
Manuscript accepted on :24-06-2025
Published online on: 30-06-2025
Plagiarism Check: Yes
Reviewed by: Dr. Gowri Burle and Dr. Soujania Singh
Second Review by: Dr. Mohammed Ahmed
Final Approval by: Dr. Jihan Seid Hussein
Ana Luisa Robles-Piedras1* , Erick Salomón Bautista-Sánchez1, Urias Bautista-Sánchez1, Elena Guadalupe Olvera-Hernández1, Alejandro Chehue-Romero1 and José Roberto Medécigo-Hernández1,2
, Erick Salomón Bautista-Sánchez1, Urias Bautista-Sánchez1, Elena Guadalupe Olvera-Hernández1, Alejandro Chehue-Romero1 and José Roberto Medécigo-Hernández1,2
1Department of Pharmacy, Autonomous University of the State of Hidalgo, San Agustín Tlaxiaca, Hidalgo, México
2 Internal Medicine Department, Hospital General ISSSTE, "Dra. Columba Rivera Osorio”, Pachuca de Soto, Hidalgo, México
Corresponding Author E-mail: roblesa@uaeh.edu.mx
DOI : https://dx.doi.org/10.13005/bpj/3204
Abstract
The appropriate use of medications is essential to ensure patient safety and improve healthcare outcomes. This study aimed to analyze prescribing and medication consumption patterns in the internal medicine department of a second-level hospital in Mexico. An observational, retrospective study was conducted in hospitalized patients between June and November 2023. Demographic data, medical conditions, and prescribed medications were collected, and the World Health Organization’s Defined Daily Dose (DDD) methodology was applied to assess antibiotic consumption. A total of 104 patients were included, with a predominance of women (59.6%) and a mean age of 67.8 years. The average number of medications prescribed per patient was 7.7, reflecting a high level of polypharmacy. The most frequent conditions were diabetes mellitus (18.5%), arterial hypertension (16.7%), and chronic kidney disease (12.3%). The most frequently used medication groups were analgesics, anesthetics, anti-inflammatory agents, and antibiotics (14.5% each). Ceftriaxone was the most prescribed antibiotic, with a DDD of 84.0, highlighting a potential overuse. The findings reflect the high burden of chronic diseases, frequent use of broad-spectrum antibiotics, and the need for strategies to optimize hospital pharmacotherapy. It is concluded that it is essential to strengthen rational drug use programs, implement safe prescribing protocols, and promote the inclusion of clinical pharmacists to improve patient safety and the quality of hospital medical care.
Keywords
Antibiotic; Defined Daily Dose; Internal medicine; Pharmacists; Pharmacotherapy
Download this article as:| Copy the following to cite this article: Piedras A. L. R, Sánchez E. S. B, Sánchez U. B, Hernández E. G. O, Romero A. C. Hernández J. R. M. Prescription and Drug Consumption Patterns in internal medicine: A Study in a Secondary Level Hospital. Biomed Pharmacol J 2025;18(2). |
| Copy the following to cite this URL: Piedras A. L. R, Sánchez E. S. B, Sánchez U. B, Hernández E. G. O, Romero A. C. Hernández J. R. M. Prescription and Drug Consumption Patterns in internal medicine: A Study in a Secondary Level Hospital. Biomed Pharmacol J 2025;18(2). Available from: https://bit.ly/3I4GHEo |
Introduction
The appropriate use of medications is fundamental for enhancing patient care and ensuring efficiency within healthcare systems. This is especially true in hospital settings, where patients often present with complex conditions demanding meticulous and personalized attention.1 The internal medicine department, in particular, faces significant challenges in medication management. It typically cares for patients with multiple, often chronic and highly complex, pathologies that necessitate combined and prolonged pharmacological treatments. This reality introduces considerable challenges in selecting, dosing, and administering medications effectively. Suboptimal medication use can elevate patient risks, leading to adverse effects, unwanted drug interactions, and even serious adverse events that compromise patient safety and therapeutic success.
In internal medicine, the simultaneous prescription of multiple medications is common, increasing the risk of polypharmacy, defined as the concurrent use of five or more drugs. This phenomenon is prevalent in patients with chronic diseases or multimorbidity, characteristic of this specialty. While polypharmacy may be necessary to manage various co-existing pathologies, it can also lead to significant issues like pharmacological interactions, increased adverse effects, reduced treatment adherence, and administration errors.2 These issues carry not only clinical repercussions but also economic ones, potentially escalating healthcare costs due to the need for additional treatments, extended hospitalizations, or new medical consultations.3-4
Drug Utilization Studies (DUS) are crucial tools for evaluating and improving drug use in various clinical contexts. These studies provide a comprehensive overview of medication prescription, distribution, consumption, and administration patterns in specific populations, aiding in problem identification and the implementation of corrective strategies. DUS are invaluable for understanding how medications are used, providing data to enhance treatment safety, mitigate associated risks, and promote more efficient management of pharmacological resources.5 Furthermore, they are essential for monitoring the impact of pharmaceutical interventions aimed at improving adherence to clinical guidelines and prescribing safety regulations.6-7
The relevance of DUS is amplified in areas like internal edicine, which handles a broad spectrum of complex and chronic diseases frequently requiring prolonged and multidisciplinary pharmacological treatments. The diverse range of medications needed for these pathologies, coupled with common comorbidities and the necessity for personalized treatments, increases the likelihood of errors and the persistence of suboptimal practices in medication use. This underscores the importance of comprehensive studies that identify current medication use patterns and areas for improvement in pharmacological care.8
Findings from DUS in internal medicine can illuminate critical aspects of clinical practice. For instance, they can reveal trends in medication selection, such as over- or under-use of certain drugs, or the preference for more expensive or less effective options over safer, more affordable alternatives. These studies also provide information on average treatment durations compared to evidence-based recommendations. Another vital aspect DUS can address is the identification of potentially dangerous pharmacological interactions, particularly in polymedicated patients, which might otherwise go unnoticed in daily hospital routines.9-10
Moreover, the implementation of DUS can serve as a foundation for designing specific pharmaceutical interventions to address deficiencies in medication management. These interventions can range from training medical personnel to identify and manage polypharmacy properly, to creating safety protocols for prescribing high-risk medications and establishing alert systems for serious drug interactions. Ultimately, the objective of DUS is to contribute to the continuous improvement of healthcare quality, promoting clinical practices that safeguard patient safety and well-being.
This study was conducted in the internal medicine department of a secondary-level hospital in Mexico. Its aim was to evaluate medication prescription and consumption patterns and to identify potential areas for improvement in clinical practice. Secondary-level hospitals play a critical role in the health system by managing a wide range of pathologies that require comprehensive and coordinated clinical management, especially concerning medication use. Therefore, this study not only describes the current medication use situation in a specific context but also offers practical recommendations applicable to similar institutions facing comparable challenges in medication management.11 The findings are intended to benefit healthcare professionals at the study hospital and other secondary-level care centers.
Materials and Methods
Study Design and Setting. A retrospective, observational study was conducted in the internal medicine Department of the ISSSTE-Pachuca General Hospital, a secondary-level healthcare facility in Mexico. The study period encompassed hospital admissions from June to November 2023. The study population included adult patients aged 18 to 85 years who were admitted to the internal medicine service during the established period. Sociodemographic data, including age and sex, were extracted from clinical records to characterize the population and identify relevant demographic patterns. Data were collected from patients’ medical records, focusing on two primary domains: (1) demographic characteristics and (2) pharmacological data.12 The latter included the total number and type of medications prescribed per patient, the percentage distribution of each therapeutic class, and the consumption rate of complementary medications. For antibiotics, consumption was standardized using the Defined Daily Dose (DDD) methodology, as recommended by the World Health Organization (WHO).13 Descriptive statistical analyses were performed using Microsoft Excel®. Categorical variables were summarized as frequencies and percentages, while continuous variables were expressed as mean values with standard deviations (SD); this approach allowed for a comprehensive description of prescription patterns and medication consumption within the study population. The study was conducted in accordance with ethical standards for research involving human subjects. Institutional ethics committee approval was obtained prior to data collection, and all applicable national and international ethical regulations were observed. Confidentiality and data privacy were rigorously maintained throughout the study process.
Results
Table 1 shows the demographic characteristics and number of medications prescribed per patient involved in the study. A total of 104 patients were included, of which 59.6% were women and 40.4% were men. The average age of the patients was 67.8 years; likewise, the average number of medications per patient was 7.7, which reflects a high level of polypharmacy.
Table 1: Demographic characteristics and number of prescribed drugs per patient involved in the study.
| n = 104 | s.d.* | |
| Patients | ||
| Male | 42 | |
| Female | 62 | |
| Age (years) | 67.8 | 10.6 |
| Number of drugs prescribed | 7.74 | 4.04 |
*s.d. Standard deviation
Table 2 shows the main pathologies observed during the study period. The analysis of the frequency table reveals important findings related to the morbidity profile of the patients treated. First, there is a predominance of chronic-degenerative diseases, including Diabetes Mellitus (18.5%), Arterial Hypertension (16.7%), and chronic kidney disease (12.3%); in addition, a large number of metabolic and cardiovascular diseases are observed, which together represent 35.2% of the total, reflecting the current epidemiological profile of Mexico.
On the other hand, infectious processes also have significant relevance, with sepsis and infections representing 11% of cases, constituting an important cause of hospitalization. Likewise, acute neurological events, such as stroke, represent 9.7% of cases and are closely related to cardiovascular risk factors.
Table 2: Main pathologies observed during the study period.
| Category | Pathology | Frequency | Percentage (%) |
| Metabolic | Type 2 Diabetes Mellitus | 42 | 18.5 |
| Cardiovascular | Arterial Hypertension | 38 | 16.7 |
| Renal | Chronic Kidney Disease | 28 | 12.3 |
| Infectious | Sepsis/Infections | 25 | 11.0 |
| Neurological | Cerebrovascular Event | 22 | 9.7 |
| Respiratory | Pneumonia | 18 | 7.9 |
| Digestive | GI Pathologies | 15 | 6.6 |
| Traumatological | Cranioencephalic Trauma/Polytrauma | 12 | 5.3 |
| Autoimmune | Autoimmune Diseases | 8 | 3.5 |
| Oncological | Neoplasm | 6 | 2.6 |
| Others | Diverse | 13 | 5.7 |
| Total | 227 | 100 |
Figure 1 shows the distribution of medications used, according to their therapeutic indication. Medications for pain, anesthesia and inflammation, and antibiotics were the most used, each representing 14.5% of the total active ingredients administered. Cardiovascular drugs and those used for the central nervous system (CNS) represented 11.8% each, followed by respiratory and gastrointestinal medications (8.6% each). Of the 104 patients included in the study, 56 (53.8%) received some type of antibiotic. The distribution of antibiotics per patient showed that the majority of them (64%) received a single antibiotic, while 27% received two antibiotics, and a small percentage received three (5%) or up to four (4%) antibiotics. Regarding the DDD value of the antibiotics used (Figure 2), it was found that ceftriaxone was the most frequently prescribed antibiotic, with a total of 21 prescriptions and a calculated DDD of 84.0. This finding is consistent with its broad-spectrum profile and its usefulness in a variety of severe infections, both respiratory and systemic. Other frequently used antibiotics included clindamycin, with a DDD of 13.5, meropenem (19.5 DDD), and vancomycin (14.5 DDD); the use of these antibiotics is indicative of the management of complex and multi-resistant infections. On the other hand, the use of levofloxacin also stood out with a DDD of 25.0.
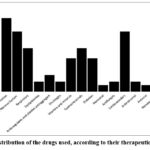 |
Figure 1: Distribution of the drugs used, according to their therapeutic indication.Click here to view Figure |
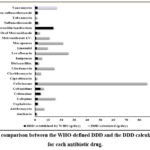 |
Figure 2: comparison between the WHO-defined DDD and the DDD calculated daily for each antibiotic drug.Click here to view Figure |
Discussion
The present drug utilization study (DUS), conducted in a second-level public hospital in Hidalgo, Mexico during a 5-month period, aimed to analyze the patterns of prescription and medication use in a hospital population. The sample consisted of 104 patients, of which 62 (59.6%) were women and 42 (40.4%) were men. This female predominance is a pattern that may be associated with the higher life expectancy of women and the prevalence of certain chronic conditions more common in this group. The average age of the patients was 67.8±10.6 years, indicating a predominantly elderly population. This age group is particularly susceptible to various chronic and acute diseases, which explains the need for therapeutic management that includes multiple medications.14 Likewise, in this study, an average use of 7.7 medications per patient was observed (Table 1), which reflects a considerable level of polypharmacy. This fact is relevant, as the use of multiple medications increases the risk of drug interactions, adverse effects, and problems with treatment adherence.
Regarding the analysis of the distribution of drugs by Therapeutic Category used during the study period, the sample revealed that medications for pain, anesthesia, and inflammation, along with antibiotics, were the most commonly employed groups (Figure 1), each representing 14.5% of the total active ingredients. This underscores the importance of these categories in the management of clinical conditions that predominate in a second-level hospital, where both acute and chronic pathology cases are treated. Cardiovascular drugs and those used for the central nervous system (CNS) also showed considerable use, each representing 11.8% of the total. The high frequency of prescription of these medications suggests the significant presence of chronic diseases such as hypertension, arrhythmias, heart failure, and neurological or psychiatric disorders. Respiratory and gastrointestinal medications, each representing 8.6% of the total, evidence the need for treatments for respiratory and digestive conditions, which are also common in this type of institution. Other therapeutic categories, such as medications for diabetes (6.6%) and vitamin and mineral supplements (6.6%), also had a notable presence. This is indicative of a comprehensive approach in the management of chronic diseases such as diabetes mellitus and the need to complement treatment with micronutrients, especially in elderly populations with potential nutritional deficits. The use of antibiotics is a critical part of clinical management in second-level hospitals. In this study, 53.8% of patients (n=104) received at least one antibiotic. Of these, 64% received a single antibiotic, while 27% were treated with two, and a smaller percentage (5% and 4%) received three or up to four antibiotics, respectively. This distribution reflects both the practice of monotherapy in less complex infections and the combination of antibiotics in more severe or resistant cases. Figure 2 illustrates the comparison between the WHO-defined DDD and the DDD calculated daily for each antibiotic drug. Ceftriaxone was the most frequently prescribed antibiotic, with a total of 21 prescriptions and a calculated DDD of 84.0; this finding is consistent with its broad-spectrum profile and its usefulness in a variety of severe infections, both respiratory and systemic. Other frequently used antibiotics included clindamycin, with a DDD of 13.5, meropenem (19.5 DDD), and vancomycin (14.5 DDD); the use of these antibiotics is indicative of the management of complex and multi-resistant infections. On the other hand, the use of levofloxacin also stood out with a DDD of 25.0, suggesting that this antibiotic was used in prolonged treatments or at high doses, probably in the management of serious infections such as pneumonia or complicated urinary tract infections.15 The presence of antibiotics such as imipenem and piperacillin/tazobactam underscores the need for robust therapeutic options for cases of resistant infections, an increasingly present challenge in second-level hospitals. The comparison of the calculated DDDs with those established by the WHO provides a perspective on the adequacy of the doses used in the hospital; for example, ceftriaxone presented a DDD much higher than the established one (84.0 versus 2), which may reflect both the need to treat serious infections as well as possible overprescription practices, and the same occurs with antibiotics such as levofloxacin and meropenem, which show high DDDs compared to WHO recommendations.16 Based on the analysis of antibiotic use, the risks and relevant considerations regarding the high use of broad-spectrum antibiotics and the polypharmacy observed in this study can be revisited, as significant challenges are presented. Polypharmacy (with an average of 7.7 medications per patient) is particularly concerning in elderly patients, given the increased risk of adverse reactions, interactions, and complications such as cognitive deterioration or frailty.17 In addition, the prescription of antibiotics at high DDDs is an important risk factor for the development of bacterial resistance, a growing public health problem that requires prudent management strategies.18-20
The main findings of the study highlight the predominance of chronic-degenerative diseases in the studied population. Among them, Diabetes Mellitus represents 18.5%, followed by Arterial Hypertension with 16.7% and Chronic Kidney Disease with 12.3%. These conditions are indicative of a high burden of non-communicable diseases in the hospital context. Likewise, a high burden of metabolic and cardiovascular diseases was observed, which together represent 35.2% of the total. This data clearly reflects the current epidemiological profile of Mexico, characterized by a transition towards a high incidence of diseases related to lifestyles and population aging. On the other hand, infectious processes, such as sepsis and other infections, constitute 11% of the cases attended, which, in this study period, positions them as an important cause of hospitalization. A relevant proportion of acute neurological events, such as cerebral vascular events, was also identified, representing 9.7% of the pathologies, and is closely linked to cardiovascular risk factors. The implications of these results obtained are very broad, they can be mentioned from the perspective of medical care, but, in addition, the need for multidisciplinary management to address the complexity of cases should be highlighted, as well as a high demand for hospital resources and the requirement of specialists in various areas.21 In Mexico, in the hospital setting, the figure of the integrated, recognized, and mainly accepted clinical pharmacist does not yet exist in health institutions, this is something that currently constitutes an important barrier to consider, hence the need to conduct this type of study.
Conclusion
The patient sample, composed predominantly of elderly adults with a female predominance, reflects a vulnerable population that requires a comprehensive and multidisciplinary approach to medical care. The average of 7.7 medications per patient evidences polypharmacy and underscores the need to monitor interactions and promote adherence to minimize risks. The frequent use of broad-spectrum antibiotics and the high calculated DDDs highlight the urgency of rational use policies to prevent bacterial resistance. The significant presence of cardiovascular, CNS, and medications for respiratory and gastrointestinal conditions shows the high burden of chronic and acute diseases in this population. This study shows that it is essential to strengthen educational programs on the rational use of medications, which would be significantly strengthened with the participation of professional hospital clinical pharmacists, as well as implementing guidelines and protocols that encourage the optimization of treatments and the reduction of unnecessary polypharmacy; likewise, the importance of continuous surveillance in the use of medications and the adoption of strategies to improve the quality and safety of treatment in highly complex patients is highlighted.
Acknowledgment
The authors would like to thank to Miss Michelle Guadarrama, for providing required support in the translation of the manuscript
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article
Ethics Statement
The study was conducted in accordance with ethical standards for research involving human subjects. Institutional ethics committee approval was obtained prior to data collection (Approval No. CEEI/001/2023), and all applicable national and international ethical regulations were observed. Confidentiality and data privacy were rigorously maintained throughout the study process.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not Applicable
Authors’ Contribution: The authors contributed to the study as follows:
- Ana Luisa Robles-Piedras: Conceptualization, Definition of Intellectual Content, Design, Literature Search, Data Analysis, Statistical Analysis, Manuscript Preparation, Manuscript Review.
- Urias Bautista-Sánchez: Conceptualization, Definition of Intellectual Content, Design, Data Acquisition, Data Analysis, Statistical Analysis, Manuscript Review.
- Erick Salomón Bautista-Sánchez: Design, Data Acquisition, Data Analysis, Manuscript Review.
- Elena Guadalupe Olvera-Hernández: Literature Search, Manuscript Review.
- Alejandro Chehue-Romero: Literature Search, Manuscript Review.
- José Roberto Medécigo-Hernández: Conceptualization, Data Acquisition, Manuscript Review.
References
- Obeid D, Karara A. Drug utilization and potential drug-drug interactions within an intensive care unit at a university tertiary care hospital in Egypt. Pharmacy (Basel). 2022;10(1):1-11.
CrossRef - Gnjidic D, Hilmer SN, Blyth FM, et al. Polypharmacy cutoff and outcomes: five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J Clin Epidemiol. 2012;65(9):989-995.
CrossRef - Athawale S, Kulkarni M. Drug utilization study in medicine intensive care unit in tertiary care hospital. Int J Basic Clin Pharmacol. 2019;8(12):2718-2724.
CrossRef - Bond CA, Raehl CL. Clinical pharmacy services, pharmacy staffing, and hospital mortality rates. Pharmacotherapy. 2007;27(4):481-493.
CrossRef - Leape LL, Cullen DJ, Clapp MD, et al. Pharmacist participation on physician rounds and adverse drug events in the intensive care unit. JAMA. 1999;282(3):267-270.
CrossRef - Lima MG, Álvares J, Guerra AA Jr, et al. Indicators related to the rational use of medicines and its associated factors. Rev Saude Publica. 2017;51(suppl 1):23s.
CrossRef - Raveh D, Muallem-Zilcha E, Greenberg A, et al. Prospective drug utilization evaluation of three broad-spectrum antimicrobials: cefepime, piperacillin-tazobactam and meropenem. QJM. 2006;99(6):397-406.
CrossRef - Khezrian M, McNeil CJ, Murray AD, Myint PK. An overview of prevalence, determinants and health outcomes of polypharmacy. Ther Adv Drug Saf. 2020;11:2042098620933741.
CrossRef - Krähenbühl-Melcher A, Schlienger R, Lampert M, et al. Drug-related problems in hospitals: a review of the recent literature. Drug Saf. 2007;30(5):379-407.
CrossRef - Egger SS, Drewe J, Schlienger RG. Potential drug-drug interactions in the medication of medical patients at hospital discharge. Eur J Clin Pharmacol. 2003;58(11):773-778.
CrossRef - Kumar R, Indira R, Rizvi A, et al. A study of prescribing pattern in the outpatient department of medicine of a tertiary care teaching hospital in North India. J Clin Diagn Res. 2013;7(1):154-157.
- Bertoldi AD, Barros AJD, Wagner A, et al. A descriptive review of the methodologies used in drug utilization research based on household surveys. Cad Saude Publica. 2008;24(suppl 4):S580-S588.
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2023. Oslo, Norway: WHO; 2022.
- Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57-65.
CrossRef - Gagliotti C, Ricchizzi E, Buttazzi R, Tumietto F, Resi D, Moro ML. Hospital statistics for antibiotics: defined versus prescribed daily dose. Infection. 2014;42(5):869-873.
CrossRef - Muller A, Monnet DL, Talon D, Hénon T, Bertrand X. Discrepancies between prescribed daily doses and WHO defined daily doses of antibacterials at a university hospital. Br J Clin Pharmacol. 2006;61(5):585-591.
CrossRef - Onder G, Petrovic M, Tangiisuran B, et al. Development and validation of a score to assess risk of adverse drug reactions among in-hospital patients 65 years or older: the GerontoNet ADR risk score. Arch Intern Med. 2010;170(13):1142-1148.
CrossRef - Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229-241.
CrossRef - Ventola CL. The antibiotic resistance crisis: part 1: causes and threats. P T. 2015;40(4):277-283.
- Spellberg B, Bartlett JG, Gilbert DN. The future of antibiotics and resistance. N Engl J Med. 2013;368(4):299-302.
CrossRef - Kaboli PJ, Hoth AB, McClimon BJ, et al. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166(9):955-964.
CrossRef

