
Manuscript accepted on :11-08-2023
Published online on: 25-09-2023
Plagiarism Check: Yes
Reviewed by: Dr. Khadiga Ibrahim and Dr. Monu Kumar Shukla
Second Review by: Dr Supratim Datta
Final Approval by: Dr. Ian James Martin
Stefano Mastrangelo , Giorgio Attina’ and Antonio Ruggiero
, Giorgio Attina’ and Antonio Ruggiero
Pediatric Oncology Unit, Fondazione Policlinico Universitario A.Gemelli IRCCS, Universita’ Cattolica Sacro Cuore, Rome, Italy.
Corresponding Author E-mail: antonio.ruggiero@unicatt.it
DOI : https://dx.doi.org/10.13005/bpj/2713
Abstract
Some multithyrosine kinase inhibitors have been reported to cause changes in thyroid function. For the management of sunitinib-induced hypothyroidism, an evaluation of thyroid hormone and antibody profile is recommended before starting treatment with tyrosine kinase inhibitors. Patients with pre-existing thyroid dysfunction should undergo dose adjustment of L-thyroxine during treatment with tyrosine kinase inhibitors. Thyroid dysfunction is not a reason to discontinue or reduce the dosage of sunitinib. Their occurrence appears to correlate with increased antitumour efficacy of the inhibitor. There are currently no guidelines for monitoring thyroid activity during treatment with TKIs, and the time interval at which TSH should be periodically measured has not yet been determined. A reasonable approach is to monitor thyroid function, both before and during 2-4 weeks after the end of therapy. A comprehensive analysis of adverse events associated with the use of these inhibitors could help clinical monitoring of patients along with the adoption of appropriate management approaches.
Keywords
Thyroid Dysfunction; Tyrosine Kinase Inhibitors; Sunitinib
Download this article as:| Copy the following to cite this article: Mastrangelo S, Attina G, Ruggiero A. Tyrosine Kinase Inhibitors and Thyroid Toxicity. Biomed Pharmacol J 2023;16(3). |
| Copy the following to cite this URL: Mastrangelo S, Attina G, Ruggiero A. Tyrosine Kinase Inhibitors and Thyroid Toxicity. Biomed Pharmacol J 2023;16(3). Available from: https://bit.ly/46737w6 |
Introduction
In recent years, the widespread use of tyrosine kinase inhibitors (TKIs) in oncology, either in combination with chemotherapy or radiotherapy or as a single agent, has led to a growing interest in the effects determined by these drugs on the endocrine system, on thyroid function. Dysregulation of tyrosine kinase receptor activity is a crucial event that determines the ‘escape’ of the tumour cell from the regulation of physiological growth mechanisms, leading to tumor genesis. The receptors ‘targeted’ by TKIs are implicated in cell survival, proliferation, invasiveness, and tumour angiogenesis. The tolerability profile of each molecule is variable and in comparison, to conventional cytotoxic agents, TKIs are associated with a lower degree of toxicity. Several tyrosine kinase inhibitor drugs have been approved and are used in therapy 1,2. As a result, the use of these drugs has increased and new side effects associated with them have been highlighted. TKIs induce thyroid dysfunction and manifest in various forms such as hypothyroidism, thyroiditis, and hyperthyroidism. The most common is hypothyroidism, which can be diagnosed or remains at subclinical levels 3-5. Sunitinib is particularly associated with these side effects that are related to thyroid function. Retrospective studies indicate that with sunitinib use there is a 53-85% risk of hypothyroidism while prospective data report an incidence of hypothyroidism of 36-71%. Other TKIs such as sorafenib, imatinib, and vandetanib induce thyroid dysfunction, though to a lesser extent than sunitinib 6-8.
TKIs and thyroid dysfunction
The main drugs believed to cause thyroid dysfunction are described and their incidences are analysed.
Sunitinib
The use of sunitinib has been associated with the highest risk of developing hypothyroidism 9. This drug is an orally administered TKI and has multitarget activity involving the platelet-derived growth factor receptor (PDGFR), vascular endothelial growth factor receptor (VEGFR), kit, and RET (Table 1)[10,11].
Table 1: Examples of TKIs and their targets
|
Target |
Drug |
Approved indications |
|
BCR-ABL |
Imatinib Dasatinib Nilotinib |
Chronic myeloid leukaemia Philadelphia chromosome positive acute lymphoid leukaemia |
|
KIT |
Imatinib Sunitinib |
Gastrointestinal stromal tumour |
|
PDGFR α/β |
Imatinib |
Chronic myelomonocyticleukaemia (with TEL-PDGFRβ fusion) Hypereosinophilic syndrome (with PDGFRβ fusion) Dermatofibrosarcoma protuberans |
|
HER 2 |
Lapatinib |
Her2+ breast cancer |
|
EGFR |
Gefitinib |
Lung adenocarcinoma (with EGFR mutation) |
|
VEGFR |
Sorafenib Sunitinib |
Kidney cancer Hepatocellular carcinoma (sorafenib only) |
Sunitinib treatment resulted in thyroid dysfunction after two cases experienced symptoms such as marked asthenia, confusion, decreased cold/heat tolerance, palpitations, decreased heat tolerance, and neck pain after sunitinib treatment. Both patients had subnormal serum thyroid-stimulating hormone (TSH) levels and received thyroid hormone replacement therapy, which resulted in resolution of symptoms and physiologic levels of TSH 12,13.
These clinical observations prompted prospective studies to identify possible associations between sunitinib and the development of thyroid dysfunction. Thus, data from 42 imatinib-resistant GIST gastrointestinal stromal tumour patients who had been treated with for at least three cycles of sunitinib were analysed. These patients had normal serum TSH levels and were not taking thyroid medications or drugs that may cause thyroid dysfunction. The data collected showed abnormal serum TSH concentrations in 26 patients (62%); persistent primary hypothyroidism was registered in 15 patients (36%); 4 patients (10%) developed isolated TSH suppression; in 7 patients (17%) a transient TSH increase was observed; biochemical data showed no signs of autoimmune thyroid disease in any patient 12.
There are many other studies showing a close association between sunitinib treatment and thyroid dysfunction. The conclusions to be drawn from these are: a) The longer the sunitinib treatment, the higher the risk of hypothyroidism. b) After discontinuing sunitinib, serum TSH levels return to normal over approximately 60 days 6. The average time to develop thyroid dysfunction is about 4 weeks. Patients who did not develop hypothyroidism in the first cycle did not develop hypothyroidism in the more advanced stages of treatment. 14,15.
Sorafenib
Sorafenib is an orally administered TKI with inhibitory activity on several kinases such as BRAF, VEGFR, RET 16,17. Because of the increased risk of thyroid dysfunction in patients receiving sunitinib, several studies have been conducted to investigate the association of other TKIs with this type of dysfunction 18,19.
These include a retrospective study evaluating thyroid function testing in patients receiving sorafenib for metastatic renal cell carcinoma (RCC). Results showed that of the 39 patients, 8 (21%) developed hypothyroidism and 7 hypothyroidism and hyperthyroidism. Clinical events due to thyroid dysfunction requiring thyroid hormone replacement therapy occurred in only 2 subjects 20. Another study involved 38 patients, with metastatic RCC treated with sorafenib 400 mg administered twice daily, in whom thyroid function was monitored over time. Thyroid hormones were assessed before starting treatment and on the first day of each treatment cycle. Of the 38 patients, 23 had normal baseline thyroid function and 15 had thyroid dysfunction. The results showed that among the 23 patients with normal basal thyroid hormones, high serum TSH was present in 7 patients (30%), and low serum TSH in 1 patient (5%). No additional treatment had to be initiated. Of the 15 patients with basal thyroid insufficiency, two patients, whose initial condition was subclinical hypothyroidism (elevated serum TSH but normal T3 and T4), subsequently showed clinical signs of hypothiroidism. Thyroid hormone therapy had to be initiated in these patients 6, 21-23.
Imatinib
Imatinib is an oral TKI that activates with RET, BCR-ABL, PDGFR, c-Fms, and c-Kit. In a study of imatinib treatment for advanced medullary thyroid cancer (MTC) in 15 patients, 10 of whom had undergone total thyroidectomy and were receiving hormone replacement therapy, 9 patients developed hypothyroidism (the 10th patient had unmonitored thyroid function). Studies have shown that a mean 210% (range 150-350%) increase in hormone replacement therapy is required to normalize TSH levels immediately after starting treatment. Normal function was maintained in patients with intact thyroid 24, 25.
Other studies have reported similar results, suggesting that the effect of imatinib on thyroid function is relevant only to patients who have undergone total thyroidectomy, as it appears that the action of imatinib does not occur in the thyroid itself 6,26. For further confirmation, a study with imatinib in patients with chronic myeloid leukemia and normal thyroid function reported no cases of thyroid changes 27.
Nilotinib
Nilotinib has received clinical approval for the treatment of Philadelphia-positive chronic myeloid leukemia form (Ph-positive CML). It belongs to the second generation of TKIs, designed on the structural analogy with imatinib but provided with enhanced efficacy on BCR-ABL inhibitory power 6,28-30.
A retrospective study evaluated the effect of nilotinib on thyroid function in Ph-positive CML patients. Of the 55 patients, 6 (11%) were taking thyroid medication prior to initiating nilotinib therapy, and 18 (33%) had previously been treated with interferon. The results showed that: 12 patients (22%) developed hypothyroidism (6 subclinical, 6 clinical); 18 subjects (33%) developed hyperthyroidism (10 subclinical, 8 clinical). In most patients treated with thyroid hormone replacement therapy prior to initiating nilotinib, it is not necessary to change the dose of thyroid hormone used, despite the risk of developing thyroid hormone abnormalities has been reported in patients previously treated with interferon: however, endpoint data not statistically significant. Four patients had thyroiditis (3 had antithyroid antibodies) and 1 patient had hyperthyroidism before hypothyroidism. In 3 of these patients, spontaneous resolution of hypothyroidism was observed while hormone replacement therapy was required in one patient. Therefore, it can be concluded that nilotinib-induced thyroid dysfunction rarely requires clinical pharmacological treatment 31.
Vandetanib
Vandetanib is administered orally and has targeted activity at EGFR, VEGFR, and RET.
In a study with vandetanib administered at a dose of 100 mg/day in subjects with advanced hereditary medullary thyroid carcinoma who had previously undergone total thyroidectomy and all were on hormone replacement therapy, there was a mean 5.1-fold increase in serum TSH, but no cases of symptomatic hypothyroidism 32–34.
Mechanisms responsible for the induction of hypothyroidism
Understanding the mechanism leading to hypothyroidism is a burning problem for scientists, they are conducting many different studies to answer this question. At present, there are no conclusive data, but various hypotheses have been proposed that need to be confirmed. Since this side effect was mainly observed with sunitinib use, many studies have focused on this TKI.
For sunitinib, multiple mechanisms appear to be involved:
Sunitinib appears to have a direct cytotoxic effect on thyroid cells, possibly by inhibiting the activity of VEGFR and/or PDGFR in thyroid follicular cells whose activity is only partially regulated by TSH 6,35,36. Experiments in rats reported that administration of VEGF inhibitors induced capillary depletion in various organs, including the thyroid gland where the greatest regression (68%) was observed. . Other interesting data show that TSH can be increased up to 19 times than the control value, while free T4 is unchanged. It should be noted that after treatment with VEGF inhibitors, capillary remodeling occurs in thyroid tissue 37.
It appears that sunitinib leads to altered thyroid activity by the inhibitory action of the thyroid peroxidase (TPO) by blocking thyroid hormone synthesis. As the thyroid has reserves of thyroid hormones, this could explain the latency period between the start of sunitinib therapy and the development of hypothyroidism. The ability of sunitinib to inhibit TPO activity has been evaluated in vitro but not in vivo 38,39.
Sunitinib can block the absorption of iodine and thereby cause transient hypothyroidism. The most widely accepted mechanism for this effect proposes that sunitinib interacts with the iodine-sodium synchronizer (NIS), whose TSH regulation occurs via cAMP, unaffected by the drug. However, Sunitib does not seem to affect NIS 6.
Finally, sunitinib does not appear to induce autoimmune thyroid disease, as may occur with interferon-α and interleukin-based therapies 6. As for sorafenib, it also inhibits VEGFR and PDGFR, thereby weakening the capillaries of thyroid tissue, but unlike sunitinib, it appears to interact with TSH-mediated regulation, because TSH is involved in RAF, which is a target of sorafenib. However, the potential effects of sunitinib on normal thyroid function have not been thoroughly investigated, nor can sorafenib have less of a thyroid effect than sunitinib 6,40.
Discussion
Over the past 50 years, cancer treatment has evolved from the use of a highly toxic drug such as nitrogen mustard (classic cytotoxic, acting on all cells and having an extremely limited margin of selectivity) until recent years when certain drugs have been introduced to have hormonal regulatory effects on tumor growth or the cell cycle control mechanism underlying malignancies 41-44. These new drugs belong to targeted molecular therapy that disrupt specific cell life signaling pathways and are more tolerable than traditional cancer drugs (Figure 1)45,46.
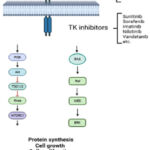 |
Figure 1: Summary of the TKI effects |
Molecularly targeted therapeutic drugs designed to act on specific cellular targets that interfere with cell growth; this leads to a decrease in nonspecific toxicity. Molecular targeted therapy indeed exhibits lower toxicity than traditional therapies, but this should not be underestimated, as it can affect different areas of the body such as the cardiovascular, skin, lungs, liver, kidneys, thyroid, gastrointestinal tract and nerves 47 -50. Side effects are usually of low intensity and are therefore more easily tolerated by patients; however, there may be degrees of toxicity that must be addressed by discontinuation of therapy or other pharmacological strategies. A distinction can also be made between targeted and untargeted side effects. Targeted toxicity is due to the primary pharmacological action of the drug (thus related to the drug’s mechanism of action) while off-target toxicity is due to a secondary pharmacological effect of the drug (which is not related to the drug’s mechanism of action)3.
The most common endocrine disturbance associated with TKI use is hypothyroidism, which may develop ex-novo or, if pre-existing, requires an adjustment in the thyroxine dose. Although TKI-induced hypothyroidism is only a manageable side effect, some results suggest a potential prognostic role in cancer treatment efficacy. For example, in a study with sunitinib or sorafenib in patients with metastatic CRC, the clinical picture of hypothyroidism was found in 21 out of 66 patients (38.1%) and was associated with a better chance of survival (16.0 ± 0.8 months versus 6.0±0.8 months, p=0.032)51. An explanation for the association between hypothyroidism and increased chances of survival after TKI treatment may be due to the inhibitory effect of hypothyroidism on tumor growth. The proposed mechanism suggests that thyroid hormone may stimulate the growth of certain types of tumors by acting directly or indirectly by regulating the expression of certain growth factors 6. Clinical data show how hypothyroidism can inhibit tumor growth: in breast cancer patients, hypothyroidism is favorably associated with a lower risk of tumor development, less aggressive tumor, and advanced age 6,52.
Since data have suggested that the presence of hypothyroidism due to TKIs is associated with improved treatment efficacy, treatment of hypothyroidism may lead to worsening clinical outcomes 53-57. Indeed, thyroid hormone replacement therapy may be permitted in patients with cancer who are active or in remission. However, elevated serum VEGF values have been identified in most hypothyroid patients receiving hormone replacement therapy 58–62. It should be noted that some studies have failed to show a life expectancy benefit related to the development of hypothyroidism 6,63-65.
There are currently no recommendations for monitoring thyroid activity during treatment with TKIs and the interval for periodic measurement of TSH levels has not been determined. There are various suggestions, such as measuring thyroid function on the first day of each treatment cycle. However, it is certainly necessary to monitor thyroid function even after the end of TKI therapy to check its recovery 66-74. A reasonable approach is to monitor thyroid function, both before and for 2-4 weeks after the end of treatment. If elevated TSH values are found shortly after stopping treatment, hypothyroidism is likely to persist and should be treated with thyroxine, as it may worsen in subsequent cycles of treatment. However, at present, further evaluation of the progression of thyroid function in TKI-treated patients is still needed to determine appropriate therapeutic measures 73-76.
Conclusions
The use of molecularly targeted drugs in therapy has resulted in improvements in the fight against cancer, as the therapeutic effect is more selective and the incidence of adverse events and toxicity is smaller than in the past. Furthermore, these effects are usually dose dependent and reversible. However, early symptoms of toxicity due to molecularly targeted therapies are often unrecognized by patients and not reported to oncologists. These first symptoms can develop into situations that are very dangerous and risky for the patient’s health, and in some (rare) cases even lead to the death of the patient.
Therefore, patients should be monitored by the treating physician and properly informed about possible toxic effects so that they can be treated consciously and can be reported to the physician during the clinical examination.
Acknowledgments
The authors thank “Fondazione per l’Oncologia Pediatrica ONLUS” for their dedicated patient care and scientific support.
Conflict of Interest
The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Funding Sources
The authors received no specific funding for this work.
References
- Arora A, Scholar EM. Role of tyrosine kinase inhibitors in cancer therapy. J Pharmacol Exp Ther. 2005;315(3):971-9
CrossRef - Baldo BA. Adverse events to monoclonal antibodies used for cancer therapy: Focus on hypersensitivity responses. Oncoimmunology. 2013;2(10):e26333.
CrossRef - Shah DR, Shah RR, Morganroth J. Tyrosine kinase inhibitors: their on-target toxicities as potential indicators of efficacy. Drug Saf. 2013;36(6):413-26.
CrossRef - Chhabra N, Kennedy J. A Review of Cancer Immunotherapy Toxicity II: Adoptive Cellular Therapies, Kinase Inhibitors, Monoclonal Antibodies, and Oncolytic Viruses. J Med Toxicol. 2022;18(1):43-55.
CrossRef - Ruggiero A, Rizzo D, Trombatore G, Maurizi P, Riccardi R. The ability of mannitol to decrease cisplatin-induced nephrotoxicity in children: real or not? Cancer Chemother Pharmacol. 2016;77(1):19-26.
CrossRef - Brown RL. Tyrosine kinase inhibitor-induced hypothyroidism: incidence, etiology, and management. Target Oncol. 2011;6(4):217-26.
CrossRef - Fallahi P, Ferrari SM, Vita R, et al. Thyroid dysfunctions induced by tyrosine kinase inhibitors. Expert Opin Drug Saf. 2014;13(6):723-33.
CrossRef - De Leo S, Trevisan M, Moneta C, Colombo C. Endocrine-related adverse conditions induced by tyrosine kinase inhibitors. Ann Endocrinol (Paris). 2023;84(3):374-381.
CrossRef - Wei G, Zhang CX, Jing Y, Chen X, Song HD, Yang L. The influence of sunitinib and sorafenib, two tyrosine kinase inhibitors, on development and thyroid system in zebrafish larvae. Chemosphere. 2022;308(Pt 2):136354.
CrossRef - Gutierrez C, McEvoy C, Munshi L, Stephens RS, Detsky ME, Nates JL, Pastores SM. Critical Care Management of Toxicities Associated With Targeted Agents and Immunotherapies for Cancer. Crit Care Med. 2020;48(1):10-21.
CrossRef - Boskabadi SJ, Dashti A, Karevan S, Kargar-Soleimanabad S, Salehifar E. Clinical uses and safety concerns of tyrosine kinase inhibitors with a focus on novel drugs: A narrative review. J Oncol Pharm Pract. 2023 May 12:10781552231174790. doi:10.1177/10781552231174790
CrossRef - Desai J, Yassa L, Marqusee E, et al. Hypothyroidism after sunitinib treatment for patients with gastrointestinal stromal tumors. Ann Intern Med. 2006;145(9):660-4
CrossRef - Pani F, Atzori F, Baghino G, Boi F, Tanca L, Ionta MT, Mariotti S. Thyroid Dysfunction in Patients with Metastatic Carcinoma Treated with Sunitinib: Is Thyroid Autoimmunity Involved? Thyroid. 2015;25(11):1255-61.
CrossRef - Sabanathan D, Zhang A, Fox P, et al. Dose individualization of sunitinib in metastatic renal cell cancer: toxicity-adjusted dose or therapeutic drug monitoring. Cancer Chemother Pharmacol. 2017;80(2):385-393.
CrossRef - Ravaud A, Bello CL. Exposure-response relationships in patients with metastatic renal cell carcinoma receiving sunitinib: maintaining optimum efficacy in clinical practice. Anticancer Drugs. 2011;22(5):377-83.
CrossRef - Acharya B, Frett B. An updated patent review of rearranged during transfection (RET) kinase inhibitors (2016-present). Expert Opin Ther Pat. 2022;32(10):1067-1077.
CrossRef - Li AY, McCusker MG, Russo A, et al. RET fusions in solid tumors. Cancer Treat Rev. 2019;81:101911.
CrossRef - Walko CM, Aubert RE, La-Beck NM, et al. Pharmacoepidemiology of Clinically Relevant Hypothyroidism and Hypertension from Sunitinib and Sorafenib. Oncologist. 2017;22(2):208-212.
CrossRef - Clemons J, Gao D, Naam M, Breaker K, Garfield D, Flaig TW. Thyroid dysfunction in patients treated with sunitinib or sorafenib. Clin Genitourin Cancer. 2012;10(4):225-31.
CrossRef - Tamaskar I, Bukowski R, Elson P, et al. Thyroid function test abnormalities in patients with metastatic renal cell carcinoma treated with sorafenib. Ann Oncol. 2008;19(2):265-8.
CrossRef - Shu M, Zai X, Zhang B, Wang R, Lin Z. Hypothyroidism Side Effect in Patients Treated with Sunitinib or Sorafenib: Clinical and Structural Analyses. PLoS One. 2016;11(1):e0147048.
CrossRef - Demirtas L, Gürbüzel M, Tahirler H, Akbas EM, Karatas O, Arslan YK. The effects of sorafenib in healthy and cisplatin-treated rats. Adv Clin Exp Med. 2023;32(4):449-456.
CrossRef - Shao YY, Cheng AL, Hsu CH. An Underdiagnosed Hypothyroidism and Its Clinical Significance in Patients with Advanced Hepatocellular Carcinoma. Oncologist. 2021;26(5):422-426.
CrossRef - de Groot JW, Zonnenberg BA, van Ufford-Mannesse PQ, et al. A phase II trial of imatinib therapy for metastatic medullary thyroid carcinoma. J Clin Endocrinol Metab. 2007;92(9):3466-9
CrossRef - Mehra N, Varmeziar A, Chen X, Kronick O, Fisher R, Kota V, Mitchell CS. Cross-Domain Text Mining to Predict Adverse Events from Tyrosine Kinase Inhibitors for Chronic Myeloid Leukemia. Cancers (Basel). 2022;14(19):4686.
CrossRef - Eroukhmanoff J, Castinetti F, Penel N, Salas S. Auto-immune thyroid dysfunction induced by tyrosine kinase inhibitors in a patient with recurrent chordoma. BMC Cancer. 2016;16(1):679.
CrossRef - Dora JM, Leie MA, Netto B, Fogliatto LM, Silla L, Torres F, Maia AL. Lack of imatinib-induced thyroid dysfunction in a cohort of non-thyroidectomized patients. Eur J Endocrinol. 2008;158(5):771-2
CrossRef - Bakerywala S, Schwarcz MD, Goldberg MD, Valiquette G, Weiss IA. Nilotinib-Associated Destructive Thyroiditis. Case Rep Endocrinol. 2015;2015:736092
CrossRef - Elnair R, Galal A. Finding the right BCR-ABL1 tyrosine kinase inhibitor: a case report of successful treatment of a patient with chronic myeloid leukemia and a V299L mutation using nilotinib. BMC Cancer. 2018;18(1):1097.
CrossRef - Yoshizato T, Nannya Y, Yoshiki Y, Nakamura F, Imai Y, Ichikawa M, Kurokawa M. Nilotinib-induced hypothyroidism in a patient with chronic myeloid leukemia. Int J Hematol. 2011;93(3):400-402.
CrossRef - Kim TD, Schwarz M, Nogai H, et al. Thyroid dysfunction caused by second-generation tyrosine kinase inhibitors in Philadelphia chromosome-positive chronic myeloid leukemia. Thyroid. 2010;20(11):1209-14
CrossRef - Robinson BG, Paz-Ares L, Krebs A, Vasselli J, Haddad R. Vandetanib (100 mg) in patients with locally advanced or metastatic hereditary medullary thyroid cancer. J Clin Endocrinol Metab. 2010;95(6):2664-71.
CrossRef - Santoni M, Guerra F, Conti A, et al. Incidence and risk of cardiotoxicity in cancer patients treated with targeted therapies. Cancer Treat Rev. 2017;59:123-131.
CrossRef - Brose MS, Bible KC, Chow LQM, et al. Management of treatment-related toxicities in advanced medullary thyroid cancer. Cancer Treat Rev. 2018;66:64-73.
CrossRef - Werbrouck E, Bastin J, Lambrechts D, et al. ABCG2 polymorphism rs2231142 and hypothyroidism in metastatic renal cell carcinoma patients treated with sunitinib. Acta Clin Belg. 2019;74(3):180-188.
CrossRef - Rizza L, Sbardella E, Gianfrilli D, et al. Thyroid profile during the alternative Sunitinib dosing 2/1 schedule in metastatic renal cell carcinoma. Endocrine. 2020;67(3):597-604.
CrossRef - Kamba T, Tam BY, Hashizume H, et al. VEGF-dependent plasticity of fenestrated capillaries in the normal adult microvasculature. Am J Physiol Heart Circ Physiol. 2006;290(2):H560-76
CrossRef - Wong E, Rosen LS, Mulay M, et al. Sunitinib induces hypothyroidism in advanced cancer patients and may inhibit thyroid peroxidase activity. Thyroid. 2007;17(4):351-5
CrossRef - Buda-Nowak A, Kucharz J, Dumnicka P, Kuzniewski M, Herman RM, Zygulska AL, Kusnierz-Cabala B. Sunitinib-induced hypothyroidism predicts progression-free survival in metastatic renal cell carcinoma patients. Med Oncol. 2017;34(4):68.
CrossRef - Bourlon MT, Gao D, Trigero S, Clemons JE, Breaker K, Lam ET, Flaig TW. Clinical significance of sunitinib-associated macrocytosis in metastatic renal cell carcinoma. Cancer Med. 2016;5(12):3386-3393.
CrossRef - Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8(1):262
CrossRef - Falsini B, Ziccardi L, Lazzareschi I, et al. Longitudinal assessment of childhood optic gliomas: relationship between flicker visual evoked potentials and magnetic resonance imaging findings. J Neurooncol. 2008; 88: 87-96.
CrossRef - Wilkes GM. Targeted Therapy: Attacking Cancer with Molecular and Immunological Targeted Agents. Asia Pac J Oncol Nurs. 2018;5(2):137-155.
CrossRef - Riccardi A, Mazzarella G, Cefalo G, et al. Pharmacokinetics of Temozolomide given three times a day in paediatric and adult patients. Cancer Chemother Pharmacol. 2003; 52: 459-464
CrossRef - Wujcik D. Science and mechanism of action of targeted therapies in cancer treatment. Semin Oncol Nurs. 2014;30(3):139-46
CrossRef - Chiaretti A, Ruggiero A, Barbi E, et al. Comparison of propofol versus propofol-ketamine combination in paediatric oncologic procedures performed by non-anesthesiologists. Pediatr Blood Cancer. 2011;57(7):1163-1167
CrossRef - Advani D, Sharma S, Kumari S, Ambasta RK, Kumar P. Precision Oncology, Signaling, and Anticancer Agents in Cancer Therapeutics. Anticancer Agents Med Chem. 2022;22(3):433-468.
CrossRef - Ruggiero A, Rizzo D, Mastrangelo S, Battaglia D, Attinà G, Riccardi R. Interactions between antiepileptic and chemotherapeutic drugs in children with brain tumors: is it time to change treatment? Pediatr Blood Cancer. 2010;54(2):193-198
CrossRef - Huang M, Geng MY, Ding J. Antitumor pharmacological research in the era of personalized medicine. Acta Pharmacol Sin. 2022;43(12):3015-3020.
CrossRef - Lazzareschi I, Ruggiero A, Riccardi R, Attinà G, Colosimo C, Lasorella A. Hypersensitivity reactions to carboplatin in children. J Neurooncol. 2002; 58:33-37
CrossRef - Riesenbeck LM, Bierer S, Hoffmeister I, et al. Hypothyroidism correlates with a better prognosis in metastatic renal cancer patients treated with sorafenib or sunitinib. World J Urol. 2011;29(6):807-13
CrossRef - Vasileiadis T, Chrisofos M, Safioleas M, Kontzoglou K, Papazisis K, Sdrolia A. Ιmpact of sunitinib-induced hypothyroidism on survival of patients with metastatic renal cancer. BMC Cancer. 2019;19(1):407.
CrossRef - Wu J, Huang H. Acquired Hypothyroidism in Patients with Metastatic Renal Cell Carcinoma Treated with Tyrosine Kinase Inhibitors. Drug Des Devel Ther. 2020;14:3977-3982.
CrossRef - Ruggiero A, Rizzo D, Catalano M, Coccia P, Triarico S, Attiná G. Acute chemotherapy-induced nausea and vomiting in children with cancer: Still waiting for a common consensus on treatment. J Int Med Res. 2018;46(6):2149-2156.
CrossRef - Bozkurt O, Karaca H, Hacıbekiroglu I, et al. Is sunitinib-induced hypothyroidism a predictive clinical marker for better response in metastatic renal cell carcinoma patients? J Chemother. 2016;28(3):230-4.
CrossRef - Falsini B, Chiaretti A, Barone G, et al. Topical nerve growth factor as a visual rescue strategy in paediatric optic gliomas: a pilot study including electrophysiology. Neurorehabil Neural Repair. 2011; 25: 512-520.
CrossRef - Badran A, Elshenawy MA, Shahin A, Aljubran A, Alzahrani A, Eldali A, Bazarbashi S. Efficacy and Prognostic Factors of Sunitinib as First-Line Therapy for Patients With Metastatic Renal Cell Carcinoma in an Arab Population. JCO Glob Oncol. 2020;6:19-26.
CrossRef - Dedecjus M, Kołomecki K, Brzeziński J, Adamczewski Z, Tazbir J, Lewiński A. Influence of L-thyroxine administration on poor-platelet plasma VEGF concentrations in patients with induced short-term hypothyroidism, monitored for thyroid carcinoma. Endocr J. 2007;54(1):63-9
CrossRef - Ruggiero A, Maurizi P, Larocca LM, Arlotta A, Riccardi R. Childhood CD4+/CD56+ hematodermic neoplasm: case report and review of the literature. Haematologica. 2006;91(12 Suppl):ECR48.
CrossRef - Huang M, Shen A, Ding J, Geng M. Molecularly targeted cancer therapy: some lessons from the past decade. Trends Pharmacol Sci. 2014;35(1):41-50.
CrossRef - Trisciuzzi MT, Riccardi R, Piccardi M, et al. A fast visual evoked potential method for functional assessment and follow-up of childhood optic gliomas. Clin Neurophysiol. 2004; 115: 217-226
CrossRef - Singha H, Chakrabarty SK, Sherpa PL, Saha S. A Study to Assess Tyrosine Kinase Inhibitors Induced Thyroid Dysfunction in Newly Diagnosed Chronic Myeloid Leukemia Patients. J Assoc Physicians India. 2023;71(1):1.
- Cai W, Zhong H, Kong W, et al. Significance of preoperative prognostic nutrition index as prognostic predictors in patients with metastatic renal cell carcinoma with tyrosine kinase inhibitors as first-line target therapy. Int Urol Nephrol. 2017;49(11):1955-1963.
CrossRef - Abd Ghafar NK, Alip A, Ong TA, Yap NY, Saad M. Efficacy, safety, and prognostic indicators of first-line sunitinib in patients with metastatic renal cell carcinoma: A single center experience. J Cancer Res Ther. 2018;14(6):1303-1311.
CrossRef - Fetoni AR, Ruggiero A, Lucidi D, De Corso E, Sergi B, Conti G, Paludetti G. Audiological Monitoring in Children Treated with Platinum Chemotherapy. Audiol Neurootol. 2016;21(4):203-211.
CrossRef - Heraudet L, Domblides C, Daste A, Lefort F, Bernhard JC, Ravaud A, Gross-Goupil M. Safety of sunitinib in patients with renal cell carcinoma following nephrectomy. Expert Opin Drug Saf. 2020;19(7):799-806.
CrossRef - Demlová R, Turjap M, Peš O, Kostolanská K, Juřica J. Therapeutic Drug Monitoring of Sunitinib in Gastrointestinal Stromal Tumors and Metastatic Renal Cell Carcinoma in Adults-A Review. Ther Drug Monit. 2020;42(1):20-32.
CrossRef - Perrone MG, Ruggiero A, Centonze A, Carrieri A, Ferorelli S, Scilimati A. Diffuse Intrinsic Pontine Glioma (DIPG): Breakthrough and Clinical Perspective. Curr Med Chem. 2021;28(17):3287-3317.
CrossRef - Westerdijk K, Krens SD, van der Graaf WTA, et al. The relationship between sunitinib exposure and both efficacy and toxicity in real-world patients with renal cell carcinoma and gastrointestinal stromal tumour. Br J Clin Pharmacol. 2021;87(2):326-335.
CrossRef - Ruggiero A, Barone G, Liotti L, Chiaretti A, Lazzareschi I, Riccardi R. Safety and efficacy of fentanyl administered by patient controlled analgesia in children with cancer pain. Support Care Cancer. 2007;15(5):569-73. doi: 10.1007/s00520-006-0193-8.
CrossRef - Cabel L, Blanchet B, Thomas-Schoemann A, et al. Drug monitoring of sunitinib in patients with advanced solid tumors: a monocentric observational French study. Fundam Clin Pharmacol. 2018;32(1):98-107.
CrossRef - Posteraro B, Bruno S, Boccia S, et al. Candida parapsilosis bloodstream infection in paediatric oncology patients: results of an epidemiologic investigation. Infect Control Hosp Epidemiol. 2004;25(8):641-5.
CrossRef - Hu X, Khatri U, Shen T, Wu J. Progress and challenges in RET-targeted cancer therapy. Front Med. 2023;17(2):207-219. doi: 10.1007/s11684-023-0985-y.
CrossRef - Diekstra MH, Fritsch A, Kanefendt F, et al. Population Modeling Integrating Pharmacokinetics, Pharmacodynamics, Pharmacogenetics, and Clinical Outcome in Patients With Sunitinib-Treated Cancer. CPT Pharmacometrics Syst Pharmacol. 2017;6(9):604-613.
CrossRef - Illouz F, Braun D, Briet C, et al. Endocrine side-effects of anti-cancer drugs: thyroid effects of tyrosine kinase inhibitors. Eur J Endocrinol. 2014;171: R91-9.
CrossRef - Acitelli E, Maiorca C, Grani G, Maranghi M. Metabolic adverse events of multitarget kinase inhibitors: a systematic review. Endocrine. 2023;81(1):16-29. doi: 10.1007/s12020-023-03362-2.
CrossRef

