
Manuscript accepted on :05-07-2023
Published online on: 08-11-2023
Plagiarism Check: Yes
Reviewed by: Dr. Ahmed Salah
Second Review by: Dr. Randa Salah Gomez
Final Approval by: Dr. Ian James Martin
I Wayan Niryana* , Steven Awyono, Made Satriya Ranuwibawaand Christopher Lauren
, Steven Awyono, Made Satriya Ranuwibawaand Christopher Lauren
Neurosurgery Division, Department of Surgery, Faculty of Medicine, Universitas Udayana, Prof. Dr. I.G.N.G. Ngoerah General Hospital, Denpasar, Bali, Indonesia.
Corresponding Author E-mail: niryanawayan@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2828
Abstract
Microvascular decompression (MVD) is one of the well-established treatment options for trigeminal neuralgia that may include posterior fossa surgery. However, Several complications were noted as being part of posterior fossa surgery and hydrocephalus is very rare to occur, especially the slow-chronic onset type. The pathophysiology is still unclear, but surgeons and patients must be warned about this possible surgical adverse event. Here we report a case of slow-chronic hydrocephalus in a 66-years old male who has a history of MVD procedure due to left trigeminal neuralgia. A shunt procedure was performed, in which after the surgery the patient’s complaints were resolved, and discharged without any morbidity.
Keywords
Hydrocephalus; Microvascular decompression; Neurofunctional; Neurosurgery; Trigeminal neuralgia
Download this article as:| Copy the following to cite this article: Niryana I. W, Awyono S, Ranuwibawa M. S, Lauren C. Slow-Chronic Progressive Hydrocephalus as Complication of Microvascular Decompression for Trigeminal Neuralgia: A Case Report. Biomed Pharmacol J 2023;16(4). |
| Copy the following to cite this URL: Niryana I. W, Awyono S, Ranuwibawa M. S, Lauren C. Slow-Chronic Progressive Hydrocephalus as Complication of Microvascular Decompression for Trigeminal Neuralgia: A Case Report. Biomed Pharmacol J 2023;16(4). Available from: https://bit.ly/4741JdX |
Introduction
Idiopathic trigeminal neuralgia (TN) is a pathological condition caused by demyelination of the root entry zone of the fifth cranial nerve around the Obersteiner-Redlich zone. This zone is the transition between peripheral and central myelin, as this central myelin is vulnerable to injury, this neurovascular contact may then lead to the demyelination process.1 Microvascular decompression (MVD) is one of the well-established treatment options for trigeminal neuralgia that may include in posterior fossa surgery. However, due to its surgical nuances with minimal disruption of the surrounding neurovascular anatomy on the posterior fossa compartment, this procedure is thought to differ from conventional posterior fossa surgeries.2 Several complications were noted as being part of posterior fossa surgery and hydrocephalus is very rare to occur especially the slow-chronic onset type. Here we report a case of slow-chronic hydrocephalus related to MVD procedure.2,3
Case Report
A 66-years old male patient came with a chief complaint of unilateral face pain on the left side for the last 3 months. He had a history of taking analgesia for the last 3 weeks but the symptoms persist. On physical examination, we found an electric-like shock over the distribution of the left trigeminal nerve. From radiological examination using magnetic resonance angiography, we found a neurovascular conflict between the left superior cerebellar artery with the left trigeminal nerve (figure 1) that led to his symptoms. We then performed MVD and the symptoms fully resolved after the surgery (figure 2).
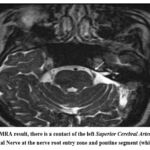 |
Figure 1: MRA result, there is a contact of the left Superior Cerebral Artery with the Trigeminal Nerve at the nerve root entry zone and pontine segment (white arrow). |
 |
Figure 2: Microvascular Decompression Procedure. The superior cerebellar artery was found to be in contact with the trigeminal nerve on superior-lateral projection. |
On the second month of post-operative follow-up, he complained about progressive headaches with memory disturbance. This complaint starts about 1 month after the surgery. Further evaluation using a head computed tomography (CT) scan revealed acute hydrocephalus (Figure 3). Ventriculoperitoneal (VP) shunt was performed using medium opening pressure. Immediately after the surgery, the patient’s complaints were resolved and he was discharged on the third postoperative day without any morbidity.
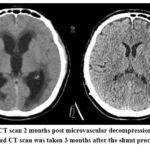 |
Figure 3: Head CT scan 2 months post microvascular decompression surgery (Left). |
Discussion
Trigeminal neuralgia is an idiopathic pathological condition that is caused by compression of the fifth cranial nerve’s root entry zone. This condition is defined by repeated stabbing pain on the trigeminal nerve branch. MVD is a well-established surgical technique to treat trigeminal neuralgia with minimal complications.
Several complications were mentioned in posterior fossa surgery including cerebellar hematoma, infections, CSF leakage, cranial nerve injury, and hydrocephalus.2,4 Among all the complications mentioned above, hydrocephalus is one of the rarest complications that occur with posterior fossa surgery.2,5,6 Hydrocephalus related to posterior fossa surgery was reported either as obstructive or communicating. Certain etiology mentioned as the causes of hydrocephalus are cerebellar hematoma, cerebellar swelling, and blood dispersion in subarachnoidal space.2,6
Microvascular decompression (MVD) is one of the well-established treatment options for trigeminal neuralgia that may include posterior fossa surgery. However, due to its surgical nuances with minimal disruption of the surrounding neurovascular anatomy on the posterior fossa compartment, this procedure is thought to differ from conventional posterior fossa surgeries.2 This concept is also supported by the fact that MVD had a lower rate of complications and morbidity compared to posterior fossa surgery. Generally, in posterior fossa surgery, hydrocephalus may occur due to cerebellar hemorrhage, cerebellar edema due to surgical manipulation, blood dispersion on a subarachnoidal layer, cerebellar ischemia, and infections.1,2,7
Two studies from Hanakita3 and Barker8, reported a total of 2 cases of acute hydrocephalus from each study that related to cerebellar swelling and cerebellar hematoma. Slow-chronic type of postoperative hydrocephalus with MVD surgery may relate to the leptomeningeal inflammatory response, which may lead to a gradual rise in CSF outflow resistance. As in this case, even though there is no subarachnoid blood dispersion, cerebellar hematoma nor infection occurs. Muratorio and colleagues explained that hydrocephalus may occur due to inflammatory substances that release after the surgery leading to an increasing CSF outflow pathway.2 This mechanism is similar to experimental hydrocephalus.
There are still minimal data regarding the slow-chronic hydrocephalus. This may be explained that most studies are focusing on short-term complications of MVD. Case series by Muratorio found the incidence of postoperative hydrocephalus was 3.5% with the mean time between MVD and the development of hydrocephalus being about 3 months.2 Similar result was found in a study by Legnani and colleagues that found that hydrocephalus occurs in about 4% of craniotomy cases.7 Sinus exposure during craniotomy that lead to sinus injury increases the risk of postoperative hydrocephalus.7
Conclusion
MVD procedure is already a standard surgical procedure to treat trigeminal neuralgia. Hydrocephalus as a complication after an MVD procedure has been reported infrequently. Slow-chronic hydrocephalus can be a potential long-term complication of MVD surgery. The pathophysiology is still unclear, but surgeons and patients must be warned about this possible surgical adverse event.
Conflicts of Interest
There are no conflicts of interest
Funding Source
There is no funding source.
References
- Fessler RG, Sekhar LN, eds. Microvascular Decompression for Cranial Nerves and Brainstem Compression Syndrome. In: Atlas of Neurosurgical Techniques. 2nd ed. Thieme; 2005:655-674.
- Muratorio F, Tringali G, Levi V, Ligarotti GKI, Nazzi V, Franzini AA. Hydrocephalus: an underrated long-term complication of microvascular decompression for trigeminal neuralgia. A single institute experience. Acta Neurochir (Wien). 2016;158(11):2203-2206. doi:10.1007/S00701-016-2911-4
CrossRef - Hanakita J, Kondo A. Serious complications of microvascular decompression operations for trigeminal neuralgia and hemifacial spasm. Neurosurgery. 1988;22(2):348-352. doi:10.1227/00006123-198802000-00012
CrossRef - Dubey A, Sung WS, Shaya M, et al. Complications of posterior cranial fossa surgery–an institutional experience of 500 patients. Surg Neurol. 2009;72(4):369-375. doi:10.1016/J.SURNEU.2009.04.001
CrossRef - Hammett T, Teale A, Kumaria A, Basu S. Hydrocephalus Following Microvascuar Decompression – an Under-Recognised Complication. In: CNS Annual Meeting. ; 2016:48.
- Fayed ZY, Afify H. Long ‑ term follow ‑ up of microvascular decompression for management of trigeminal neuralgia. Egypt J Neurosurg. 2022;37(30). doi:10.1186/s41984-022-00171-z
CrossRef - Legnani FG, Saladino A, Casali C, et al. Craniotomy vs. craniectomy for posterior fossa tumors: a prospective study to evaluate complications after surgery. Acta Neurochir (Wien). 2013;155(12):2281-2286. doi:10.1007/S00701-013-1882-Y
CrossRef - Barker FG, Jannetta PJ, Bissonette DJ, Larkins M V., Jho HD. The long-term outcome of microvascular decompression for trigeminal neuralgia. N Engl J Med. 1996;334(17):1077-1084. doi:10.1056/NEJM199604253341701
CrossRef

