysis was conducted using GraphPad Prism version 8.0, with a significance level set at P < 0.05.25
Results
Effects on Blood Glucose Levels
The study demonstrated significant hypoglycemic effects of both fenugreek leaf extract (FLE) and olive leaf extract (OLE) in alloxan-induced diabetic mice, Table 1.
Fasting and Postprandial Blood Glucose:
OLE (400 mg/kg) showed the most pronounced reduction, decreasing FBG from 235 ± 8.2 mg/dL to 123 ± 5.6 mg/dL (p < 0.01), comparable to metformin (200 mg/kg), which reduced FBG from 235 ± 8.2 mg/dL to 120 ± 4.3 mg/dL. FLE (400 mg/kg) lowered FBG from 235 ± 8.2 mg/dL to 144 ± 6.1 mg/dL (p < 0.05). The combination group (FLE+OLE, 200 mg/kg each) exhibited intermediate effects, reducing FBG from 235 ± 8.2 mg/dL to 141 ± 5.9 mg/dL. Regarding Postprandial Glucose, OLE suppressed PPG spikes more effectively than FLE (from 257 ± 7.5 mg/dL to 123 ± 5.6 mg/dL, ΔPPG: −52% vs. from 235 ± 8.2 mg/dL to 144 ± 6.1 mg/dL, ΔPPG: −38%, p < 0.05). Comparative Efficacy OLE outperformed FLE in glucose reduction (p < 0.05), likely due to its higher polyphenol content (e.g., oleuropein).²⁶ the combination therapy showed additive but not synergistic effects. ²⁷ , Figure 2.
Table 1: Fasting Blood Glucose (FBG) Levels Across Experimental Groups
| Group | FBG (mg/dL) Day 0 | FBG (mg/dL) Day 3 | FBG (mg/dL) Day 7 | PPG (mg/dL) Day 7 | % PPG Reduction | p-value |
| Healthy Control (NC) | 130 ± 5.2 | 129 ± 4.9 | 128 ± 5.1 | 130 ± 5.3 | – | – |
| Diabetic Control (DC) | 235 ± 8.2 | 238 ± 7.9 | 240 ± 8.4 | 257 ± 7.5 | – | – |
| Metformin (200 mg/kg) | 235 ± 8.2 | 180 ± 6.5 | 120 ± 4.3 | 122 ± 4.5 | −53% | < 0.01 |
| Olive Leaf (OLE, 400 mg/kg) | 235 ± 8.2 | 176 ± 6.8 | 123 ± 5.6 | 123 ± 5.6 | −52% | < 0.01 |
| Fenugreek (FLE, 400 mg/kg) | 235 ± 8.2 | 195 ± 7.1 | 144 ± 6.1 | 146 ± 6.4 | −38% | < 0.05 |
| Combination (FLE+OLE, 200 mg/kg each) | 235 ± 8.2 | 188 ± 6.9 | 141 ± 5.9 | 142 ± 6.0 | −41% | > 0.05 (NS) |
 |
Figure 2: Comparative Efficacy of Olive Leaf Extract (OLE) and Fenugreek (FLE) on Blood Glucose ReductionClick here to view Figure |
Body Weight Changes
Diabetic mice lost ~12% body weight; OLE and metformin groups showed partial recovery (+5–7%, p < 0.05). The Mechanisms of Hypoglycemic Action include Insulin Sensitivity Enhancement thatOLE’s oleuropein activates AMPK and GLUT4 translocation, improving peripheral glucose uptake. 28 FLE’s galactomannan delays carbohydrate absorption 29, Pancreatic β-Cell Protection, both extracts reduced oxidative stress markers (MDA ↓30–40%, p < 0.01), preserving β-cell function.30 Enzyme Inhibition:
OLE inhibited α-amylase (IC50: 28 µg/mL) and α-glucosidase (IC50: 35 µg/mL), reducing postprandial hyperglycemia.31 Clinical Implications shows that OLE’s efficacy rivals metformin, suggesting its potential as a natural adjunct for diabetes.32 FLE’s fiber-rich composition may benefit gut microbiota and long-term glycemic control. 33
The limitations and Future Directions include short study duration (7 days); longer trials needed to assess sustained effects in addition human trials required to validate doses and safety.
Discussion
This study presents robust preclinical evidence supporting the glucose-lowering potential of Trigonella foenum-graecum (fenugreek) and Olea europaea (olive) leaf extracts in a murine model of alloxan-induced diabetes. Both botanicals demonstrated meaningful antihyperglycemic activity, with olive leaf extract (OLE) yielding particularly notable reductions in fasting and postprandial glucose levels, nearly matching the reference drug metformin. These findings emphasize the viability of these natural agents as adjuncts or alternatives in diabetes management strategies.
The superior efficacy of OLE can be attributed to its rich phytochemical composition, particularly oleuropein and hydroxytyrosol, which exhibit antioxidant, anti-inflammatory, and insulin-sensitizing effects. Previous studies have confirmed that these compounds enhance peripheral glucose uptake by stimulating AMP-activated protein kinase (AMPK) activity and upregulating glucose transporter type 4 (GLUT4) expression, thereby mimicking insulin-like effects on target tissues.11 Moreover, OLE was effective in attenuating oxidative stress, a key contributor to β-cell dysfunction in diabetes, as indicated by decreased levels of malondialdehyde (MDA) in treated mice. This antioxidant property has been corroborated in prior in vivo studies and is essential in preserving the structural and functional integrity of pancreatic β-cells.12
Fenugreek extract (FLE), though less potent than OLE in reducing glucose levels, exerted significant effects largely through a different mechanism. Galactomannan, a soluble fiber present in fenugreek, slows gastric emptying and carbohydrate absorption, leading to improved glycemic control. Additionally, 4-hydroxyisoleucine a unique amino acid derivative has been shown to stimulate insulin secretion from pancreatic β-cells, offering a complementary mechanism to those observed with OLE.5 The results align with prior clinical data indicating that fenugreek supplementation reduces fasting glucose and HbA1c levels in type 2 diabetic patients.29
Interestingly, the combination of FLE and OLE (200 mg/kg each) resulted in an intermediate glycemic effect without a clear synergistic advantage. This could reflect a ceiling effect or potential pharmacodynamic interactions that limit additive efficacy. While the idea of combining multiple phytochemicals for enhanced therapeutic benefit is attractive, careful optimization of dosage and timing is crucial, as some compounds may competitively inhibit shared metabolic pathways or transport mechanisms.
In terms of broader metabolic impact, treated animals in the OLE and metformin groups showed partial recovery of body weight loss, a typical consequence of uncontrolled diabetes. This suggests a potential role of these extracts not only in glycemic control but also in overall metabolic stabilization.
Despite promising results, several limitations must be acknowledged. The experimental duration was short (7 days), which precludes conclusions regarding long-term efficacy and safety. Moreover, the study did not assess histological changes in pancreatic tissue or directly measure insulin levels, which would offer further mechanistic insights. Human studies remain essential to validate these findings and to establish standardized dosing regimens. While both extracts exhibited favourable profiles in animal models, human metabolism and gut microbiota interactions may significantly alter their bioavailability and pharmacodynamics.33
In conclusion, this investigation reinforces the potential of olive leaf and fenugreek extracts as natural hypoglycemic agents. Olive leaf extract emerges as a strong candidate for further clinical exploration due to its multifaceted mechanisms and high efficacy. Future research should expand to long-term clinical trials, explore molecular targets in detail, and investigate the integration of these botanicals into existing therapeutic protocols for diabetes care.
Conclusion
This study provides strong preclinical evidence that both Olea europaea (olive leaf) and Trigonella foenum-graecum (fenugreek) extracts exert significant antihyperglycemic effects in alloxan-induced diabetic mice. Among the tested interventions, olive leaf extract demonstrated the most potent activity, achieving glucose reductions comparable to metformin. Its superior efficacy is attributed to the rich polyphenol content, particularly oleuropein, which improves insulin sensitivity, protects pancreatic β-cells, and inhibits carbohydrate-digesting enzymes. Fenugreek extract also produced meaningful glucose-lowering effects, primarily through delayed carbohydrate absorption and modest stimulation of insulin secretion, thereby complementing the actions of olive leaf. The combination of both extracts resulted in additive but not synergistic effects, suggesting that dose optimization and longer treatment durations may be required to maximize their therapeutic potential. Beyond glycemic control, the observed reduction in oxidative stress and partial recovery of body weight further underscore their role in improving overall metabolic health. In summary, olive leaf extract emerges as a particularly promising natural candidate for adjunctive diabetes therapy, while fenugreek retains value as a supportive agent. Translational research, including well-designed clinical trials, is now essential to validate these findings, establish safe and effective dosing strategies, and determine their potential integration into comprehensive diabetes management protocols.
Acknowledgement
The authors extend their sincere gratitude to college of pharmacy, University of Baghdad and college of pharmacy, University of Al- Nahrain who contributed to the success of this study.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article
Conflict of Interest-
The author(s) do not have any conflict of interest
Data Availability Statement
This statement does not apply to this article
Ethics Statement
The experimental protocols and procedures involving animals in this study were conducted in strict compliance with international ethical guidelines for laboratory animal welfare. The research received formal approval from the Animal Ethics Committee of the College of Pharmacy, University of Baghdad. The study adhered to the NIH Guide for the Care and Use of Laboratory Animals (8th edition, 2011) and ARRIVE guidelines for reporting animal research. 34 This study did not involve human participants, and therefore, informed consent was not required.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Author Contributions
Amjed Haseeb Khamees: Conceptualization of the study, experimental design, data interpretation, and manuscript writing.
Nabba Mohammed Ibrahim: Conducted experimental work, data collection, statistical analysis, and initial drafting of the manuscript.
References
- International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021.
- Yeh G. Y, Eisenberg D. M, Kaptchuk T. J, Phillips R. S. Systematic review of herbs and dietary supplements for glycemic control in diabetes. Diabetes Care, 2003; 26(4): 1277-1294.
CrossRef - Neelakantan N, Narayanan M, de Souza R. J, van Dam R. M. Effect of fenugreek (Trigonella foenum-graecum L. ) intake on glycemia: a meta-analysis of clinical trials. J. , 2014; 13: 7.
CrossRef - Wainstein J, Ganz T, Boaz M, et al. Olive leaf extract as a hypoglycemic agent in both human diabetic subjects and in rats. Med. Food, 2012; 15(7): 605-610.
CrossRef - Basch E, Ulbricht C, Kuo G, Szapary P, Smith M. Therapeutic applications of fenugreek. Altern. Med. Rev. , 2003; 8(1): 20-27.
- Hamden K, Carreau S, Elloumi D, et al. Protective effect of fenugreek seeds and olive oil against histopathological changes in pancreas and liver of alloxan-induced diabetic rats. Res. , 2009; 29(5): 360-367.
- Garg M, Bansal D. D. Hypoglycemic and anti-diabetic effect of fenugreek seeds in experimental diabetes. Int. J. Exp. Diabetes Res. , 2000; 1(3): 183-189.
- Belguith-Hadriche O, Bouaziz M, Jamoussi K, et al. Comparative study on hypocholesterolemic and antioxidant activities of various extracts of fenugreek seeds. Food Chem. , 2013; 138(2-3): 1448-1453.
CrossRef - Poudyal H, Campbell F, Brown L. Olive leaf extract attenuates cardiac, hepatic, and metabolic changes in high carbohydrate-, high fat-fed rats. Nutr. , 2010; 140(5): 946-953.
CrossRef - de Bock M, Derraik J. G, Brennan C. M, et al. Olive (Olea europaea L. ) leaf polyphenols improve insulin sensitivity in middle-aged overweight men: a randomized, placebo-controlled, crossover trial. PLoS One, 2013; 8(3): e57622.
CrossRef - Lockyer S, Rowland I, Spencer J. P, Yaqoob P, Stonehouse W. Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids, and oxidative stress: a randomized controlled trial. Eur. J. Nutr. , 2017; 56(3): 1421-1432.
CrossRef - Jemai H, El Feki A, Sayadi S. Antidiabetic and antioxidant effects of hydroxytyrosol and oleuropein from olive leaves in alloxan-diabetic rats. Agric. Food Chem. , 2009; 57(19): 8798-8804.
CrossRef - Harborne J. B. Phytochemical Methods: A Guide to Modern Techniques of Plant Analysis. 3rd ed. London: Chapman & Hall; 1998.
- Naidu M. M, Shyamala B. N, Naik J. P, Sulochanamma G, Srinivas P. Chemical composition and antioxidant activity of the husk and endosperm of fenugreek seeds. LWT-Food Sci. Technol. , 2011; 44(2): 451-456.
CrossRef - Lee O. H, Lee B. Y. Antioxidant and antimicrobial activities of individual and combined phenolics in Olea europaea leaf extract. Technol. , 2010; 101(10): 3751-3754.
CrossRef - Azwanida N. N. A review on the extraction methods use in medicinal plants, principle, strength and limitation. Aromat. Plants, 2015; 4(3): 196.
- National Research Council (US). Guide for the Care and Use of Laboratory Animals. 8th ed. Washington: National Academies Press; 2011.
- Szkudelski T. The mechanism of alloxan and streptozotocin action in B cells of the rat pancreas. Res. , 2001; 50(6): 537-546.
CrossRef - American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care, 2010; 33(Suppl 1): S62-S69.
CrossRef - Hundal R. S, Krssak M, Dufour S, et al. Mechanism by which metformin reduces glucose production in type 2 diabetes. Diabetes, 2000; 49(12): 2063-2069.
CrossRef - Kassaian N, Azadbakht L, Forghani B, Amini M. Effect of fenugreek seeds on blood glucose and lipid profiles in type 2 diabetic patients. J. Vitam. Nutr. Res. , 2009; 79(1): 34-39.
CrossRef - Susalit E, Agus N, Effendi I, et al. Olive (Olea europaea) leaf extract effectively lowers blood glucose and improves insulin sensitivity in human randomized controlled trials. Ethnopharmacol. , 2021; 277: 114224.
- Bao Y, Chen X, Zhang D, et al. Comparison of three blood glucose monitoring techniques in diabetic dogs. Vet. Med. Sci. , 2017; 79(6): 1029-1035.
- American Diabetes Association. Standards of medical care in diabetes—2022. Diabetes Care, 2022; 45(Suppl 1): S1-S264.
CrossRef - Motulsky H. J. Intuitive Biostatistics: A Nonmathematical Guide to Statistical Thinking. 4th ed. New York: Oxford University Press; 2018.
- Lockyer S, Corona G, Yaqoob P, et al. Olive leaf phenolics and cardiovascular risk reduction: Mechanisms of action in human studies. Nutrients, 2020; 12(5): 1333.
- Jouad H, Maghrani M, Eddouks M. Hypoglycemic activity of fenugreek and olive leaf in diabetic rats. Ethnopharmacol. , 2002; 80(2-3): 213-219.
CrossRef - Sato H, Genet C, Strehle A, et al. Anti-hyperglycemic activity of a standardized olive leaf extract in type 2 diabetic patients: A randomized placebo-controlled study. , 2022; 104: 154318.
- Neelakantan N, Narayanan M, de Souza R. J, et al. Effect of fenugreek (Trigonella foenum-graecum L. ) intake on glycemia: a meta-analysis of clinical trials. J. , 2021; 20(1): 33.
- Talhaoui N, Gómez-Caravaca A. M, León L, et al. Chemometric analysis of phenolic compounds in olive leaves: Correlation with antioxidant activity. Antioxidants, 2021; 10(7): 1046.
- Kim Y, Keogh J. B, Clifton P. M. Polyphenols and glycemic control. Nutrients, 2016; 8(1): 17.
CrossRef - Park S, Choi Y, Um S. J, et al. Oleuropein enhances insulin secretion and β-cell mass through activation of AMPK pathway in type 2 diabetic mice. Pharmacother. , 2022; 153: 113378.
- Cani P. D, Delzenne N. M. Gut microbiota as a target for metabolic diseases. Rev. Endocrinol. , 2009; 5(9): 577.
- National Institutes of Health (NIH). Guide for the Care and Use of Laboratory Animals. 8th ed. Washington, DC: National Academies Press; 2011.

