The Role of Interleukin-6 and Procalcitonin in Kidney Patients have Bacterial and Viral Infection
 and Jawad Kadhum Muraih*
and Jawad Kadhum Muraih* Department of chemistry, College of Science, Al-Muthanna University, Samawah, Iraq
Corresponding Author E-mail: jmuraih@mu.edu.iq
DOI : http://dx.doi.org/10.13005/bpj/2874
Download this article as:
![]()
Background: IL-6 is one of the most studied cytokines in kidney disease. It is making inflammation worse by activating B cells that affect the production of hepatic acute phase proteins. It is also involved in metabolic, regenerative, and neurological processes Procalcitonin (PCT) is a typical biomarker for bacterial infections. since it increases in response to bacterial infections but not to other inflammatory reactions such as viral infections. Aim: study the role of IL-6 and PCT on renal failure that is affected by bacterial and viral infection. Methods: Between January and April 2023, 120 patients were confirmed to have chronic renal failure with or without diabetes mellitus who were affected or not via bacterial or viral infections based on previous medical reports and were divided into six groups; each of them included 20 patients. IL-6 and PCT levels were assayed and compared among groups. Different groups had very significantly different levels of IL-6 (90.40±25.77 for patients in G1, 42.33±17.32 for patients in G2, 84.95±19.80 for patients in G3, and 36.68±15.10 for patients in G4). The levels were 2.44±0.79 for patients in G5 and 2.26±0.59 for the control group, respectively (p<0.0001). The levels of PCT were also significantly different between groups (4.77±1.86 for patients in G1; 0.31±0.09 for patients in G2; 4.41±1.43 for patients in G3; 0.28±0.09 for patients in G4). The levels were 0.04±0.01 for patients in G5 and 0.03±0.01 for the control group, respectively (p<0.0001). Results: The findings demonstrated significant in levels of interleukin-6, urea, and creatinine in all patients except diabetic patients and significant increase in the level of procalcitonin in patients who have a bacterial infection, not a viral infection. Conclusion: The level of IL-6 increases in renal failure in both bacterial and viral infection states, but the Procalcitonin level increases in bacterial infection only.
KEYWORDS:Creatinine; Interleukin-6; PCT; Renal failure; Urea
Introduction
After the discovery of interleukin-6 (IL-6) in 1986 as a B-cell stimulatory factor that begins IgG production, it was found to be a pleiotropic cytokine that regulates a wide variety of physiopathological processes, including cell proliferation, survival, migration, invasion, metastasis, angiogenesis, inflammation, and metabolism 1. While monocytes and macrophages account for the vast majority of IL-6 production, other cell types, including T cells, B cells, hepatocytes, endothelial cells, fibroblasts, keratinocytes, mesangial cells, adipocytes, and even certain tumor cells, are capable of producing IL-6 either constitutively or in response to stimulation 2,3. In response to microbial stimulation, monocytes and macrophages (MO/M ) release IL-6 4.
The inflammatory effects of IL-6 may be either pro- or anti-inflammatory. The anti-inflammatory effects of IL-6 include stopping bacterial infections, increasing the growth of epithelial cells, and stopping epithelial cells from giving up 1. In contrast, IL-6 exhibits pro-inflammatory activity when there is no control over its production; consequently, an increase in the release of this cytokine can be a symptom of the syndrome known as cytokine storm5. A cytokine storm is a condition in which a wide variety of immune-active molecules, such as chemokines and cytokines, are released from the immune system at extremely high concentrations6.
Weakness, fever, muscular discomfort, and other symptoms are all caused by both bacterial and viral diseases. Differentiating between these two kinds of infections as soon as possible is crucial for effective treatment and a positive prognosis. Antibiotics are often used to treat bacterial infections; however, they are ineffective against viral infections and may even lead to the spread of antibiotic resistance 7.
IL-6 is up-regulated fast and transiently during viral or bacterial pathogenic invasion. Rapid elevation of IL-6 following bacterial infection, with a peak at 2 h, is significantly connected with disease severity. Acute increases in IL-6 levels can occur in response to viral infection and inflammation. IL-6 is a reliable indicator of stress responses and plays a key role in the adaptive immune response by stimulating B cells to produce antibodies and inducing the differentiation of naive CD4+ T cells into effector T cells. IL-6 rises first in response to inflammation and stays elevated for longer than other cytokines. In comparison with C-reactive protein (CRP) and procalcitonin (PCTs), it is useful for screening acute infections in their earliest stages1,4,8.
Procalcitonin (PCT) is a prohormone secreted by the thyroid gland. Procalcitonin (PCT) is located on the CALC-1 gene on chromosome 11, a 116-amino-acid polypeptide9. IL-6, TNF-a, and IL-1 induce PCT production in extrathyroidal tissue in response to bacterial infection. PCT is bacterial-specific since its synthesis is inhibited during most viral infections due to an increase in interferon-γ production10.
Procalcitonin has gained popularity as a diagnostic tool for bacterial infections and sepsis in recent years. Since serum PCT levels may rise within a few hours after inflammation and often peak within 24 to 48 hours, their specificity is greater than that of other frequent laboratory indicators such as leukocytosis, increased band cells, and C-reactive protein (CRP). Serum PCT increases have been seen in patients with severe systemic fungal or parasitic infections, in addition to those with bacterial infections and sepsis. While PCT values are too low or not at all in viral infections, the cytokines produced during viral infections are mostly responsible for this since they inhibit the synthesis of tumor necrosis factor-a (TNF-a). Therefore, serum PCT levels are an excellent indicator that distinguishes between bacterial and viral illnesses11,12.
Chronic kidney disease (CKD) progresses to its last irreversible stage, which is known as end-stage renal disease (ESRD). This stage is characterized by a steady decrease in kidney function that ultimately results in kidney failure. ESRD is linked to a worse quality of life, death at an earlier age, and increased expenses for the whole healthcare system13. Loss of kidney function is linked to the failure to properly eliminate several types of uremic toxins. They are both the cause and the effect of CKD because of their biological activity14.
IL-6 is one of the cytokines that has been studied the most in kidney disease. It is making inflammation worse by activating B cells and causing the production of hepatic acute phase proteins. It is also involved in metabolic, regenerative, and neurological processes8. The presence of elevated plasma interleukin-6 (IL-6) levels is frequently observed in patients with chronic kidney disease (CKD). This phenomenon is primarily attributed to heightened production as a consequence of oxidative stress, chronic inflammation, and fluid overload. In addition, diminished renal function plays a role in the accumulation of IL-6 by reducing its clearance. Both therapeutic hemodialysis and peritoneal dialysis have been shown to increase the production of interleukin-6 (IL-6) in people with end-stage renal disease (ESRD) as a result of the inflammation. Researchers have found that interleukin-6 (IL-6) speeds up the progression of chronic kidney disease (CKD) by making kidney damage worse and causing complications like chronic vascular disease (CVD) 3. The objective of the study is to investigate the role of interleukin-6 and PCT in the severity of microbial injury in kidney patients.
Materials and Methods
Patients and Groups
The current study included 120 patients, divided into six groups of 20 patients to each.
Groups 1, have patients with chronic renal failure and diabetes mellitus with bacterial infection.
Group 2, , have patients with chronic renal failure and diabetes mellitus with viral infection.
Group 3, have patients with chronic renal failure with bacterial infection.
Group 4, , have patients with chronic renal failure with viral infection.
The patients are 40 years of age and older and were admitted to the Al-Hussein Teaching Hospital in the Al Muthanna Government during the period from January 2023 to the end of April 2023. All patients were diagnosed as having chronic renal failure with a bacterial or viral infection based on previous medical reports, laboratory tests, and clinical examinations by consultant nephrologists.
Group 5, 20 subjects with diabetes mellitus.
Control group, 20 healthy subjects with an age group of 40 years and up.
The control group subjects were selected as healthy individuals without a history of kidney disease, current or previous kidney stones, diabetes mellitus, or hypertension, depending on previous medical reports and laboratory investigations. Blood samples (5 mL) were taken from each patient and healthy individuals.
Samples
The blood samples were centrifuged at 3000 × g at 4 °C for 10 min. The serum was removed, aliquoted in some vials, and stored at -20 °C. The serum was used for the detection of biochemical parameters, including urea, creatinine, IL-6, and PCT. Laboratory diagnosis depended on using an auto-analyzer known as the Cobas C111 in Germany for the estimation of serum urea and creatinine. Additionally, Getein 1100 identified IL-6 and PCT. Methods were conducted according to the instructions in the manufacturing company leaflet.
Statistical analysis
This study designed by Completely randomized design (CRD) that used in the analysis of variance for study parameters by using one-way ANOVA test and independent t-test. Moreover, Dunnett’s Test was used for comparison of study parameters between study groups and control group. Regarding linear correlation, Pearson’s Correlation Coefficient was used. Data were processed and analyzed by using statistical program social science (SPSS 22) and the results were expressed as Mean±SD (McDonald, 2014)15.
Results
This study showed a significant variance in IL-6 parameters means among six study groups, where the p value was <0.0001. The results showed a significant difference when compared between all groups with a control group (a- p<0.0001*) and between the first group ( RF, DM and BI) with control (a- p<0.0001*), also when compared between the second group ( RF, DM and VI ), third group ( RF and BI) and fourth group ( RF and VI) with control, (b, c, d, e – p<0.0001*). However, the fifth group (DM) showed there is no significant difference when compared with the control group ( f- p = 0.972).
For PCT measurements, the results showed a significant variance in PCT parameters means among six study groups, where the p value was <0.0001. In comparison between all groups versus a control, we found p-value is less than 0.0001(a- p<0.0001*). Also, there is significant difference when compared between the first group ( RF, DM and BI) and the third group ( RF and BI), with control (b, d, – p<0.0001*), but there is no significant difference in comparison between the second group ( RF, DM and VI ), fourth group ( RF and VI) and fifth group (DM) with control (c- p=0.826, e. p=0.873 and f- p=0.982 respectively). These results are shown in table (1) and figure (1).
Table 1: Comparison of study parameters (PCT and IL-6) among study Groups. Asterisks represent the significance. Number of patients = 20 to each group.
|
P value |
Mean ± St. Deviation |
Groups |
|
|
<0.0001* |
4.7720 ± 1.86547 |
G1 |
PCT |
|
<0.0001* |
0.3150 ± 0.09378 |
G2 |
|
|
0.826 |
4.4160 ± 1.43331 |
G3 |
|
|
0.0001* |
0.2895 ± 0.09110 |
G4 |
|
|
0.873 |
0.0430 ± 0.01895 |
G5 |
|
|
0.982 |
0.0360 ± 0.01930 |
Control |
|
|
<0.001* |
90.400 ± 25.77949 |
G1 |
IL6 |
|
<0.001* |
42.3350 ± 17.32592 |
G2 |
|
|
<0.001* |
84.9500 ± 19.80424 |
G3 |
|
|
<0.001* |
36.6800 ± 15.10833 |
G4 |
|
|
<0.001* |
2.4400 ± 0.79565 |
G5 |
|
|
0.972 |
2.2600 ± 0.59683 |
Control |
|
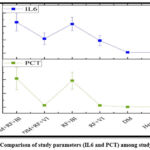 |
Figure 1: Comparison of study parameters (IL6 and PCT) among study Groups |
The results for Urea and creatinine parameters means showed there is a significant difference among all groups when compared with control since the p-value was <0.0001, except for the fifth group (DM) there is no significant difference with the control group. These results are shown in table (2,3) and figure (2).
Table 2: Comparison of study parameter (Urea) among study Groups . Asterisks represent the significance. Number of patients = 20 to each group.
|
Groups |
Mean ± St. Deviation |
P value |
|
|
Urea |
G1 |
124.0850 ± 19.18674 |
<0.0001* |
|
G2 |
129.3700 ± 39.84359 |
<0.0001* |
|
|
G3 |
120.1950 ± 45.37441 |
<0.0001* |
|
|
G4 |
117.4900 ± 27.26289 |
<0.0001* |
|
|
G5 |
32.6500 ± 7.57611 |
<0.0001* |
|
|
Control |
26.6000 ± 7.87000 |
0.943 |
|
Table 3: Comparison of study parameters (Creatinine) among study Groups. Asterisks represent the significance. Number of patients = 20 to each group.
|
Groups |
Mean ± St. Deviation |
P value |
|
|
Creatinine |
G1 |
6.2300 ± 1.87283 |
0.0001* |
|
G2 |
6.9950 ± 2.29174 |
0.0001* |
|
|
G3 |
8.3795 ± 3.12715 |
0.0001* |
|
|
G4 |
8.6150 ± 2.26838 |
0.0001* |
|
|
G5 |
0.6900 ± 0.17741 |
0.0001* |
|
|
Control |
0.6925 ± 0.18934 |
0.997 |
|
 |
Figure 2: Comparison of study parameters (urea and creatinine) among study Groups |
Discussion
Interleukin-6 (IL-6) is one of the pro-inflammatory cytokines. Infection, inflammation, obesity, and stress all play a role in triggering IL-6 production16. Foreign bodies, hemodialysis catheters, arteriovenous fistulas, and the hemodialysis technique all contribute to inflammation. Chronic stress and negative feelings can also lead to increased cytokine levels17. Infections caused by bacteria and viruses pose a serious threat to people with CKD. High morbidity and mortality rates have been linked to bacterial infections in hemodialysis (HD) patients18. Patients on dialysis may have inflammation for a number of reasons, including those connected to the dialysis procedure itself, to the underlying cause of renal failure (such as oxidative stress), or to an infection. It appears that exposing blood to bioincompatible dialysis membranes is a significant contributor to chronic inflammation connected to dialysis. White blood cells and complement are triggered by cellulosic membranes and other bioincompatible membranes19. Studies show that the cytokine IL-6 promotes inflammation. As a result of a bacterial infection, it helps kick off the acute phase response in humans. The serum level of interleukin-6 (IL-6) is modest in healthy individuals but rises substantially during the early phase of bacterial infection20. In viral infections, the cytokines are implicated in establishing an antiviral state as the unspecific first line of defense and virus-specific response. PRRs, which can exist as transmembrane receptors or in other intracellular compartments, are responsible for kicking off this process by recognizing viral organisms. Changes in the receptor’s structure initiate a signaling pathway in the cytoplasm that ultimately leads to the translocation of cytoplasmic transcription factors into the nucleus, where they boost the production of several cytokines. Cytokine production might differ in kind depending on the virus and the cell type21. They may be able to recognize cells that have been infected by a virus and exert control over inflammatory and immunological responses, the removal of viruses, and processes that cause harm to tissue. It is known that both HBV and HCV infections can alter a wide range of cytokine activities. An imbalance in the production of pro-inflammatory and anti-inflammatory cytokines is what drives the immunopathogenesis of HBV and HCV infections22. The lower level of IL-6 in people with type 2 diabetes compared to a healthy control group, on the other hand, suggests that cell-mediated immunity may be weakened in people who are taking medications to control their blood sugar levels23. Most previous results agreed with ours. This means that the increase in IL-6 is due to a bacterial or viral infection of the failed kidney, and there is no effect of diabetes on IL-6.
An increasingly popular biomarker for bacterial infections is procalcitonin (PCT). PCT is greatly raised in response to stimulation by pathogens, although its level in otherwise healthy people is below the detection threshold (0.01 ng/mL)24. PCT levels in the blood can rise within hours of inflammation and usually reach their highest point within 24 to 48 hours. This makes them more specific than other common lab markers like leukocytosis, increased band cells, and C-reactive protein (CRP). Patients with bacterial infections and sepsis have elevated serum PCT levels, while those with viral infections have lower PCT values or none at all. This is mainly because cytokines created during viral infections inhibit the generation of tumor necrosis factor-a. As a result, PCT levels in the serum are a reliable and accurate indicator for distinguishing bacterial from viral illnesses12.Our results showed a non-significant difference in the level of PCT in type 2 diabetes mellitus compared with the control group. Insulin may have anti-inflammatory effects apart from its impact on blood sugar, according to several studies. Increased endothelial nitric oxide release, decreased expression of proinflammatory cytokines, and immune system suppression are some of the ways insulin reduces inflammation. This could be the reason why the PCT levels were low in diabetic patients, as in the study25. Our findings corroborated who reported that patients with diabetes mellitus had a decrease in PCT concentration. This decrease was observed irrespective of the specific type of diabetes26.
The non-enzymatic conversion of creatine and phosphocreatine produces creatinine in muscle. The amount of creatinine produced is directly proportional to the amount of muscle mass. The liver plays a crucial role in the synthesis of creatinine by methylating guanidine amino-acetic acid27. Patients with chronic kidney disease who are on dialysis often have viral infections, which could be a result of contracting an infection while on dialysis. Time on hemodialysis and infection prevalence within hemodialysis units are inversely related to the probability of transmission. The results of our study showed that patients who have renal failure with DM and viral infection showed significantly higher levels of creatinine than the controls. These results agreed with the results of a study carried out, which found that out of the 164 patients, 26 tested positive for viruses. Serum creatinine in viral-infected CKD patients was higher than in non-viral-infected CKD patients28.
Additionally, this study demonstrated that type 2 diabetes mellitus did not significantly affect serum creatinine concentration in comparison to the control group. This agreed with the results of the previous study, which showed that low serum creatinine increases the risk of type 2 diabetes. Some results postulated that a smaller amount of skeletal muscle would correlate with a lower serum creatinine level. When skeletal muscle stops responding to insulin, it sets off a cascade of events that culminate in the development of type 2 diabetes29.
Urea is an organic compound that is produced as a result of protein metabolism in the human body. It is non-toxic and plays a crucial role in eliminating 80–90% of the nitrogen waste. Elevated blood urea levels indicate compromised renal function, while reduced urea levels can be attributed to impaired liver function and protein-energy deficiency30. According to the results of this study, the level of serum urea concentrations in viral infection and CKD was higher than in the control group. This study confirmed previous findings that chronic kidney disease and viral infections were linked to higher serum urea concentrations than non-viral infections and chronic kidney diseases28.
Results in this study showed a non-significant difference in the level of Urea in type 2 diabetes mellitus compared with the control group. These results are in agreement with Kurniawan and Kusrini who found that more than 80% of the diabetic participants had normal urea levels (≤40 mg/dL). In the group of patients aged 45 years and up, the average urea level was 34.54 mg/dL, which is still considered normal. This finding shows that diabetics still have normal kidney function, which means it is possible to manage a diabetic to keep blood sugar levels under control 31 .
Conclusion
It is clear depending on our obtained findings that, the level of interleukin – 6 increases in case of renal failure accompanied by either bacterial or viral infections. Considering the procalcitonin, it was seen to elevate in case of renal failure accompanied with bacterial infection only.
Acknowledgement
The authors of this study offer their grateful thanks to the laboratory staff of Dialysis center for their cooperation and assistance throughout my stay with them at Al-Hussein Teaching Hospital.
Conflicts of interest
No conflict of interest from authors regarding the publication of this manuscript.
Funding source
There are no funding sources
References
- Li YS, Ren HC, Cao JH. Roles of Interleukin-6-mediated immunometabolic reprogramming in COVID-19 and other viral infection-associated diseases. International Immunopharmacology. 2022;110:109005. doi:10.1016/j.intimp.2022.109005
CrossRef - Drucker C, Gewiese J, Malchow S, Scheller J, Rose-John S. Impact of interleukin-6 classic- and trans-signaling on liver damage and regeneration. Journal of Autoimmunity. 2010;34(1):29-37. doi:10.1016/j.jaut.2009.08.003
CrossRef - Su H, Lei CT, Zhang C. Interleukin-6 Signaling Pathway and Its Role in Kidney Disease: An Update. Front Immunol. 2017;8:405. doi:10.3389/fimmu.2017.00405
CrossRef - Zhu K, Lu XJ, Jian-Fei Lu, Chen J. The interleukin-6 regulates the function of monocytes/macrophages (MO/MФ) via the interleukin-6 receptor β in ayu (Plecoglossus altivelis). Fish & Shellfish Immunology. 2019;93:191-199. doi:10.1016/j.fsi.2019.07.049
CrossRef - Perrone F, Piccirillo MC, Ascierto PA, et al. Tocilizumab for patients with COVID-19 pneumonia. The single-arm TOCIVID-19 prospective trial. J Transl Med. 2020;18(1):405. doi:10.1186/s12967-020-02573-9
CrossRef - Majidpoor J, Mortezaee K. Interleukin-6 in SARS-CoV-2 induced disease: Interactions and therapeutic applications. Biomedicine & Pharmacotherapy. 2022;145:112419. doi:10.1016/j.biopha.2021.112419
CrossRef - Largman-Chalamish M, Wasserman A, Silberman A, et al. Differentiating between bacterial and viral infections by estimated CRP velocity. Chen TH, ed. PLoS ONE. 2022;17(12):e0277401. doi:10.1371/journal.pone.0277401
CrossRef - Jones SA, Jenkins BJ. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nat Rev Immunol. 2018;18(12):773-789. doi:10.1038/s41577-018-0066-7
CrossRef - Sahu S, Dutta G. Emerging evidence for serum procalcitonin estimation at point-of-care and advancement in quantitative sensing strategies over the past decade. Sensors International. 2021;2:100107. doi:10.1016/j.sintl.2021.100107
CrossRef - Malinverni S, Lazzaroni S, Nuňez M, et al. Diagnostic Accuracy of Procalcitonin upon Emergency Department Admission during SARS-CoV-2 Pandemic. Antibiotics. 2022;11(9):1141. doi:10.3390/ antibiotics11091141
CrossRef - Sadeq SS, Muraih JK. CLINICAL SEVERITY OF COVID-19 INFECTION IN RELATION TO PEPTIDE PROCALCITONIN LEVEL AND OTHER FACTORS IN DIABETIC PATIENTS. 2022;22(2). doi:https://doi.org/ 10.31838/hiv22.02.309
CrossRef - Piperidou A, Zografos E, Vassilakopoulos TJ, et al. Serum Procalcitonin Levels in Newly Diagnosed Hodgkin Lymphoma: Correlation with Other Inflammatory Biomarkers. Medicina. 2022;58(10):1331. doi:10.3390/medicina58101331
CrossRef - Imamah NF, Lin HR. Palliative Care in Patients with End-Stage Renal Disease: A Meta Synthesis. IJERPH. 2021;18(20):10651. doi:10.3390/ijerph182010651
CrossRef - Rysz J, Franczyk B, Ławiński J, Gluba-Brzózka A. Oxidative Stress in ESRD Patients on Dialysis and the Risk of Cardiovascular Diseases. Antioxidants. 2020;9(11):1079. doi:10.3390/antiox9111079
CrossRef - McDonald JH. Handbook of Biological Statistics. 3rded. 2014, USA: Sparky House Publishing.
- Susilo H, Thaha M, Pikir BS, et al. The Role of Plasma Interleukin-6 Levels on Atherosclerotic Cardiovascular Disease and Cardiovascular Mortality Risk Scores in Javanese Patients with Chronic Kidney Disease. JPM. 2022;12(7):1122. doi:10.3390/jpm12071122
CrossRef - Turon-Skrzypinska A, Dutkiewicz G, Marchelek-Mysliwiec M, et al. Assessment of Sclerostin and Interleukin 6 Levels and Selected Anthropometric Parameters in Patients Receiving Hemodialysis Replacement Therapy-Pilot Study. Medicina (Kaunas). 2019;55(12):784. doi:10.3390/medicina55120784
CrossRef - Tao M, Zheng D, Liang X, He Q, Zhang W. Diagnostic value of procalcitonin for bacterial infections in patients undergoing hemodialysis: a systematic review and meta-analysis. Renal Failure. 2022;44(1):81-93. doi:10.1080/0886022X.2021.2021236
CrossRef - Bossola M, Sanguinetti M, Scribano D, et al. Circulating bacterial-derived DNA fragments and markers of inflammation in chronic hemodialysis patients. Clin J Am Soc Nephrol. 2009;4(2):379-385. doi:10.2215/CJN.03490708
CrossRef - Wu Y, Wang M, Zhu Y, Lin S. Serum interleukin-6 in the diagnosis of bacterial infection in cirrhotic patients: A meta-analysis. Medicine (Baltimore). 2016;95(41):e5127. doi:10.1097/MD.0000000000005127
CrossRef - Vatansever HS, Becer E. Relationship between IL-6 and COVID-19: to be considered during treatment. Future Virology. 2020;15(12):817-822. doi:10.2217/fvl-2020-0168
CrossRef - Khan S, Bhargava A, Pathak N, Maudar KewalK, Varshney S, Mishra PK. Circulating Biomarkers and their Possible Role in Pathogenesis of Chronic Hepatitis B and C Viral Infections. Ind J Clin Biochem. 2011;26(2):161-168. doi:10.1007/s12291-010-0098-7
CrossRef - Ekhlass N Ali, Ashwaq A Khadem, Muhammed HJ. Determination of IL-6 and CRP in Patients with Type Two -Diabetes Mellitus in Baghdad/ Iraq. Published online 2021. doi:10.13140/RG.2.2.23313.45924
- Wu SC, Liang CX, Zhang YL, Hu WP. Elevated serum procalcitonin level in patients with chronic kidney disease without infection: A case-control study. J Clin Lab Anal. 2020;34(2):e23065. doi:10.1002/jcla.23065
CrossRef - Al-Shammaree SAW, Abu-ALkaseem BA, Salman IN. Procalcitonin levels and other biochemical parameters in patients with or without diabetic foot complications. J Res Med Sci. 2017;22:95. doi:10.4103/jrms.JRMS_906_16
CrossRef - Usman A. 25-OH-Vitamin D and procalcitonin levels after correction of acute hyperglycemia. Med Sci Monit. 2013;19:264-268. doi:10.12659/MSM.883880
CrossRef - Samra M, Abcar AC. False estimates of elevated creatinine. Perm J. 2012;16(2):51-52. doi:10.7812/tpp/11-121
CrossRef - MA E, HB O, T D, LA E. IMPACT OF VIRAL INFECTIONS ON UREA AND CREATININE LEVELS IN PATIENTS WITH CHRONIC KIDNEY DISEASE ON HAEMODIALYSIS. JMBR. 2013;12(1):17-23.
- Harita N, Hayashi T, Sato KK, et al. Lower serum creatinine is a new risk factor of type 2 diabetes: the Kansai healthcare study. Diabetes Care. 2009;32(3):424-426. doi:10.2337/dc08-1265
CrossRef - Lin H, Wong GLH, Zhang X, et al. U-shaped relationship between urea level and hepatic decompensation in chronic liver diseases. Clin Mol Hepatol. 2022;28(1):77-90. doi:10.3350/cmh.2021.0188
CrossRef - Kurniawan MR, Kusrini E. UREUM AND CREATININE HEALTH STUDY IN PATIENTS DIABETES MELLITUS. IJMLST. 2020;2(2):85-92. doi:10.33086/ijmlst.v2i2.1565
CrossRef




