A Systematic Review and Meta-Analysis of Kiwifruit’s Impact on Functional Constipation
 , Ervina Vashti1, Agustina Dwi Retno Nurcahyanti1, , 3 and Rungnapa Malasao4
, Ervina Vashti1, Agustina Dwi Retno Nurcahyanti1, , 3 and Rungnapa Malasao4 1Department of Pharmacy, School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Jakarta, Indonesia.
2Department of Clinical Pathology, Padjadjaran University/Hasan Sadikin General Hospital, Bandung, Indonesia.
3Department of Clinical Pathology, Maranatha Christian University, Bandung, Indonesia.
4Department of Community Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Corresponding Author E-mail: fonny.cokro@atmajaya.ac.id
DOI : http://dx.doi.org/10.13005/bpj/2891
Download this article as:
![]()
Introduction: Kiwifruit is rich in nutrients and fibers that benefit the digestive system. Despite various clinical investigations on the efficacy of kiwifruit for constipation, conflicting results are present. Therefore, the purpose of this meta-analysis was to evaluate the effectiveness of kiwifruit in treating functional constipation. Methods: The study’s main goal is to quantify the frequency of defecation. Randomized-controlled trials (RCTs) were explored from four databases, including Cochrane Library, ProQuest, Science Direct, and MEDLINE, with Google Scholar as an additional database for hand-searching purposes. The Risk of Bias 2 (RoB2) and Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tools were employed to evaluate the certainty of evidence. The meta-analysis was carried out using RevMan. Results: After critically appraising the individual articles, the study includes five randomized controlled trials (RCTs). The results indicated that defecation frequency improved considerably, with a p-value of 0.0008 and a weighted mean difference (WMD) of 0.07. However, the GRADE analysis showed low-quality evidence. Conclusions: Kiwifruit may be a secure and efficient treatment for people with functional constipation. However, further high-quality clinical investigations are needed to confirm these results.
KEYWORDS:Constipation; Defecation Frequency; Kiwifruit; Meta-Analysis; Systematic Review
Introduction
Functional constipation occurs when the waste disposal system does not function correctly without comorbidities and medication side effects. This type of constipation can be caused by slow food transit and obstruction in the gastrointestinal tract 1. According to a systematic review of patients with constipation from 1990 to 2020, the prevalence of functional constipation was 15.3% 2. Meanwhile, a study conducted in Japan with 5,155 participants reported that the incidence of functional constipation was 52.2% compared to other types of chronic constipation 3. Dietary adjustment and lifestyle modification can serve as effective preventive measures and alternatives to pharmacological medications, which may entail potential side effects like magnesium toxicity, cramping, and nutrient malabsorption4,5. By implementing these changes, individuals can help prevent the onset of this disorder and alleviate constipation without relying solely on medication5,6. Dietary fiber, categorized as a type of bulk laxative medication, is widely regarded as the safest treatment option when compared to other classes of laxatives4. As a result, it is highly recommended for effectively managing functional constipation. Fiber can enhance stool water retention, create gel-like substances to lubricate the stool, increase stool volume, and stimulate peristalsis, aiding in regular bowel movements 2. In addition to fiber, certain functional foods like psyllium and wheat bran can contribute to maintaining a healthy gut. It is noteworthy that multiple studies have consistently recommended whole green kiwifruit as an effective remedy for relieving constipation over an extended period of time7–10.
Kiwifruit belongs to the genus Actinidia and contains about 1.4 – 3 g of fiber per 100 g, with one-third soluble fiber and two-thirds insoluble fiber 7. The most common kiwifruit species are Actinidia deliciosa and Actinidia chinensis, known as green and gold kiwifruit, respectively. In addition to fiber, kiwifruit also contains vitamins, minerals, phytonutrients, and proteins, including actinidin, a natural proteolytic enzyme that helps in protein breakdown and digestion 7,11. Numerous randomized controlled trials (RCTs) showed that kiwifruit can enhance bowel movement frequency, with conflicting results 12–14. Therefore, this systematic review and meta-analysis was undertaken to provide an up-to-date study on the effectiveness of kiwifruit in
treating functional constipation symptoms. The scope of this research included kiwifruit species, namely Actinidia chinensis var. deliciosa, which consists of both green and gold kiwifruit.
Methods
Research Design
We prepared this meta-analysis using the Cochrane Handbook for Systematic Reviews of Interventions as a guideline.15. The results were reported according to the Preferred Reporting Items of Systematic Reviews and Meta-Analysis (PRISMA) statement.
Eligibility Criteria
Using the population, intervention, comparator, and outcome (PICO) approach, participants were chosen based on inclusion criteria. The inclusion criteria were healthy patients with functional constipation aged ≥ 18 years and no history of comorbidities. Meanwhile, the intervention criteria were kiwifruit in whole fruit or supplement form, non-combination, with the placebo or without therapy as the comparator. The primary outcome was bowel movement, with defecation frequency as the measured parameter. The secondary outcome included straining events, stool texture, and side effects of kiwifruit. This analysis focused on studies with both parallel and crossover RCT designs. Meanwhile, studies that did not comply with predetermined PICO criteria, including those involving patients taking laxatives or dietary fiber supplements, were excluded.
Literature Search
A research librarian guided the search protocol for this review. Literature searches were conducted until May 2023 on several databases, including Cochrane Central Register of Controlled Trials (CENTRAL), Medline, Science Direct, and ProQuest.For the Medline, CENTRAL, and Proquest databases, the exact MeSH terms used included: ((((((actinidia[MeSH Terms]) OR (Actinidia*[Title/Abstract])) OR (kiwifruit[Title/Abstract])) OR (kiwi[Title/Abstract])) OR (“Actinidia chinensis”[Title/Abstract])) OR (“Actinidia deliciosa”[Title/Abstract]) AND (randomizedcontrolledtrial[Filter])) AND ((constipation[MeSH Terms]) OR (constipation[Title/Abstract])). RCT was used as a filter for Medline, whereas books, book
chapters, conference papers and proceedings, dissertations and theses, articles, evidence-based healthcare, and other sources were used as filters for Proquest. Meanwhile, for the Science Direct database, we used exact keywords as follows: (Actinidia OR kiwifruit OR kiwi OR “Actinidia chinensis” OR “Actinidia deliciosa”) AND (constipation). For an additional search, we conducted a hand search via the Google Scholar database to find related articles.
Selection of Studies and Data Extraction
To assess the feasibility of research that satisfied the inclusion criteria, two researchers independently reviewed the title, abstract, and contents of full-text papers. The selected studies were tabulated based on PICO analysis. Related interventions were mentioned in detail regarding species and varieties of kiwi fruit, dosage form, dosage, and frequency of interventions. The flow from the literature searches to the study selection was carried out following the guidelines from the PRISMA, and any discrepancies were explored until an agreement was reached.
Qualitative Analysis
Two researchers independently analyzed the quality of each RCT study by conducting critical appraisals based on Cochrane Review guidelines. The qualitative analysis was carried out using the Risk of Bias 2 (RoB2) instrument, and the risk of bias was evaluated across six major domains. For parallel RCT studies, the five domains included were the randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result. Furthermore, period and carryover effects, or Domain S, were assessed as additional domains for cross-over RCT studies. Questions from each domain can be answered with multiple choices, such as “Yes,” “Probably Yes,” “No,” “Probably No,” or “No Information.” The overall risk of bias criteria was expressed as “Low” for the low RoB, “Some Concerns” for some domains that need attention but are not in the form of a high RoB, and “High” for the high RoB. GRADE tool was used in systematic reviews to assess the quality of an evidence body. This tool graded the RoB, indirectness, inconsistency, the risk of publication bias, and imprecision. The conclusion of the GRADE was reflected in the certainty level, which started from very low to high certainty 16.
Quantitative Analysis
The meta-analysis was conducted using the fixed-effect model generated from the Cochrane Collaboration’s Review Manager software version 5.4.1, and the included studies were displayed through a forest plot. The results were presented as a weighted mean difference (WMD) or standardized mean difference (SMD) for continuous outcomes. For continuous data on the same scale, weighted mean difference (WMD) was used to present the overall meta-analysis result, and 95% confidence intervals (CI95%) were applied. Heterogeneity was also evaluated and presented as I2>50%.
Results and Discussion
Selection of Studies
The literature search was conducted until May 2023 using the 2020 PRISMA flowchart guide, which was divided into three flow sections: identification, screening, and inclusion, as presented in Figure 1. Numerous studies were excluded for several reasons, including irrelevant reporting outcomes, participants who also had comorbid irritable bowel syndrome, used non-placebo comparators, had unfinished clinical trials, and originated in the same trial. Databases yielded information on 160 studies in total. After critically appraising the individual studies, five studies were selected for systematic review and meta-analyses by considering feasibility study, inclusion, and exclusion criteria.
 |
Figure 1: PRISMA Flowchart |
Characteristic of Studies
The characteristics of each selected study are displayed in Table 1. From 2002 to 2018, the research included four cross-over RCT studies and one parallel RCT study. This study involved 175 subjects: 93 from a cross-over study and 82 from a parallel study design. There were more female subjects than males in the overall RCT studies. All participants in each study were healthy individuals with symptoms of constipation and aged between ≥18 years old. Constipation was characterized as having less than three bowel movements each week, straining at least 25% of the defecation process, and experiencing a minimum of 25% of the bowel movement incompletely. Kiwifruit interventions varied in powder, extract, and whole fruit forms. The duration of the intervention ranged from three days to four weeks. Of the five studies, four utilized green kiwifruit, and one employed green and gold species 12–14,17.
 |
Table 1: Characteristic of Studies |
Qualitative Analysis
We used the RoB2 application to analyze the studies’ quality. Our results indicate that low-risk bias was present in one study, and high-risk bias was present in three studies, as in Table 2 and Figure 2. Among all studies, the highest RoB occurred in deviations from the intended intervention (D2). Finally, low certainty results were obtained after assessing the RoB by the GRADE system, as seen in Table 3.
Table 2: Risk of Bias (RoB2) Results of Each Study
|
Study |
D1 |
DS |
D2 |
D3 |
D4 |
D5 |
Overall Bias |
|
Study A Udani et al. (2013) |
+ |
N/A |
+ |
+ |
+ |
+ |
+ |
|
Study B Kindleysides et al. (2015) |
! |
+ |
+ |
+ |
+ |
+ |
! |
|
Study C Wilkin-Smith et al. (2019) |
– |
+ |
– |
+ |
– |
+ |
– |
|
Study D Ansell et al. (2015) |
+ |
+ |
– |
+ |
+ |
+ |
– |
|
Study E Rush et al. (2002) |
! |
– |
– |
+ |
– |
+ |
– |
Description: + Low risk ! Some concerns – High risk
DS Period and carry-over effects
D1 Randomization process
D2 Deviations from intended intervention
D3 Missing outcome ßdata
D4 Measurement of the outcome
D5 Selection of the reported result
N/A Parallel group
 |
Figure 2: Overall Results of Risk of Bias (RoB2). |
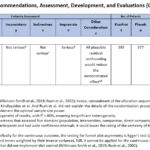 |
Table 3: Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) Analysis Results |
Quantitative Analysis
Five studies were analyzed quantitatively regarding defecation frequency as the primary outcome of this study. According to Ansell et al., kiwifruit intervention consisted of low-dose green, high-dose green, and gold kiwifruit. Therefore, the outcome values were entered separately in the forest plot. Udani et al. displayed outcome scores separately for both the intervention and comparator groups from week 1 to week 4 in the forest plot following the original study 12. Meanwhile, Rush et al. displayed two data sets: the preliminary data, including healthy adults, and the main data, including healthy elderly 18. According to the forest plots, the kiwifruit intervention significantly increased defecation frequency (p = 0.0008), with a WMD of 0.07 (95% CI 0.03–0.11), as seen in Table 4.
 |
Table 4: Forest Plot of Defecation Frequency Outcome |
The inability to convert studies into forest plots is due to the small amount of research that expresses secondary outcomes by means, standard deviation (SD), or mean standard error (SE) and the fact that not all studies evaluate secondary outcomes. Although some minor side effects, such as flatulence, bloating, and nausea, were reported in several studies, no serious side effects were found after consuming kiwifruit. The two RCTs conducted by Wilkinson-Smith et al. and Ansell et al. demonstrated non-significant adverse effects between groups 13,14.
The quantitative analysis of five studies showed that kiwifruit significantly increased the frequency of defecation. Our results are similar to the previous study, which included subjects with irritable bowel syndrome (IBS), where kiwifruit was effective in increasing defecation frequency. However, the prior meta-analysis’s studies had a very high level of heterogeneity (I2>50%) 19, while this analysis included more homogenous studies (I2=46%). This indicated that kiwifruit could be recommended in constipation patients without comorbidities to support the role of fibers and actinidin in promoting defecation 7,20. Heterogeneity is also an essential component of meta-analysis to draw overall conclusions 21.
In this study, we also consider the term clinically significant, which can be used in which clinically relevant outcomes are used to assess the effectiveness of a treatment modality 22. Despite statistically significant findings, the therapeutic advantages of kiwifruit are negligible. WMD was found to increase defecation frequency by 0.07, which is not considerably different from the placebo group. The clinical impact of kiwifruit on functional constipation has to be confirmed by more clinical studies.
Regarding quality, these results must be applied carefully; although promising heterogeneity levels exist, some studies had a high RoB. A study with the largest overall number of participants (n = 86) by Rush et al. had 68.9% of the overall weight of the defecation frequency outcome, which significantly affected this meta-analysis since it comprised more than half of the overall weighted effect, categorized as high RoB. Meanwhile, the second largest study, with 29.8% of the overall weighted effect, was ranked as low RoB, followed by high bias with 0.8% and 0.3% overall weighted effects from the third and fourth largest studies. Half of the studies had insufficient D2 components of RoB due to a failure in implementing the intervention on several participants to have sufficient power. Studies with D2 insufficiency had several participants drop out, lowering their power and influencing the study’s validity 23. Regarding the D1 component of RoB, the insufficiency was found in three studies, where no detailed explanation about the sequence allocation was shown, including the blinding process of allocation, specifically for the parallel RCT design study. The recipients of the intervention were known to both the participants and the researchers, which can interfere with the results. Two of the studies did not meet the criteria for the D4 component of RoB, and blinding of intervention was not performed. This study also used diary filling as a patient-reported outcome. The absence of patients’ blinding increased impact estimates by an average SD of 0.56 (0.71 to 0.41) when outcomes were patient-reported, as indicated in the systematic review 24, which can cause a potential bias. Regarding the DS component, one cross-over study did not implement a wash-out period that could lead to carry-over effects.
We carried out a GRADE analysis to evaluate the feasibility of this study 25. Our result from the GRADE analysis emphasized the importance of further studies on kiwifruit’s efficacy in overcoming constipation symptoms. Serious imprecision and the possibility of plausible residual confounding detected in two studies, where diet control still needs to be implemented, could be undiagnosed confounders, thus affecting the measured outcomes 26.
The limitations of this meta-analysis included the variation between studies’ dosages and formulations. Regarding the dosage, one study showed that consuming two kiwifruits every day can increase the laxative effect. It is also possible that the Wilkin-Smith et al. study showed significant results in increasing defecation after participants consumed two kiwifruits with an average weight of 150 g for one kiwi. Meanwhile, other studies used smaller doses of kiwifruit 27. Although subgroup analysis was not performed due to the need for a larger number of studies and data, the meta-analysis of defecation frequency showed considerably low heterogeneity between studies. Secondly, the inability to perform sensitivity analysis is due to the limited number of studies included. To overcome the RoB, performing sensitivity analysis is highly recommended. The third weakness of this study is the varied definitions of constipation in the included studies that can cause differences among the subjects. ROME III was used in two studies, while the rest did not apply the standardized definition of functional constipation. Studies showed that varied definitions might lead to various prevalence 28, which could interfere with the study results. The fourth limitation is the limited access to EMBASE, which should have enhanced the comprehensiveness of the search. However, since we used the CENTRAL database, which supports EMBASE29, we anticipated that all articles would be noticed. Meanwhile, this limitation was compensated by using other databases 30.
Conclusion
Based on statistical research, daily ingestion of kiwifruit is regarded safe and may have a considerable impact on increasing the frequency of bowel movements. However, there is no clinical evidence to support this claim. Additional research is required to ascertain the clinical and statistical impact of kiwifruit on functional constipation.
Acknowledgement
Fonny Cokro: Conceptualization, Methodology, Formal Analysis, Investigation, Resources, Writing – Review and Editing
Ervina Vashti: Methodology, Investigation, Validation, Formal Analysis, Writing – Original Draft
Agustina Dwi Retno Nurcahyanti: Methodology, Formal Analysis, Investigation, Writing – Review, and Editing
Anton Sumarpo: Methodology, Formal Analysis, Investigation, Writing – Review, and Editing
Rungnapa Malasao: Methodology, Formal Analysis, Investigation, Writing – Review, and Editing
Conflict of Interest
The authors declare there are no competing interests.
Funding Source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Jani B, Marsicano E. Constipation: Evaluation and Management. Mo Med. 2018;115(3):236-240.
- Aziz I, Whitehead WE, Palsson OS, Törnblom H, Simrén M. An approach to the diagnosis and management of Rome IV functional disorders of chronic constipation. Expert Rev Gastroenterol Hepatol. 2020;14(1):39-46. doi:10.1080/17474124.2020.1708718
CrossRef - Tamura A, Tomita T, Oshima T, et al. Prevalence and Self-recognition of Chronic Constipation: Results of an Internet Survey. J Neurogastroenterol Motil. 2016;22(4):677-685. doi:10.5056/jnm15187
CrossRef - Portalatin M, Winstead N. Medical Management of Constipation. Clin Colon Rectal Surg. 2012;25(1):12-19. doi:10.1055/s-0032-1301754
CrossRef - Bae SH. Diets for Constipation. Pediatr Gastroenterol Hepatol Nutr. 2014;17(4):203-208. doi:10.5223/pghn.2014.17.4.203
CrossRef - Yamada M, Sekine M, Tatsuse T, Fujimura Y. Lifestyle, psychological stress, and incidence of adolescent constipation: results from the Toyama birth cohort study. BMC Public Health. 2021;21(1):47. doi:10.1186/s12889-020-10044-5
CrossRef - Richardson DP, Ansell J, Drummond LN. The nutritional and health attributes of kiwifruit: a review. Eur J Nutr. 2018;57(8):2659-2676. doi:10.1007/s00394-018-1627-z
CrossRef - Chang CC, Lin YT, Lu YT, Liu YS, Liu JF. Kiwifruit improves bowel function in patients with irritable bowel syndrome with constipation. Asia Pac J Clin Nutr. 2010;19(4):451-457.
- Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014;146(1):67-75.e5. doi:10.1053/j.gastro.2013.09.046
CrossRef - Bassotti G, Chistolini F, Marinozzi G, Morelli A. Abnormal colonic propagated activity in patients with slow transit constipation and constipation-predominant irritable bowel syndrome. Digestion. 2003;68(4):178-183. doi:10.1159/000075554
CrossRef - Boland M. Kiwifruit proteins and enzymes: actinidin and other significant proteins. Adv Food Nutr Res. 2013;68:59-80. doi:10.1016/B978-0-12-394294-4.00004-3
CrossRef - Udani JK, Bloom DW. Effects of kivia powder on Gut health in patients with occasional constipation: a randomized, double-blind, placebo-controlled study. Nutrition Journal. 2013;12(1):78. doi:10.1186/1475-2891-12-78
CrossRef - Wilkinson-Smith V, Dellschaft N, Ansell J, et al. Mechanisms underlying effects of kiwifruit on intestinal function shown by MRI in healthy volunteers. Aliment Pharmacol Ther. 2019;49(6):759-768. doi:10.1111/apt.15127
CrossRef - Ansell J, Butts CA, Paturi G, et al. Kiwifruit-derived supplements increase stool frequency in healthy adults: a randomized, double-blind, placebo-controlled study. Nutr Res. 2015;35(5):401-408. doi:10.1016/j.nutres.2015.04.005
CrossRef - Cochrane Handbook for Systematic Reviews of Interventions. Accessed September 8, 2022. https://training.cochrane.org/handbook
- Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE handbook. Published October 2013. Accessed February 21, 2023. https://gdt.gradepro.org/app/handbook/handbook.html
- Kindleysides S, Kuhn-Sherlock B, Yip W, Poppitt SD. Encapsulated green kiwifruit extract: a randomised controlled trial investigating alleviation of constipation in otherwise healthy adults. Asia Pac J Clin Nutr. 2015;24(3):421-429. doi:10.6133/apjcn.2015.24.3.15
- Rush EC, Patel M, Plank LD, Ferguson LR. Kiwifruit promotes laxation in the elderly. Asia Pac J Clin Nutr. 2002;11(2):164-168. doi:10.1046/j.1440-6047.2002.00287.x
CrossRef - Antonelli M, Donelli D. Kiwifruit (Actinidia spp.) Dietary Consumption for Constipation: A Systematic Review and Meta-Analysis. Future Pharmacology. 2021;1(1):27-40. doi:10.3390/futurepharmacol1010003
CrossRef - Bayer SB, Gearry RB, Drummond LN. Putative mechanisms of kiwifruit on maintenance of normal gastrointestinal function. Critical Reviews in Food Science and Nutrition. 2018;58(14):2432-2452. doi:10.1080/10408398.2017.1327841
CrossRef - Fletcher J. What is heterogeneity and is it important? BMJ. 2007;334(7584):94-96. doi:10.1136/bmj.39057.406644.68
CrossRef - Sharma H. Statistical significance or clinical significance? A researcher’s dilemma for appropriate interpretation of research results. Saudi J Anaesth. 2021;15(4):431-434. doi:10.4103/sja.sja_158_21
CrossRef - Parker RM. Power, Control, and Validity in Research. J Learn Disabil. 1990;23(10):613-620. doi:10.1177/002221949002301008
CrossRef - Hróbjartsson A, Emanuelsson F, Skou Thomsen AS, Hilden J, Brorson S. Bias due to lack of patient blinding in clinical trials. A systematic review of trials randomizing patients to blind and nonblind sub-studies. International Journal of Epidemiology. 2014;43(4):1272-1283. doi:10.1093/ije/dyu115
CrossRef - Zhang X, Donnan PT, Bell S, Guthrie B. Non-steroidal anti-inflammatory drug induced acute kidney injury in the community dwelling general population and people with chronic kidney disease: systematic review and meta-analysis. BMC Nephrol. 2017;18(1):256. doi:10.1186/s12882-017-0673-8
CrossRef - Verbeek JH, Whaley P, Morgan RL, et al. An approach to quantifying the potential importance of residual confounding in systematic reviews of observational studies: A GRADE concept paper. Environment International. 2021;157:106868. doi:10.1016/j.envint.2021.106868
CrossRef - Gearry R, Fukudo S, Barbara G, et al. Consumption of 2 Green Kiwifruits Daily Improves Constipation and Abdominal Comfort—Results of an International Multicenter Randomized Controlled Trial. Official journal of the American College of Gastroenterology | ACG. 2023;118(6):1058. doi:10.14309/ajg.0000000000002124
CrossRef - Barberio B, Judge C, Savarino EV, Ford AC. Global prevalence of functional constipation according to the Rome criteria: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(8):638-648. doi:10.1016/S2468-1253(21)00111-4
CrossRef - How CENTRAL is created | Cochrane Library. Accessed May 16, 2023. https://www.cochranelibrary.com/central/central-creation
- Wong SSL, Wilczynski NL, Haynes RB. Comparison of top-performing search strategies for detecting clinically sound treatment studies and systematic reviews in MEDLINE and EMBASE. J Med Libr Assoc. 2006;94(4):451-455.
- Kulich KR, Madisch A, Pacini F, et al. Reliability and validity of the Gastrointestinal Symptom Rating Scale (GSRS) and Quality of Life in Reflux and Dyspepsia (QOLRAD) questionnaire in dyspepsia: A six-country study. Health Qual Life Outcomes. 2008;6:12. doi:10.1186/1477-7525-6-12
CrossRef - Rome IV Criteria. Rome Foundation. Accessed February 24, 2023. https://theromefoundation.org/rome-iv/rome-iv-criteria/
- Schmulson MJ, Drossman DA. What Is New in Rome IV. J Neurogastroenterol Motil. 2017;23(2):151-163. doi:10.5056/jnm16214
CrossRef - Blake MR, Raker JM, Whelan K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Alimentary Pharmacology & Therapeutics. 2016;44(7):693-703. doi:10.1111/apt.13746
CrossRef




