
Manuscript accepted on :11-02-2023
Published online on: 01-08-2023
Plagiarism Check: Yes
Reviewed by: Dr. Ameer Ali Shakr Hadi
Second Review by: Dr. Nataliya Kitsera
Final Approval by: Dr. Ayush Dogra
Durairaj Natesan1 , Vidhya Venugopal1, Maheshkumar kuppusamy2, P.Saiprasad3 and A.Subhashini4
, Vidhya Venugopal1, Maheshkumar kuppusamy2, P.Saiprasad3 and A.Subhashini4
1Department of Environmental Health Engineering, Sri Ramachandra Institute for Higher Education and Research (SRIHER), Chennai, Tamilnadu, India.
2Government Yoga and Naturopathy Medical College and Hospital, Chennai, Tamilnadu, India.
3Tamilnadu Pollution control Board, Chennai, Tamilnadu, india.
4Department of Physiology, Sri Ramachandra Institute for Higher Education and Research (SRIHER), Chennai, Tamilnadu, India.
Corresponding Author E-mail:durai@ehe.org.in
DOI : https://dx.doi.org/10.13005/bpj/2728
Abstract
Background: Women in developing countries are exposed to household air pollution from traditional cook a stove, which causes a huge burden of morbidity. This study aims to examine the impact of cooking fuel use on lung function changes among women in rural Tamil Nadu, India. Methods: Between 2012 and 2014, 565 adult women (237 using solid biomass fuel and 328 using clean fuel for cooking) participated in this cross-sectional study. Basic demographic and socioeconomic characteristics and exposure related information such as fuel type, kitchen type, type of house, and other potential sources of particulates inside the house, such as cigarettes; incense, and mosquito coils, were collected using questionnaires. A pulmonary function test assessment was done for all participants using a KOKO spirometer following the standard protocols. Results: Pulmonary function was significantly (p < 0.05) lower in rural women using biomass fuel for cooking. Women in the biomass group had FVC 2.45 (0.58), FEV1 1.99 (0.49), and PEFR 5.31 (1.54), while women in the LPG group had FVC 2.63 (0.48), FEV1 2.19 (0.42), and PEFR 5.81 (1.38). Conclusion: This cross-sectional study found that the reduction in the pulmonary function parameters was considerably higher among women using biomass for cooking compared to women using liquefied petroleum gas for cooking in rural Tamil Nadu. Objective measurements by spirometry from this study can help physicians and health policy makers develop measures for better prevention and management of respiratory diseases among rural women in Tamil Nadu, southern India.
Keywords
Biomass; Cooking fuel; pulmonary function; rural Tamil Nadu
Download this article as:| Copy the following to cite this article: Natesan D, Venugopal V, Kuppusamy M, Saiprasad P, Subhashini A. Lung Function Impairment Among Women Cooking with Biomass Fuels Compared to LPG Fuel in Rural Tamil Nadu. Biomed Pharmacol J 2023;16(3). |
| Copy the following to cite this URL: Natesan D, Venugopal V, Kuppusamy M, Saiprasad P, Subhashini A. Lung Function Impairment Among Women Cooking with Biomass Fuels Compared to LPG Fuel in Rural Tamil Nadu. Biomed Pharmacol J 2023;16(3). Available from: https://bit.ly/47kEnkZ |
Introduction
Air pollution is commonly perceived as an urban problem that is associated with motor vehicles and industries; indoor air pollution caused by the combustion of biomass fuels for household cooking virtually exposes about half of the world’s population in rural areas of developing countries to some of the highest levels of air pollution. Household air pollution (HAP) is generated by the use of incompetent and polluting fuels and technologies in and around the home and contains a range of health-damaging pollutants, including small particles that infiltrate deep into the lungs and enter the bloodstream. Many people are changing to LPG throughout the world. Unfortunately, in low and middle income countries, mainly in rural areas, many households still use solid fuel for cooking, heating, and burning 1. Household air pollution (HAP), particularly particulate air pollution, has been linked to an increase in cardiovascular and respiratory illnesses in several countries, including India 2,3. The health effects vary greatly from person to person, and women who cook using biomass fuel in poor ventilation conditions have higher exposures, which put them at high-risk 6. Most of the respiratory problems that have been linked with exposure to (HAP are acute respiratory infections, chronic bronchitis, asthma, tuberculosis, lung cancer, impaired lung function, and chronic obstructive pulmonary disease 7-10. Several epidemiological studies report that higher exposure to increased levels of HAP reduces lung function 11,12. One of the most important risk factors for decreased pulmonary function is exposure to HAP from biomass cooking smoke, ETS, the burning of incense and mosquito coils, and poor housing quality 13,14. Previous studies have also reported that there is a reduction in lung function in women who are exposed to biomass fuels; especially wood 15. Although, in a study conducted by AIIMS (India) in New Delhi, biomass fumes were found to have no significant effect on pulmonary function, due to good ventilation in the kitchens 16. Indian women spend more than 4 hours/day in cooking and related work, and are thus exposed to high levels of emissions from the burning of biomass cooking fuels. As a result of their relatively long exposure to emissions from cooking fuels, women and young children who stay at home are the most affected population. In developing countries, a woman begins cooking at the age of 15. She spends about 4-6 hours per day in the kitchen and is therefore exposed to the cooking fuel smoke for approximately 30–40 years during her entire lifetime 17. Although there are several studies across the world on the effect of cooking fuel on lung functions, very few studies have been conducted on rural women in Tamil Nadu. This study is focused mainly on examining objectively, the impact of cooking biomass fuel usage on lung function among women in rural areas of Tamil Nadu using spirometry.
Materials and methods
Study design and participants
This is a cross-sectional study that was conducted on adult women in rural areas of Tiruvallur and Kanchipuram districts of Tamil Nadu. Participants were selected based on the inclusion criteria: age ranging from 18–60 years, residing in the same locality for at least 10 years. Smokers as well as persons with conditions such as a history of tuberculosis (TB), pregnancy, or malignancy were excluded from the study. Institutional Ethical Committee (IEC –NI / 13 / FEB / 32 / 16) approval was obtained from the host institution, and written informed consent was obtained from all the participants.
Outcome measurements
Each participant was given a validated exposure questionnaire in order to collect information on household level parameters such as fuel type, kitchen, and house, as well as other potential sources of particulates inside the house such as smoke from cigarettes, incense, and mosquito coils. The spirometry checklist was administered to the participant, and if the participant was found to be eligible, a KOKO spirometer was used (ATS guidelines, Miller et al., 2005). Calibration of the flow spirometer (KOKO) was done using a 3-litre calibration syringe every morning before starting in the field.
Pulmonary function test (PFT)
The spirometry procedure was explained to the participant in detail, and a demonstration was given, following which the participant’s height and weight were measured using a stadiometer and weighing balance, respectively. The test was performed with the participant in a standing position. The participant was instructed to start the procedure, and was continuously encouraged and motivated to do better. The PFT for all the participants was performed by the same person to avoid inter-observer variability. Forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), and peak expiratory flow rate (PEFR) values were recorded. A complete flow volume loop was obtained from the spirometer (Figure: 1). The procedure was repeated a minimum of three times and no more than eight times to obtain three acceptable and reproducible records. The record with the largest FVC, FEV1, FEV1/FVC, and PEFR was selected, and its data was checked and entered in Microsoft Excel and stored on a separate server 18.
Statistical analysis
The data was analysed using the R software (version 4.2.0) Two-tailed Student’s t-tests were used to compare the mean difference. A p-value of 0.05 was considered significant for all analyses.
Results
A total of 565 women participated, of whom 237 rural women who use biomass for cooking and 328 rural women who use LPG for cooking performed acceptable PFT testing. General characteristics of the study participants are presented in the table and figure: 1. The mean age of the biomass group is 40.83 years and 40.50 years for the LPG group. Among all the biomass group participants, 32 (14% of them) were underweight, 150 (63% of them) were of normal weight, 45 (19%) were overweight, and 10% were obese; among the LPG group participants, 34 (10%) were underweight, 156 (48% were of normal weight), 99 (30%) were overweight, and 39 (12%) were obese. In the biomass group, 36 (15%) were illiterate, 53 (23%) had finished primary or middle school, 131 (55%) had finished higher or higher education, and 17 (7% had finished graduate or higher education), whereas in the LPG group, 38 (12%) were illiterate, 23 (7%) had finished primary or middle school, 145 (44%) had finished higher or higher education, and 122 (37%) had finished graduate or higher education. In the entire biomass participants group, 55 (23%) were residing in kutcha houses, 98 (41%) in semi-pucca houses, and 84 (36%) in pucca houses; in the LPG study participants group, 45 (14% were residing in kutcha houses, 115 (35% in semi-pucca houses), and 168 (51% in pucca houses. Unadjusted mean PFT parameters for FVC, FEV1, FEV1/FVC, and PEF (p 0.05) were significantly lower in biomass users compared to LPG users (Figure 2).
Table 1: General Descriptive of the participated in the study.
|
Variables |
Biomass (Mean ± SD) |
LPG (Mean ± SD) |
|
Age |
40.83 ± 11.31 |
40.50 ± 10.25 |
|
Height |
154.69 ± 6.98 |
156.82 ± 7.24 |
|
Weight |
53.98 ± 9.99 |
59.64 ± 12.7 |
|
Age |
Biomass N (%) |
LPG N (%) |
|
<35 |
62(26) |
88(27) |
|
35-44 |
101(43) |
131(40) |
|
>45 |
74(31) |
109(33) |
|
BMI |
||
|
Under weight(<18.5) |
32(14) |
34(10) |
|
Normal (18.5-24.9) |
150(63) |
156(48) |
|
Overweight (25-29.9) |
45(19) |
99(30) |
|
Obesity (>30) |
10(4) |
39(12) |
|
Education |
||
|
Graduation &above |
17(7) |
23(7) |
|
High/Higher school |
131(55) |
145(44) |
|
Primary/middle |
53(23) |
122(37) |
|
Illiterate |
36(15) |
38(12) |
|
SES |
||
|
lower class |
43(18) |
52(16) |
|
Middle Class |
120(51) |
190(58) |
|
Upper |
74(31) |
86(26) |
|
House type |
||
|
Kutcha |
55(23) |
45(14) |
|
Pucca |
84(36) |
168(51) |
|
Semi-pucca |
98(41) |
115(35) |
|
Passive. Smoke |
||
|
No |
154(65) |
247(75) |
|
Yes |
83(35) |
81(25) |
 |
Figure 1: Pulmonary function test curve with outcome variables |
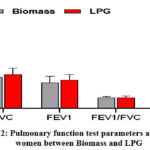 |
Figure 2: Pulmonary function test parameters among the women between Biomass and LPG |
Discussion
The findings of this study indicate a reduction in pulmonary function among the rural women living in households using biomass fuel for cooking compared to the women using LPG for cooking, even after controlling for a variety of significant confounders and variables (such as age, SES, education level, smoking, season, and other cooking exposures). Previous studies have also demonstrated decreased pulmonary function among the women using biomass in various parts of India 19-21. Lower pulmonary function was also statistically significant (p 0.01) in women with lower levels of education and lower socioeconomic status, which is consistent with previous research among biomass fuel users 15,22.
In the rural and suburban areas of developing countries, air pollution inside the dwellings usually reaches up to 1000 g/m3 during cooking with biomass, and this would increase the risk of developing lung dysfunction among women 6. Air pollution induces constriction of the smooth muscles of the airways and irritation of the mucous glands, resulting in wheezing and excessive sputum production. Biomass smoke contains a mix of gases and particulates that have been shown to compromise host defences 23. Inhaling these dangerous pollutants causes changes in the respiratory system, such as lung inflammation and activation of alveolar epithelial cells, which leads to increased mucus secretion and, eventually, airway remodelling 24,25. The use of biomass has also been linked to a number of pulmonary and extrapulmonary diseases. According to the World Health Organization, household air pollution causes around 3.8 million deaths worldwide 26. Due to air pollution, India has a disproportionately high death and disease load. This burden is commonly highest in the rural parts of India, where access to alternative, cleaner fuels is limited. The problem is compounded by poor ventilation in the houses where the food is cooked. Recent studies in India have found that using cleaner biomass cook stoves and clean fuels like biogas, electricity, and liquefied petroleum gas improves lung function indicators and reduces self-reported respiratory symptoms 27. The Government of India recently introduced a number of programmes to increase the use of clean fuel, including PMUY, Give-it-Up (GiU), and Pratyaksha Hastaantarit Laabh (PAHAL)—Direct Benefits Transfer for LPG (DBTL) 27. These programmes dramatically increased the use of clean fuels, particularly among lower-middle-income households and in urban areas. Due to several behavioural, social, cultural, and economic considerations like safety, the expense of refilling an LPG cylinder, and doorstep delivery, LPG uptake in rural regions continues to be a significant barrier 28. Therefore, it is necessary to expand the clean fuel program’s reach into remote and inaccessible locations.
Conclusion
The result observed in this study has demonstrated a decline in pulmonary function in rural women using biofuels. More interventional studies may be required to provide stronger evidence of this link and, more critically, to assess the extent of the health benefit that can be achieved by reducing exposure to acceptable levels. The recognition of the true size of the problem and corresponding efforts to increase early identification of respiratory impairments can help reduce the morbidity and mortality due to biofuel use.
Acknowledgment
We are grateful to the research participants, research support staff, and management of SREIHER.
Competing of Interests
There are no declared competing interests from the authors.
Funding Sources
There is no funding sources
References
- Tran VV, Park D, Lee YC. Indoor air pollution, related human diseases, and recent trends in the control and improvement of indoor air quality. International journal of environmental research and public health. 2020 Apr;17(8):2927.
CrossRef - Balmes JR. Household air pollution from domestic combustion of solid fuels and health. Journal of Allergy and Clinical Immunology. 2019 Jun 1;143(6):1979-87.
CrossRef - Saini J, Dutta M, Marques G. A comprehensive review on indoor air quality monitoring systems for enhanced public health. Sustainable environment research. 2020 Dec;30(1):1-2.
CrossRef - Kumar R, Sharma SK, Thakur JS, Lakshmi PVM, Sharma MK, Singh T: Association of air pollution and mortality in the Ludhiana city of India: a time-series study. Indian J Public Health 2010, 54(2):98.
CrossRef - Balakrishnan K, Ganguli B, Ghosh S, Sankar S, Thanasekaraan V, Rayudu VN, Caussy H: Part 1. Short-term effects of air pollution on mortality: results from a time-series analysis in Chennai, India. Research report (Health Effects Institute) 2011(157):7-44.
- Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Balakrishnan K, Brunekreef B, Dandona L, Dandona R: Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet 2017, 389(10082):1907-1918.
CrossRef - Schraufnagel DE, Balmes JR, Cowl CT, De Matteis S, Jung SH, Mortimer K, Perez-Padilla R, Rice MB, Riojas-Rodriguez H, Sood A, Thurston GD. Air pollution and noncommunicable diseases: A review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air pollution and organ systems. Chest. 2019 Feb 1;155(2):417-26.
CrossRef - Pandey A, Brauer M, Cropper ML, Balakrishnan K, Mathur P, Dey S, Turkgulu B, Kumar GA, Khare M, Beig G, Gupta T. Health and economic impact of air pollution in the states of India: the Global Burden of Disease Study 2019. The Lancet Planetary Health. 2021 Jan 1;5(1):e25-38.
CrossRef - Pathak U, Gupta NC, Suri JC. Risk of COPD due to indoor air pollution from biomass cooking fuel: a systematic review and meta-analysis. International journal of environmental health research. 2020 Jan 2;30(1):75-88.
- Sharma D, Jain S. Impact of intervention of biomass cookstove technologies and kitchen characteristics on indoor air quality and human exposure in rural settings of India. Environment international. 2019 Feb 1;123:240-55.
CrossRef - Dai X, Bui DS, Perret JL, Lowe AJ, Frith PA, Bowatte G, Thomas PS, Giles GG, Hamilton GS, Tsimiklis H: Exposure to household air pollution over 10 years is related to asthma and lung function decline. Eur Respir J 2021, 57(1).
CrossRef - Patel V, Foster A, Salem A, Kumar A, Kumar V, Biswas B, Mirsaeidi M, Kumar N: Long‐term exposure to indoor air pollution and risk of tuberculosis. Indoor Air 2021, 31(3):628-638.
CrossRef - World Health O: Review of evidence on health aspects of air pollution: REVIHAAP project: technical report. In.: World Health Organization. Regional Office for Europe; 2021.
CrossRef - Pandey A, Brauer M, Cropper ML, Balakrishnan K, Mathur P, Dey S, Turkgulu B, Kumar GA, Khare M, Beig G: Health and economic impact of air pollution in the states of India: the Global Burden of Disease Study 2019. The Lancet Planetary Health 2021, 5(1):e25-e38.
CrossRef - Saha A, Rao NM, Kulkarni PK, Majumdar PK, Saiyed HN: Pulmonary function and fuel use: a population survey. Respir Res 2005, 6(1):1-6.
CrossRef - Young BN, Clark ML, Rajkumar S, Benka‐Coker ML, Bachand A, Brook RD, Nelson TL, Volckens J, Reynolds SJ, L’Orange C, Good N. Exposure to household air pollution from biomass cookstoves and blood pressure among women in rural Honduras: a cross‐sectional study. Indoor air. 2019 Jan;29(1):130-42.
CrossRef - Salvi S, Barnes PJ: Is exposure to biomass smoke the biggest risk factor for COPD globally? Chest 2010, 138(1):3-6.
CrossRef - Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, van der Grinten CM, Gustafsson P: General considerations for lung function testing. Eur Respir J 2005, 26(1):153-161.
CrossRef - Sukhsohale ND, Narlawar UW, Phatak MS: Indoor air pollution from biomass combustion and its adverse health effects in central India: an exposure-response study. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine 2013, 38(3):162.
- Siddique S, Banerjee M, Ray MR, Lahiri T: Air pollution and its impact on lung function of children in Delhi, the capital city of India. Water Air Soil Pollut 2010, 212(1):89-100.
- Balakrishnan K, Mehta S, Kumar P, Ramaswamy P, Sambandam S, Kumar KS, Smith KR: Indoor air pollution associated with household fuel use in India: an exposure assessment and modeling exercise in rural districts of Andhra Pradesh, India. 2004.
- Behera D, Balamugesh T: Indoor air pollution as a risk factor for lung cancer in women. JAPI 2005, 53:190-192.
- Borchers-Arriagada N, Palmer AJ, Bowman DMJS, Williamson GJ, Johnston FH: Health impacts of ambient biomass smoke in Tasmania, Australia. Int J Environ Res Public Health 2020, 17(9):3264.
- Oluwole O, Arinola GO, Ana GR, Wiskel T, Huo D, Olopade OI, Olopade CO: Relationship between household air pollution from biomass smoke exposure, and pulmonary dysfunction, oxidant-antioxidant imbalance and systemic inflammation in rural women and children in Nigeria. Global journal of health science 2013, 5(4):28.
- Silva R, Oyarzún M, Olloquequi J: Pathogenic mechanisms in chronic obstructive pulmonary disease due to biomass smoke exposure. Archivos de Bronconeumología (English Edition) 2015, 51(6):285-292.
- World Health O: Air quality guidelines: global update 2005: particulate matter, ozone, nitrogen dioxide, and sulfur dioxide: World Health Organization; 2006.
- Clasen T, Checkley W, Peel JL, Balakrishnan K, McCracken JP, Rosa G, Thompson LM, Barr DB, Clark ML, Johnson MA: Design and rationale of the HAPIN study: a multicountry randomized controlled trial to assess the effect of liquefied petroleum gas stove and continuous fuel distribution. Environ Health Perspect 2020, 128(4):047008.
- Ravindra K, Smith KR. Better kitchens and toilets: both needed for better health. Environ Sci Pollut Res Int. 2018;25:12299-12302.
- Sharma D, Ravindra K, Kaur M, Prinja S, Mor S. Cost evaluation of different household fuels and identification of the barriers for the choice of clean cooking fuels in India. Sustainable Cities and Society. 2020 Jan 1;52:101825.

