
Manuscript accepted on :12-09-2025
Published online on: 26-09-2025
Plagiarism Check: Yes
Reviewed by: Dr. Salma Rattani
Second Review by: Dr. Raju Thenge
Final Approval by: Dr. Prabhishek Singh
Abdelhaq Barbach1* , Youssef Ikken2,3, Yahya Charrah1,4, Anas Ansari Chenguiti1,4,5, Ouiam Dahmane1, Rachid Alami6and Amina Barkat1,4,7
, Youssef Ikken2,3, Yahya Charrah1,4, Anas Ansari Chenguiti1,4,5, Ouiam Dahmane1, Rachid Alami6and Amina Barkat1,4,7
1Department of Biomedical Sciences, Abulcasis International University of Health Sciences, Rabat, Morocco
2Department of Public Health, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco
3Department of Research, Higher Institute of Nursing Professions and Health Techniques (ISPITS), Ministry of Health and Social Protection, Rabat, Morocco.
4Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco
5Department of Obstetrics and Gynecology, Sheikh Zaid International University Hospital, Rabat, Morocco
6Department of Management, Abu Dhabi School of Management, Abu Dhabi, United Arab Emirates
7Department of Neonatology and Nutrition, National Reference Center, Ibn Sina Rabat Children's Hospital, Rabat, Morocco
Corresponding Author E-mail: barbachabdelhaq@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/3262
Abstract
This study evaluated the face validity, content validity, and applicability of a newly developed Therapeutic Patient Education (TPE) workbook for gestational diabetes (GD) in Morocco. GD is an increasing public health concern requiring a multidimensional approach integrating biomedical, educational, and psychosocial aspects, with TPE as a key component. A cross-sectional mixed-methods study combining quantitative and qualitative approaches was conducted with 35 experts from various disciplines (gynecologists, endocrinologists, nutritionists, psychologists, public health specialists, and nurse managers) in the Rabat-Salé-Kénitra region. The evaluation questionnaire comprised five dimensions: scientific relevance, pedagogical methodology, diagnostic educational tools, clinical feasibility, and psychosocial-economic adaptability, using a five-point Likert scale and open-ended questions. Quantitative analysis (Cronbach’s alpha = 0.82; overall mean score = 4.09 out of 5; Kruskal–Wallis tests) and qualitative thematic analysis (29 identified themes for improvement) were conducted. The workbook was validated across all five dimensions, indicating satisfactory acceptance. Scientific relevance received the highest ratings (mean = 4.56 out of 5), particularly for content on nutrition, physical activity, and glucose self-monitoring. Experts recommended improvements in content clarity, personalization of materials, cultural appropriateness, and adaptability to clinical constraints. Suggestions included adding summary sheets, decision-making algorithms, digital resources, and context-specific adaptations. Following these revisions, further validation with healthcare professionals and patient evaluations will be conducted to confirm the workbook’s alignment with practical educational needs and enhance its implementation in Arabic-speaking contexts.
Keywords
Cultural adaptation; Educational tool validation; Gestational diabetes; Gestational diabetes tools; Maternal health education; Psychosocial factors; Therapeutic patient education
Download this article as:| Copy the following to cite this article: Barbach A, Ikken Y, Charrah Y, Chenguiti A. A, Dahmane O, Alami R, Barkat A. Expert-Based Content Validation of a Culturally Adapted Therapeutic Education Workbook for Gestational Diabetes in Moroccan and Arabic-speaking Contexts. Biomed Pharmacol J 2025;18(3). |
| Copy the following to cite this URL: Barbach A, Ikken Y, Charrah Y, Chenguiti A. A, Dahmane O, Alami R, Barkat A. Expert-Based Content Validation of a Culturally Adapted Therapeutic Education Workbook for Gestational Diabetes in Moroccan and Arabic-speaking Contexts. Biomed Pharmacol J 2025;18(3). Available from: https://bit.ly/4mBbB5V |
Introduction
Gestational diabetes (GD) is characterized by impaired glucose tolerance leading to hyperglycemia that occurs during pregnancy. According to the World Health Organization (WHO), this definition encompasses both true GD and previously undiagnosed type 2 diabetes (T2D) identified during pregnancy, regardless of treatment initiation or postpartum progression.1
Internationally, the prevalence of GD varies considerably, with notably high rates reported in Arabic-speaking countries, ranging from 5.1% in Yemen to over 24.9% in the United Arab Emirates, and even reaching up to 37.7% among certain high-risk populations.2,3 In Morocco, the prevalence of GD is also increasing, driven primarily by rising metabolic risk factors. However, the heterogeneity of screening practices and the absence of standardized diagnostic criteria contribute significantly to underdiagnosis, leading to greater maternal and neonatal complications.4
The management of GD, typically focused on medical interventions such as blood glucose monitoring and pharmacological treatment, may be insufficient without an integrated multidisciplinary approach.5 Approximately 70–85% of women with GD can achieve adequate glycemic control through non-pharmacological interventions, including personalized nutritional strategies, regular physical activity, and self-monitoring of blood glucose.6 Although nutrition remains a cornerstone of this approach, successful dietary management requires patients to make sustained behavioral changes.7 However, dietary counseling alone has been shown to be insufficient to substantially improve maternal and neonatal outcomes.8
Therapeutic Patient Education (TPE), defined by WHO as a continuous, integrated care process comprising information, education, and psychosocial support,9 has proven effective in improving health behaviors, disease self-management, and quality of life, especially in high-income countries.10 However, in Arabic-speaking contexts (including Morocco), TPE remains underutilized, primarily due to a lack of culturally and linguistically appropriate educational tools, limited awareness among healthcare professionals, and a shortage of trained educators.11 Cultural factors such as religious beliefs, family norms, and social perceptions further highlight the need for context-specific educational materials. Consequently, the WHO Regional Framework for Diabetes Prevention explicitly recommends culturally tailored programs.12
In Morocco, despite national strategic commitments, TPE implementation remains limited, mainly due to incomplete understanding of its principles and persistent methodological shortcomings among healthcare professionals.13 Although various TPE programs have been implemented for chronic conditions such as diabetes,14 asthma,15,16 rheumatoid arthritis,17 psychiatric disorders,18 and Human Immunodeficiency Virus (HIV),19,20 within the National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases (2019–2029), structured and culturally adapted tools specifically designed for GD remain absent.21
A recent African review highlighted that limited access to GD education, especially face-to-face interventions, is a critical barrier, underscoring the need for structured TPE programs in such settings.22 To date, there is no validated, multidisciplinary, culturally adapted TPE tool for GD patients specifically developed for Morocco or broader Arabic-speaking populations. This gap significantly undermines patient-centered diabetes care strategies.23 For instance, a recent North African randomized trial showed that a culturally tailored GD education program significantly improved maternal and neonatal outcomes.24 However, no comparable comprehensive program has been developed or implemented in Morocco, accentuating this gap.
This study aims to (1) evaluate the scientific, methodological, and practical quality of a newly developed TPE workbook for GD; (2) assess expert acceptability and feasibility of its clinical implementation; and (3) identify key areas for improvement through a combination of quantitative scoring and thematic analysis.
The workbook was developed following guidelines from the French National Authority for Health (HAS) and WHO and based on a comprehensive literature review, and then evaluated by a multidisciplinary panel of experts in gynecology, endocrinology, nutrition, psychology, public health, and nursing management. Ultimately, this research seeks to bridge the gap related to validated and culturally adapted GD education tools in Morocco and comparable Arabic-speaking settings. By providing a rigorously evaluated, context-specific educational resource, this study aims to enhance GD management through improved patient education and facilitate its integration into maternal healthcare practices.
Materials and Methods
Type of study and context
This study adopted a mixed-method, cross-sectional observational, descriptive, and analytical design, conducted in the Rabat-Sale-Kenitra region of Morocco. A mixed-methods approach was used to capture both structured expert ratings and open-ended feedback, thereby enhancing content validity and providing a nuanced understanding of the workbook’s cultural and contextual appropriateness. The quantitative component assessed the workbook’s scientific quality, clarity, methodology, and practical feasibility through a structured questionnaire. The qualitative component involved thematic analysis of open-ended expert feedback to identify specific suggestions for improvement. This study forms part of a broader effort to enhance the pedagogical quality of educational tools in maternal health, in alignment with the recommendations of HAS and WHO on TPE.
Study setting and duration
The study was conducted in the Rabat-Sale-Kenitra region (Morocco), across both public and private sectors, from August 2024 to February 2025. Participating experts were affiliated with the following institutions: the Ministry of Health, the Directorate of Population, the Directorate of Epidemiology and Disease Control (DELM), the Cheikh Zaid International University Hospital (Rabat), the Mohammed V Military Hospital (Rabat), Souissi Maternity Hospital (Rabat), Orangers Hospital (Rabat), Avicenne Hospital (Rabat), as well as several private medical practices located in Rabat, Sale, and Temara.
Design of the educational workbook
The evaluated workbook was developed according to the methodological principles of the HAS and WHO, which structure TPE into four key steps:
Initial educational diagnosis
Negotiation of learning objectives
Implementation of educational activities
Final program evaluation
Its design was based on
Recent clinical guidelines on gestational diabetes
A review of the international literature
Established TPE pedagogical frameworks
The workbook is composed of two main components. First, a structured TPE program focused on developing self-management skills, including modules on understanding GD, healthy nutrition, appropriate physical activity, stress management techniques, blood glucose self-monitoring, and therapeutic management.
Second, a personalized TPE program provides operational tools for individualizing educational follow-ups. These include an educational diagnosis grid to guide initial patient assessment, a summary sheet of identified educational needs, a model educational contract to formalize objectives with the patient, an implementation guide for healthcare providers, and a post-TPE evaluation grid to assess progress and outcomes.
Participants and sampling
A multidisciplinary panel of 35 experts was assembled through purposive sampling, ensuring balanced representation of specialties involved in TPE, maternal health, diabetology, and public health. The panel comprised 6 obstetrician-gynecologists, 6 endocrinologists, 6 psychologists, 6 nutritionists, 6 healthcare managers (including 3 midwives and 2 quality-of-care coordinators), and 5 public health and epidemiology experts.
Although content validation studies commonly recommend panels of 5 to 10 members.25 We deliberately included a larger and more diverse group to enrich disciplinary perspectives and achieve greater thematic saturation of expert feedback. Indeed, qualitative research often reaches saturation with fewer participants; thus, involving 35 experts was expected to comprehensively capture insights across multiple specialties.26 Furthermore, some authors specifically suggest panels of approximately 25–30 experts for robust content validation,27 which further supports our methodological choice. This approach aimed to strengthen both the reliability and credibility of the validation process.
However, the panel predominantly comprised professionals from urban institutional and private-sector settings. Therefore, perspectives from rural, lower-resource, and primary care environments may be underrepresented, constituting a potential source of selection bias.
Eligibility criteria
Inclusion criteria
Minimum of 5 years of professional experience
Expertise in health education, diabetes, perinatal care, or public health
Availability to participate in a thorough evaluation process
Exclusion criteria
Less than 5 years of professional experience in the relevant fields
Unavailability to devote sufficient time to reviewing the workbook and completing the entire questionnaire.
Data collection and evaluation instrument
The questionnaire was developed based on the quality criteria defined by HAS for TPE programs. A preliminary pilot test was conducted with three independent experts to assess face validity and enhance the clarity, structure, and relevance of the evaluation items. This step aimed to optimize:
The wording and precision of the items
The systematic inclusion of open-ended questions to gather expert suggestions
The logical organization of sections in alignment with the four-step TPE methodology.
Following the pilot test, several refinements were made to improve item phrasing, ensure layout consistency across sections, and enhance the structure of the open-ended comment fields. All modifications were documented and integrated before final dissemination. Initially, the questionnaire included 16 Likert-scale items and one open-ended question. Based on the experts’ feedback, four additional Likert-scale items were added (bringing the total to 20), and the questionnaire was reorganized into five thematic axes. Each Likert-scale item was followed by an open-ended question, allowing experts to provide specific comments and suggestions for improvement.
The first expert recommended including a comment field after each Likert item, especially to clarify the rationale behind low scores. The second expert advised aligning the questionnaire with the four-step TPE methodology and adding an introductory note encouraging comments even when high ratings were assigned. The third expert proposed removing redundant questions and reordering items to improve logical flow, for example, by fully assessing the educational diagnosis grid before addressing tools for negotiating learning objectives. All suggestions were adopted, resulting in enhanced item clarity, a more coherent distribution across thematic axes, and overall improvement in the questionnaire’s structure and usability.
The study assessed face and content validity using a multidisciplinary panel. Face validity was defined as the extent to which experts found the material appropriate, relevant, and understandable. Content validity was defined as the extent to which the workbook comprehensively covered the necessary domains of GD education, including pedagogical and cultural aspects. No further psychometric testing was performed at this stage.
The final questionnaire included 20 items, grouped into five thematic axes, each rated on a 5-point Likert scale (1 = Very insufficient, 5 = Very sufficient). Each item was accompanied by an open-ended question designed to elicit qualitative comments, suggestions for improvement, or specific critiques from the experts. The following table summarizes the five thematic axes and their associated evaluation variables.
Table 1: Axis and variables of the TPE-GD workbook evaluation questionnaire
| Axis | Variable | Variable Code | |
| 1 | Relevance and Scientific Basis | Content relevance according to recommendations | RSB 1 |
| Currency of the data used | RSB 2 | ||
| Adequacy of professional competencies | RSB 3 | ||
| Clarity and structure of the content | RSB 4 | ||
| 2 | Methodology and Program Personalization | Compliance with TPE methodological standards | MPP 1 |
| Adaptation of the 4-step methodology to gestational diabetes | MPP 2 | ||
| Adaptation of tools and methods to objectives | MPP 3 | ||
| Personalization based on patient needs | MPP 4 | ||
| 3 | Educational Diagnosis and Learning Objectives | Ability of the grid to identify educational priorities | EDO 1 |
| Ease of use of the grid by professionals | EDO 2 | ||
| Ability of the grid to identify learning barriers | EDO 3 | ||
| Ease of using tools in goal negotiation | EDO 4 | ||
| 4 | Program Implementation and Evaluation | Adaptation of the workbook to clinical constraints | PIE 1 |
| Practical usefulness for healthcare professionals | PIE 2 | ||
| Ability of evaluation tools to measure progress | PIE 3 | ||
| Relevance of self-assessment tools | PIE 4 | ||
| 5 | Adaptation and Psychosocial-Economic Factors | Consideration of the psychosocial aspects of gestational diabetes | APF 1 |
| Capacity of tools to integrate economic and cultural specificities | APF 2 | ||
| Relevance of tools for family involvement | APF 3 | ||
| Integration of tools to enhance self-confidence | APF 4 |
Evaluation procedures
After finalizing the questionnaire, each expert received a file, either electronically or in person, containing the TPE-GD workbook, an introductory sheet (outlining the objectives, instructions, and participation guidelines), and the questionnaire to complete. A two-week period was granted to allow for a thorough review of the material and independent completion of the questionnaire, in accordance with confidentiality requirements.
Responses were collected using two complementary methods:
By return of the completed digital file sent via email (in Word or PDF format)
Through individual face-to-face interviews, especially for experts who preferred guided discussion or were met at their workplace.
The Excel tool used for data entry was structured into two separate spreadsheets:
Sheet 1: Entry of numerical ratings assigned to the 20 variables using a Likert scale (scores from 1 to 5)
Sheet 2: Full transcription of responses to open-ended questions
These open-ended questions, placed after each axis of the questionnaire, aimed to collect qualitative feedback, suggestions for improvement, specific critiques, or proposals for adaptation freely expressed by the experts. They enriched the analysis by providing contextual insights into the numerical scores and guided the subsequent methodological adjustments of the workbook. Special attention was given to the diversity of the verbatim comments collected, ensuring thematic grouping and traceability by axis and by specialty.
Data analysis
Quantitative analysis
Internal reliability: Cronbach’s alpha coefficient was used to assess the consistency of responses globally and by thematic axis (a threshold between 0.5 and 0.6 was considered acceptable, and a threshold > 0.6 was considered indicative of good consistency).
Descriptive analysis: Quantitative data were computed using the Jamovi software (v2.3.28) to obtain means, standard deviations, and score frequencies by disciplinary group.
Intergroup comparisons: The non-parametric Kruskal–Wallis test was used to examine score differences based on experts’ specialties, years of professional experience, and prior TPE training. Normality was assessed using the Shapiro–Wilk test (p < 0.001). Given the number of comparisons conducted, results were interpreted with caution, and Bonferroni-adjusted p-values were applied where appropriate to control for type I error.
All statistical tests were performed with a type I error rate of α = 5%.
A p-value < 0.05 was considered statistically significant.
Qualitative analysis
To ensure the reliability of the qualitative analysis, a rigorous coding process was implemented. Two researchers (AB and YI) independently coded all open-ended responses using an inductive approach based on Braun and Clarke’s framework.28 Following this initial phase, they held a consensus meeting to compare their coding frameworks. Discrepancies, which represented approximately 12% of the initial codes, were systematically discussed. For each point of disagreement, the original expert feedback was re-read, and a consensus code was either chosen or created. This iterative process continued until 100% agreement was reached on the final codebook. This transparent procedure strengthens the credibility of the thematic analysis.
Ethical aspects and regulatory compliance
The study was conducted in accordance with the ethical principles applicable to non-interventional research. All participants were informed in writing about the study’s objectives and assurances of confidentiality. Free and informed consent was obtained from each expert. In accordance with Moroccan Law No. 28.13 and article 2 of the National Ethics Guidelines for Non-Interventional Studies, formal ethical approval was not required. Nonetheless, good research practices were strictly followed throughout the process, including respect for anonymity, data protection, and voluntary participation.
Results
Quantitative results
Internal reliability
The TPE-GD workbook showed good overall consistency (Cronbach’s alpha = 0.820). However, two axes had values around 0.5, indicating moderate internal consistency for those subscales.
Table 2: Cronbach’s Alpha coefficients by thematic axis of the questionnaire
| Axis | Variables | Cronbach’s α |
| Relevance and Scientific Basis | RSB 1 – RSB 4 | 0.67 |
| Methodology and Program Personalization | MPP 1 – MPP 4 | 0.57 |
| Educational Diagnosis and Objectives | EDO 1 – EDO 4 | 0.52 |
| Implementation and Evaluation | PIE 1 – PIE 4 | 0.72 |
| Psychosocial and Cultural Adaptation | APF 1 – APF 4 | 0.63 |
| Global Questionnaire (20 items) | RSB 1 – APF 4 | 0.82 |
General characteristics of the sample
The study was conducted with 35 experts from various specialties, backgrounds, and professional experiences.
Specialty distribution: The sample included a balanced representation from disciplines involved in therapeutic patient education (TPE).
Age distribution: The majority of participants (48.6%) were aged between 40 and 49 years, followed by those aged 30 to 39 years (31.4%).
Professional experience: 62.9% of experts had over 15 years of professional experience.
Training in TPE: Less than half of the experts (45.7%) had received specific training in TPE.
Table 3: Expert characteristics
| Category | Count | % of Total | |
| Specialty | Health managers | 6 | 17.1 % |
| Endocrinology – Diabetology | 6 | 17.1 % | |
| Obstetrics and Gynecology | 6 | 17.1 % | |
| Nutrition and Dietetics | 6 | 17.1 % | |
| Psychology | 6 | 17.1 % | |
| Public Health | 5 | 14.3 % | |
| Age group | 30–39 years | 11 | 31.4 % |
| 40–49 years | 17 | 48.6 % | |
| 50–59 years | 3 | 8.6 % | |
| 60 years and over | 2 | 5.7 % | |
| Under 30 years | 2 | 5.7 % | |
| Gender | Female | 22 | 62.9 % |
| Male | 13 | 37.1 % | |
| Professional experience | More than 15 years | 22 | 62.9 % |
| 10–15 years | 5 | 14.3 % | |
| 5–10 years | 8 | 22.9 % | |
| Training in TPE | Yes | 16 | 45.7 % |
| No | 19 | 54.3% |
Workbook evaluation: Scores and comparisons
The table below presents the average scores attributed to each specialty and evaluation axis.
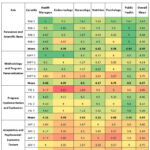 |
Table 4: Mean scores assigned to the evaluation variables of the TPE-GD workbookClick here to view Figure |
The analysis of the average scores assigned to the various dimensions of the TPE-GD workbook highlights the following trends:
Relevance and Scientific Basis: Average score of 4.56; all related variables show values above 4.
Methodology and Program Personalization: Average score of 4.27; the variable program personalization (MPP 4) scored slightly lower at 3.75.
Educational Diagnosis and Learning Objectives: Average score of 4.03; the identification of learning barriers (EDO 3) received a lower score of 3.73.
Program Implementation and Evaluation: Average score of 4.04; the lowest-rated variable in this axis was adaptation of the workbook to clinical constraints (PIE 1), with a score of 3.05.
Adaptation and Psychosocial-Economic Factors: Average score of 3.55; all variables scored below 4, with the lowest being family involvement (AFP 3) at 3.16.
Group comparison: Statistical analysis
Due to the non-normal distribution confirmed by the Shapiro–Wilk test (p < 0.001), the Kruskal–Wallis test was used for comparison between groups.
The results are summarized in the following table:
Table 5: Comparison of variables according to specialty, experience, and participation in TPE training
| Variable | Specialty (χ², p) | Experience (χ², p) | TPE training (χ², p) |
| RSB 1 | 9.21 (0.101) | 3.471 (0.176) | 0.490 (0.484) |
| RSB 2 | 4.94 (0.424) | 6.518 (0.038) | 0.774 (0.379) |
| RSB 3 | 5.19 (0.393) | 0.802 (0.670) | 0.913 (0.339) |
| RSB 4 | 12.19 (0.032) | 0.522 (0.770) | 4.261 (0.039) |
| MPP 1 | 11.86 (0.037) | 5.058 (0.080) | 0.126 (0.722) |
| MPP 2 | 3.20 (0.669) | 7.837 (0.020) | 4.607 (0.032) |
| MPP 3 | 6.43 (0.267) | 0.113 (0.945) | 0.153 (0.696) |
| MPP 4 | 7.15 (0.210) | 0.301 (0.860) | 0.000 (1.000) |
| EDO 1 | 1.18 (0.947) | 1.39 (0.500) | 0.194 (0.660) |
| EDO 2 | 1.93 (0.858) | 2.05 (0.358) | 0.196 (0.658) |
| EDO 3 | 6.46 (0.264) | 2.60 (0.272) | 1.419 (0.234) |
| EDO 4 | 4.41 (0.492) | 1.33 (0.513) | 0.326 (0.568) |
| PIE 1 | 1.18 (0.947) | 1.39 (0.500) | 0.194 (0.660) |
| PIE 2 | 1.93 (0.858) | 2.05 (0.358) | 0.196 (0.658) |
| PIE 3 | 6.46 (0.264) | 2.60 (0.272) | 1.419 (0.234) |
| PIE 4 | 4.41 (0.492) | 1.33 (0.513) | 0.326 (0.568) |
| APF 1 | 2.01 (0.848) | 2.45 (0.294) | 4.626 (0.031) |
| APF 2 | 3.76 (0.585) | 1.40 (0.496) | 9.263 (0.002) |
| APF 3 | 6.16 (0.291) | 2.06 (0.357) | 0.606 (0.436) |
| APF 4 | 2.86 (0.722) | 2.35 (0.309) | 3.39 (0.985) |
Regarding scientific relevance, significant differences were observed. Professional experience influenced the evaluation of the currency of the data used (RSB 2, p = 0.038), while TPE training affected perceptions of the clarity and structure of the content (RSB 4, p = 0.039). A variation by specialty was also noted for content clarity (RSB 4, p = 0.032).
In terms of methodology and program personalization, specialty influenced the assessment of compliance with TPE methodological standards (MPP 1, p = 0.037). Furthermore, both professional experience (MPP 2, p = 0.020) and TPE training (MPP 2, p = 0.032) significantly impacted evaluations of the adaptation of the methodology to GD specificities.
For the axis related to educational diagnosis and learning objectives, no statistically significant differences were found across specialty, professional experience, or TPE training.
Similarly, for program implementation and evaluation, no significant differences were reported for any of the assessed variables.
Concerning adaptation to psychosocial and economic factors, TPE-trained experts gave lower scores for both the consideration of psychosocial dimensions (APF 1, p = 0.031) and the program’s ability to integrate cultural and economic specificities (APF 2, p = 0.002).
Qualitative results
Responses to the open-ended questions generated a series of expert recommendations aimed at improving the TPE-GD workbook. These qualitative insights complemented the quantitative findings by identifying specific dimensions requiring refinement. A manual thematic analysis was conducted to classify the responses according to the five axes of the evaluation grid, revealing recurrent suggestions, points of divergence, and areas for enhancement.
One of the most prominent themes concerned the need to simplify the workbook’s content to enhance its usability in clinical settings. This issue, particularly salient for variable RSB 4 (Clarity and structure), was underscored by several experts. An endocrinologist remarked: “The workbook gives too many details, which sometimes makes it difficult for the user to extract relevant information in a simple way.” This was echoed by a midwife who noted: “We need simplified materials for the patients.”
A second frequently cited issue was the insufficient integration of family support mechanisms, especially under variable APF 3 (Family involvement). In reference to sociocultural norms, a psychologist observed: “In our culture, the patient is not alone—decisions about food and health are often made by the husband or the mother-in-law. The workbook speaks only to the patient.” A gynecologist added that the development of “specific tools for the patient’s support system” would be highly beneficial.
Regarding the methodological dimension (MPP 2), many experts highlighted the challenge of implementing the four-step educational process within the constraints of routine consultations. One respondent stated: “This four-step method is time-consuming; we need to adapt it to the reality of short consultations.” Another expert emphasized the importance of timely implementation, stating: “The program must be implemented quickly after diagnosis to avoid complications for the mother and the fetus.”
For variable EDO 1 (Identifying educational priorities), experts emphasized the importance of incorporating tools that allow patients to articulate their needs. Recommendations included the use of open-ended questions and patient-completed diagnostic grids to facilitate this process. Regarding the methodological dimension (MPP 2), time constraints were frequently cited. One expert noted: “This four-step method is time-consuming; we need to adapt it to the reality of short consultations.” Another participant added: “The program must be implemented quickly after diagnosis to avoid complications for the mother and the fetus.”
The most frequently cited recommendations, grouped by theme, are summarized below:
Simplify and streamline content for ease of use by non-specialist educators.
Adapt materials to local socio-economic contexts for better relevance.
Strengthen psychosocial support mechanisms (stress management, emotional support, family involvement).
Enhance interprofessional coordination and define clear roles within the team.
Provide patient-centered educational tools (patient booklets, summary sheets, decision aids).
 |
Figure 1: Heatmap matrix of recurrent themes identified by experts across evaluation variablesClick here to view Figure |
This heatmap matrix displays the distribution of recurrent themes identified through thematic analysis of expert responses (themes with ≥ 3 occurrences are highlighted). It emphasizes operational priorities such as adaptation to local contexts, interprofessional coordination tools, and psychosocial support mechanisms.
The following table presents a summary of the recommendations made by the experts for the variables that obtained an average score of less than 4.
Table 6: Summary of expert recommendations for improving the TPE-GD Workbook by variable
| Variable | Recurring themes | N | % (variable) | Total themes n (%) | Key recommendations |
| RSB 4 : Clarity and structure | Dense and voluminous content | 4 | 57.1 | 7 (8) | Simplify and streamline content for ease of use by non-specialist educators |
| Lack of synthesis tools (summaries, practical sheets) | 3 | 42.9 | Add summaries at the end of sections; include practical tools (summary sheets, decision-making algorithms) | ||
| MPP 2 : GD-specific methodology | Time constraints poorly addressed | 6 | 54.5 | 11 (13) | Adapt content to GD follow-up time constraints |
| Limited integration of pregnancy-specific content | 5 | 45.5 | Integrate pregnancy-related aspects more thoroughly in educational materials | ||
| MPP 4: Personalization and interprofessional collaboration | No patient education booklet | 1 | 8.3 | 12 (14) | Develop educational booklets for patients |
| Insufficient definition of roles and interprofessional consultation | 5 | 41.7 | Define the roles of stakeholders and strengthen interprofessional consultation. | ||
| Lack of coordination and training tools for implementation | 6 | 50.0 | Create coordination tools between teams and organize training to facilitate the implementation of the workbook. | ||
| EDO 1 : Identifying priorities | Insufficient exploration of the patient’s needs | 2 | 50.0 | 4 (5) | Use open questions to better identify needs. |
| Lack of initial diagnostic tool completed by the patient | 2 | 50.0 | Provide initial diagnostic grids completed by patients | ||
| EDO 3 : Learning barriers | Incomplete assessment of psychosocial barriers | 3 | 75.0 | 4 (5) | Integrate the assessment of educational level, social support, dietary beliefs and psychosocial barriers. |
| Lack of a specific module on psychological and socio-economic barriers | 1 | 25.0 | Add a specific module on psychological and socio-economic obstacles. | ||
| EDO 4 : Learning objectives | Insufficient negotiation tools for objectives | 4 | 80.0 | 5 (6) | Improve goal negotiation tools to promote active patient participation. |
| Lack of simplified guides for patients | 1 | 20.0 | Develop simplified guides to support patients. | ||
| PIE 1 : Clinical constraints | Lack of digital support and dedicated multidisciplinary units | 2 | 22.2 | 9 (10) | Digitize the workbook and create dedicated multidisciplinary units. |
| Complexity of protocols and limited adaptation to context | 2 | 22.2 | Simplify protocols and promote adaptation to the GD context | ||
| Interest of group sessions | 3 | 33.3 | Encourage group session format to optimize time. | ||
| Limited integration into routine consultations | 2 | 22.2 | Integrate the program into standard consultations to limit organizational impact. | ||
|
APF 1 : Psychological aspects |
Limited content on stress/emotional support | 4 | 57.1 | 7 (8) | Develop a specific chapter on stress management and emotional support. |
| Need for a psychologist in the team | 2 | 28.6 | Systematically integrate a psychologist trained in TPE. | ||
| Inadequate emotional support during diagnosis | 1 | 14.3 | Implement a structured emotional support protocol for diagnosis disclosure | ||
| APF 2 : Socioeconomic and cultural adaptation | Inadequate adaptation to local contexts | 7 | 77.8 | 9 (10) | Adjust materials to local economic/cultural realities (e.g., rural settings) |
| Lack of multilingual educational tools | 1 | 11.1 | Provide multilingual resources for better accessibility | ||
| Limited socioeconomic profiling | 1 | 11.1 | Categorize socioeconomic profiles to offer tailored adaptations | ||
| APF 3 : Family involvement | Insufficiently defined framework for family involvement | 3 | 37.5 | 8 (9) | Clarify when family involvement is beneficial |
| Lack of educational support for those around them | 4 | 50.0 | Create specific resources for the patient’s support system | ||
| Patient preferences not always respected | 1 | 12.5 | Respect patient decisions on family inclusion | ||
| APF 4 : Self-confidence | Lack of strategies to strengthen self-esteem and acceptance of the disease | 5 | 55.6 | 9 (10) | Include techniques to improve self-esteem and disease acceptance |
| Lack of practical exercises or group activities | 2 | 22.2 | Develop hands-on activities and group sessions | ||
| Insufficient recognition of skills acquisition | 2 | 22.2 | Offer opportunities for patients to apply knowledge and gain confidence |
Qualitative analysis identified 29 recurring themes, with a total of 85 coded occurrences. These themes mainly concern variables with mean scores below 4 and indicate areas requiring improvement, as detailed in the methodology section.
The expert suggestions were distributed as follows:
Axis 5 – Adaptation and Psychosocial-Economic Factors: 33 instances (38%) across the four variables APF 1 to APF 4;
Axis 2 – Methodology and Program Personalization: 23 instances (27%) across two variables: MPP 2 and MPP 4;
Axis 3 – Educational Diagnosis and Objectives: 13 instances (16%) across three variables: EDO 1, EDO 2, and EDO 3;
Axis 4 – Program Implementation and Evaluation: 9 instances (10%) for one variable: PIE 1;
Axis 1 – Relevance and Scientific Basis: 7 instances (8%) for one variable: RSB 4.
Discussion
This study confirms the suitability of the TPE-GD workbook as an educational tool for women with GD, based on evaluation by a panel of 35 multidisciplinary experts. The average score (4.09/5) indicates overall acceptability between “satisfactory” and “very satisfactory.” However, adjustments are necessary for items rated below 4, particularly concerning content clarity, methodological adaptation, identification of learning barriers, and integration of psychosocial factors. These needs were reinforced by the qualitative analysis, identifying 29 areas for improvement, totaling 85 thematic occurrences.
Regarding scientific relevance, the workbook demonstrates strong alignment with international guidelines (WHO, HAS). Sections addressing nutrition, physical activity, and glycemic monitoring were particularly well-received, consistent with previous findings highlighting the positive impact of clear, validated information on GD self-management.29 Such alignment supports the credibility and transferability of the tool to settings beyond Morocco, provided local contextualization is maintained. Nevertheless, disciplinary differences emerged: endocrinologists cited excessive technical detail, whereas dietitians, psychologists, and health managers found the content accessible to non-specialist users.
This divergence does not reflect a fundamental flaw but rather highlights a recognized pedagogical challenge: balancing scientific rigor with usability for frontline educators.30 This challenge is particularly relevant for Arabic-speaking patients, as studies have shown they achieve better comprehension when counseling is delivered in their native language.31 Thus, beyond linguistic translation, adapting scientific content to varying health literacy levels is crucial.30,31 A practical approach could involve developing multi-level formats, such as simplified explanations for patients alongside detailed annexes for clinicians. This strategy would enhance comprehension and foster interprofessional collaboration by enabling health professionals to use the workbook effectively within their respective scopes of practice.
Statistical analysis supported these observations, revealing significant specialty differences in the clarity and structure of content (p = 0.032). Endocrinologists assigned notably lower scores (p < 0.05), potentially reflecting perceived excessive density and limited suitability for Moroccan clinical contexts. Furthermore, experts trained in TPE evaluated this dimension more critically (p = 0.039), likely due to heightened awareness of pedagogical best practices and readability. Professionals with more than 15 years of experience also highlighted the need to update the scientific content (p = 0.038). Experts recommended enhancing clinical usability by adding summaries at the end of sections, simplifying technical content, and incorporating concise reference sheets.
The workbook’s methodology aligns with TPE standards, following the core stages of educational diagnosis, goal-setting, implementation, and evaluation. Nonetheless, experts highlighted insufficient individualization, particularly noted by psychologists, nutritionists, and gynecologists. This underscores the need for better tailoring materials to patient profiles, accounting for their motivations, socioeconomic backgrounds, and personal perceptions. A standardized approach may inadequately address specific patient needs, reinforcing calls for personalized educational resources to enhance patient engagement32. Future iterations might benefit from a modular design, allowing professionals greater flexibility in selecting content tailored to individual patient characteristics or readiness.
Statistically, specialty significantly influenced methodological evaluation (p = 0.037), while professional experience affected perceptions of adaptability (p = 0.020). Experts trained in TPE provided more critical assessments (p = 0.032), potentially due to heightened expectations regarding flexibility. Proposed improvements included summary sheets, decision-making algorithms tailored to patient profiles, and greater patient involvement in content development, consistent with literature advocating co-constructed educational materials.33
Regarding educational diagnostic tools, experts generally found them appropriate, although the identification of learning barriers was rated lower. Biomedical dimensions were well covered, yet psychosocial aspects were underrepresented, and the current format might limit patient expression of challenges or perceptions. While no significant differences by specialty, experience, or training were found, experts recommended enriching diagnostic tools with open-ended questions to better identify patient expectations and barriers. Including dedicated sections on learning obstacles with self-assessment features (quizzes, reflective boxes) could improve individual tailoring32, aligning with recent recommendations for more inclusive and interactive patient engagement methods. Additionally, incorporating content addressing cultural and contextual aspects, such as healthcare access, food norms, or religious beliefs, could significantly enhance contextual relevance30, particularly in multicultural and multilingual settings.
Regarding program implementation, clinical constraints posed notable challenges, primarily related to integrating the program into routine care amidst overloaded consultations and limited TPE-trained professionals. This finding aligns with literature identifying time constraints as a significant barrier to TPE delivery.34 Further issues included the absence of dedicated facilities, limited institutional recognition, and inconsistent patient attendance. To mitigate these constraints, experts suggested digital solutions (e.g., mobile applications, interactive platforms) facilitating patient self-management. Recent evidence supports the effectiveness of digital technologies in managing gestational diabetes, often surpassing traditional follow-up methods.35 Additional recommendations included appointing dedicated TPE coordinators, training multidisciplinary teams, organizing group education sessions, and employing simplified monitoring tools, such as brief questionnaires, to reduce professional workload.
The psychosocial and economic adaptation dimension received lower ratings, reflecting the need for enhanced adaptation to real-life contexts experienced by women with gestational diabetes. Disparities in language, culture, and socioeconomic status significantly influence the comprehension and application of educational recommendations. Studies confirm that Arabic-speaking patients achieve better comprehension when counseling is delivered in their native language, and lower health literacy is linked to poorer self-management outcomes.31 Additionally, family involvement remains crucial for adherence to medical recommendations.36
Experts thus recommended including dedicated sections targeting family members, clearly outlining their roles in dietary management and glycemic monitoring. The involvement of spouses or relatives can notably strengthen patient adherence and emotional support.37 Furthermore, adapting educational content to cultural and religious practices (e.g., Ramadan fasting, traditional dietary norms) is considered essential for maintaining relevance and acceptability. Most current digital applications lack this cultural specificity,30 reinforcing recent literature advocating culturally tailored educational tools for GD management.38
These findings align with evidence from low- and middle-income countries (LMICs), particularly South Asia, where culturally tailored modules demonstrated effectiveness. The DESI GDM project in India, a personalized nutrition intervention, showed high acceptability and improved glycemic control.39 Similarly, in high-income settings, tailored interventions such as a Spanish-language program for Hispanic women in the United States improved self-monitoring behaviors and glycemic outcomes.40
Addressing emotional responses, particularly stress triggered by diagnosis, emerged as a critical theme. GD diagnoses often generate significant anxiety;41 thus, integrating stress-management resources, patient testimonials, and psychoeducational elements could enhance patient engagement. Structured interventions addressing emotional aspects have effectively reduced GD-related stress and enhanced self-efficacy.42 Experts also noted economic constraints as potential barriers, particularly for vulnerable populations, advocating flexible educational formats, such as teleconsultations, to increase accessibility.
From a statistical perspective, experts trained in TPE consistently provided significantly lower ratings regarding psychosocial and cultural dimensions (p = 0.031 and p = 0.002, respectively), reflecting heightened awareness of these critical dimensions. No significant differences were observed by specialty or experience, indicating broad agreement on their importance. Recommended improvements included stronger emphasis on emotional experiences, translation into Moroccan Arabic, and the development of modular, accessible delivery formats.
Implications for practice
The validated TPE-GD workbook constitutes an operational tool ready for use in diabetes clinics and maternity units in Morocco. It supports standardized TPE delivery and improves patient adherence by offering culturally and linguistically adapted content tailored to Arabic-speaking populations.
To facilitate implementation, the following strategic actions are recommended:
Integration into national maternal health programs under Ministry of Health coordination.
Pilot deployment in selected public and private facilities to assess feasibility.
Development of digital formats (e.g., mobile apps, web platforms) for autonomous access.
Targeted training of healthcare providers in educational methods and workbook use.
Institutional support to ensure resource allocation and systemic integration.
These recommendations reflect expert insights and address real-world constraints such as limited time, staff shortages, and irregular patient follow-up. The workbook may also serve as a model for Arab countries aiming to institutionalize TPE in maternal care.
Theoretical contribution
This study offers the first validated GD-specific educational tool adapted to Moroccan and Arab contexts. It fills a gap in the literature by combining pedagogical structure with cultural sensitivity. The use of a multidisciplinary expert panel and mixed methods enhances the robustness and replicability of the validation process.
Unlike other GD tools in the MENA region, often lacking local relevance or formal validation, the TPE-GD workbook demonstrates methodological rigor and cultural alignment. Scaling to other countries would require adjustments in language, culture, and health systems. The findings contribute to debates on TPE in low-resource settings, emphasizing the value of co-designed, context-sensitive tools for improving maternal health outcomes.
Limitations of the study
Several limitations should be noted. First, purposive sampling may have reduced the diversity of expert views, as most participants were based in urban or institutional settings, limiting generalizability to rural or underserved contexts.
Second, the evaluation occurred in a single round, without iterative methods like Delphi, limiting the refinement of expert feedback. A second round is planned to enhance consensus and validation rigor.
Although internal consistency was acceptable overall (α = 0.82), some subscales had moderate reliability (α = 0.52–0.63). In particular, the low consistency of the “Educational Diagnosis” axis suggests that items like “identify priorities”, “ease of use”, and “identify barriers” may represent distinct constructs. Future revisions should address this by refining item grouping and formulation.43
Moreover, this validation was based solely on expert assessment. The absence of patient involvement constitutes a major limitation, as it prevents the evaluation of clarity, acceptability, and real-world applicability from the end-user perspective. Future phases will need to include patient feedback to ensure that the tool is comprehensible, culturally appropriate, and effective in improving self-management outcomes.
Conclusion
Based on an evaluation by 35 experts, this study confirms the relevance and content validity of the TPE workbook for GD. The tool was considered useful, well-aligned with international standards, and potentially transferable across Arabic-speaking contexts, provided that local adaptation is ensured.
However, its effective implementation will require targeted improvements, particularly in terms of personalization, psychosocial integration, and simplification to adapt to clinical constraints such as time pressure and limited human resources. Recommendations include the development of summary sheets, modular content, and digital adaptations to enhance flexibility and accessibility.
This work provides a validated foundation for the next phase of co-construction with patients, aiming to develop the first TPE tool for gestational diabetes that is both pedagogically sound and fully adapted to the Moroccan sociocultural context. This next stage should include (1) structured pilot testing with patients to assess clarity and usability, (2) evaluation of clinical and behavioral outcomes, and (3) digital dissemination to support broader access and equity in therapeutic education.
Acknowledgment
The authors would like to thank the Abulcasis International University of Health Sciences for supporting this research work. Special thanks are also extended to the Faculty of Medicine and Pharmacy, Mohammed V University in Rabat, for their institutional support. We are also grateful to the health professionals and experts who participated in the evaluation process of the therapeutic education workbook and provided valuable insights.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
The study was conducted in accordance with the ethical principles applicable to non-interventional research. All participants were informed in writing about the study’s objectives and assurances of confidentiality. Free and informed consent was obtained from each expert. In accordance with Moroccan Law No. 28.13 and article 2 of the National Ethics Guidelines for Non-Interventional Studies, formal ethical approval was not required. Nonetheless, good research practices were strictly followed throughout the process, including respect for anonymity, data protection, and voluntary participation..
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Authors’ Contributions
- Abdelhaq Barbach: Conceptualization, Methodology, Data Analysis, Writing – Original Draft
- Youssef Ikken: Conceptualization, Methodology, Writing – Review & Editing
- Ouiam Dahmane: Data Analysis, Review
- Yahya Charrah: Critical Review
- Anas Ansari Chenguiti: Critical Review, Validation
- Rachid Alami: Critical Review, Validation
- Amina Barkat: Supervision, Project Administration, Writing – Final Approval
References
- World Health Organization. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. Geneva: World Health Organization; 2013. Report No.: WHO/NMH/MND/13.2.
- Agarwal MM. Gestational Diabetes in the Arab Gulf Countries: Sitting on a Land-Mine. Int J Environ Res Public Health. 2020;17(24):9270.
CrossRef - Bashir MM, Ahmed LA, Elbarazi I, et al. Incidence of gestational diabetes mellitus in the United Arab Emirates; comparison of six diagnostic criteria: The Mutaba’ah Study. Front Endocrinol (Lausanne). 2022;13:1069477.
CrossRef - Lende M, Rijhsinghani A. Gestational Diabetes: Overview with Emphasis on Medical Management. Int J Environ Res Public Health. 2020;17(24):9573.
CrossRef - Berger H, Gagnon R, Sermer M. Directive clinique N° 393 – Le diabète pendant la grossesse. J Obstet Gynaecol Can. 2019;41(12):1826-1839.e1.
CrossRef - Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational Diabetes Mellitus: Mechanisms, Treatment, and Complications. Trends Endocrinol Metab. 2018;29(11):743-754.
CrossRef - Kapur K, Kapur A, Hod M. Nutrition management of gestational diabetes mellitus. Ann Nutr Metab. 2021;76 (Suppl. 3): 17–29.
CrossRef - Han S, Middleton P, Shepherd E, Van Ryswyk E, Crowther CA. Different types of dietary advice for women with gestational diabetes mellitus. Cochrane Database Syst Rev. 2017;2(2):CD009275.
CrossRef - World Health Organization. Therapeutic Patient Education: Continuing Education Programmes for Health Care Providers in the Prevention of Chronic Diseases. Geneva, Switzerland: World Health Organization; 1998.
- Correia JC, Waqas A, Aujoulat I, et al. Evolution of Therapeutic Patient Education: A Systematic Scoping Review and Scientometric Analysis. Int J Environ Res Public Health. 2022;19(10):6128.
CrossRef - Al-Khamees N. Diabetes prevention challenges in Arabic region: A call to action addressing the cultural context and eHealth. Curr Res Diabetes Obes J. 2016;1(5):1-4.
CrossRef - World Health Organization. Framework for Action on Diabetes Prevention and Control in the WHO Eastern Mediterranean Region. Cairo, Egypt: WHO Regional Office for the Eastern Mediterranean; 2021.
- World Health Organization. Therapeutic Patient Education: An Introductory Guide. Copenhagen, Denmark: WHO Regional Office for Europe; 2023.
- Doubi S, El Ouahabi H, Dakkar O, Ajdi F. Evaluation of a therapeutic education program in diabetic patients in a Moroccan university hospital: preliminary results of a pilot survey. Pan Afr Med J. 2014;18:258.
CrossRef - Rhattat F, Yassine N, Zaghba N. Mise en place d’un programme d’éducation thérapeutique du patient asthmatique au service de pneumologie CHU Ibn Rochd de Casablanca. J Biomed Res Health Econ. 2020;(2):1-6.
- Bougadoum M, Ait Batahar S, Amro L. Impact d’une intervention éducative de l’asthmatique sur la qualité de vie, l’observance thérapeutique et le contrôle de la maladie. Rev Mal Respir Actual. 2022;14(1):80.
CrossRef - Bentaleb I, Rostom S, Elbinoune I, Elhassani Sbai S, Amine B, Bahiri R. Evaluation of a therapeutic education program regarding the safety of biotherapies in patients with rheumatoid arthritis: Preliminary results at M3 of a randomized study. Rev Rhum. 2021;88(Suppl 1):A171.
CrossRef - Elghazouani F, Barrimi M, Aarab C, Rammouz I, Aalouane R. Mise en place d’un programme psychoéducatif pour les troubles bipolaires adapté au contexte marocain. L’Information Psychiatrique. 2017;93(3):217-221.
- Iguenane J, Marchand C, Bodelot D, et al. Implantation de programmes d’éducation thérapeutique de patients vivant avec le VIH dans quatre pays à ressources limitées. Approche évaluative. Sante Publique. 2007;19(4):323-333.
CrossRef - Khachani I. Mise en œuvre et évaluation d’un programme d’éducation thérapeutique pour patients VIH positifs suivis au CHU Ibn Sina de Rabat [thesis]. Rabat: Université Mohammed V – Souissi; 2008. Available from: http://ao.um5.ac.ma/xmlui/handle/123456789/1334
- Ministère de la Santé du Maroc. Stratégie nationale multisectorielle de prévention et de contrôle des maladies non transmissibles 2019–2029. Rabat: Ministère de la Santé; 2019. Available from: https://www.sante.gov.ma/Documents/2019/02/Plan%20Strate%CC%81gique.pdf
- Druye AA, Owusu G, Yeboa NK, et al. Self-management interventions for gestational diabetes in Africa: a scoping review. BMC Pregnancy Childbirth. 2024;24:549.
CrossRef - Al Hashmi I, Al Yazidi B, Al Omari O. Translation and psychometric validation of the Arabic Gestational Diabetes Management Self-Efficacy Scale (GDMSES). J Healthc Qual Res. 2022;37(4):231–238.
CrossRef - Chahed S, Lassouad L, Dardouri M, Mtiraoui A, Maaroufi A, Khairi H. Impact of a tailored-care education programme on maternal and neonatal outcomes in pregnant women with gestational diabetes: A randomized controlled trial. Pan Afr Med J. 2022;43:128.
CrossRef - Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11(2):49–54.
CrossRef - Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc Sci Med. 2022;292:114523.
CrossRef - Urrutia Egaña M, Barrios Araya S, Gutiérrez Núñez M, Mayorga Camus M. Métodos óptimos para determinar validez de contenido. Educ Med Super. 2014;28(3):547–558.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
CrossRef - Staynova RA, Gueorguiev SR, Petkova-Gueorguieva ES, et al. Written Health Education Materials for Women with Gestational Diabetes Mellitus – Evaluation of Usefulness and Patients’ Satisfaction. Folia Med (Plovdiv). 2019;61(1):127-133.
CrossRef - Birati Y, Yefet E, Perlitz Y, Shehadeh N, Spitzer S. Cultural and digital health literacy appropriateness of app- and web-based systems designed for pregnant women with gestational diabetes mellitus: Scoping review. J Med Internet Res. 2022;24(10):e37844.
CrossRef - Althubyani AN, Gupta S, Tang CY, et al. Barriers and enablers of diabetes self-management strategies among Arabic-speaking immigrants living with type 2 diabetes in high-income Western countries: A systematic review. J Immigr Minor Health. 2024;26(4):761–774.
CrossRef - Davis J, Fischl AH, Beck J, et al. 2022 National Standards for Diabetes Self-Management Education and Support. Sci Diabetes Self Manag Care. 2022;48(1):44-59.
CrossRef - Armstrong MJ, Mullins CD, Gronseth GS, Gagliardi AR. Recommendations for patient engagement in guideline development panels: A qualitative focus group study of guideline-naïve patients. PLoS One. 2017;12(3):e0174329.
CrossRef - Hafez G, Aarnio E, Mucherino S, et al. Barriers and Unmet Educational Needs Regarding Implementation of Medication Adherence Management Across Europe: Insights from COST Action ENABLE. J Gen Intern Med. 2024;39(15):2917-2926.
CrossRef - Smyth S, Curtin E, Tully E, Molphy Z, Breathnach F. Smartphone apps for surveillance of gestational diabetes: Scoping review. JMIR Diabetes. 2022;7(4):e38910.
CrossRef - Al Hashmi I. Gestational diabetes and determinants of adherence to healthy behaviors. Minerva Obstet Gynecol. 2022;74(2):146–154.
CrossRef - Abdollahian M, Dorri S, Haghani H, Ashghali Farahani M. The effect of spouse participation in gestational diabetes care on pregnant women’s perceived social support. J Nurs Midwifery Sci. 2023;10(1):e132630.
CrossRef - Jones C, Cui Y, Jeminiwa R, Bajracharya E, Chang K, Ma T. Personalized and Culturally Tailored Features of Mobile Apps for Gestational Diabetes Mellitus and Their Impact on Patient Self-Management: Scoping Review. JMIR Diabetes. 2024;9:e58327.
CrossRef - Stennett RN, Adamo KB, Anand SS, et al. A culturally tailored personaliseD nutrition intErvention in South ASIan women at risk of Gestational Diabetes Mellitus (DESI-GDM): a randomised controlled trial protocol. BMJ Open. 2023;13(5):e072353.
CrossRef - Ferrara A, Hedderson MM, Brown SD, et al. A telehealth lifestyle intervention to reduce excess gestational weight gain in pregnant women with overweight or obesity (GLOW): A randomised, parallel group, controlled trial. Lancet Diabetes Endocrinol. 2020;8(6):490–500.
CrossRef - Grinberg K, Yisaschar-Mekuzas Y. Assessing Mental Health Conditions in Women with Gestational Diabetes Compared to Healthy Pregnant Women. Healthcare. 2024; 12(14):1438.
CrossRef - Alshammari M, Lee RLT, Stubbs M, Chan SW. Effectiveness of psychoeducation interventions for pregnant women with gestational diabetes mellitus: An integrative review. BMC Public Health. 2024;24(1):2929.
CrossRef - Tavakol M, Dennick R. Understanding Cronbach’s alpha. Int J Med Educ. 2011;2:53–55.
CrossRef
Abbreviations List
TPE : Therapeutic Patient Education
GD : Gestational Diabetes
WHO : World Health Organization
T2D : Type 2 Diabetes
HAS : French National Authority for Health (Haute Autorité de Santé)
LMICs : Low- and Middle-Income Countries
DELM : Directorate of Epidemiology and Disease Control
CHU : University Hospital Center (Centre Hospitalier Universitaire)
HIV : Human Immunodeficiency Virus

