
Manuscript accepted on :27-04-2023
Published online on: 21-06-2023
Plagiarism Check: Yes
Reviewed by: Dr. Deepak Bansal and Dr. Saumya Bipin
Second Review by: Dr. Nagham Aljamali
Final Approval by: Dr. Jihan Seid Hussein
Samyuktha Harikrishnan1 , Radha Pulate1, Steffy Terrance1, Ousama Shikfa1 and Jayadevan Sreedharan2*
, Radha Pulate1, Steffy Terrance1, Ousama Shikfa1 and Jayadevan Sreedharan2*
1College of Medicine, Gulf Medical University, Ajman, UAE.
2Epidemiology and Biostatistics, College of Medicine, Gulf Medical University, Ajman, UAE.
Corresponding Auther E-mail: drjayadevans@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2680
Abstract
Background: Type 2-diabetes mellitus (T2DM) is a chronic metabolic disease in which insulin resistance and reduced insulin with increased hepatic glucose production lead to hyperglycemia. The condition cannot be cured; however, the incidence can be delayed and the progression can be halted. This study researches the association of 2 modifiable risk factors- lifestyle and stress with Diabetes Mellitus. The study aimed to assess the role of stress and other lifestyle factors on the occurrence of diabetes mellitus. Studies on diabetes mellitus and its factors have not been done much in United Arab Emirates (UAE) so this research is aimed to determine the association between diabetes mellitus and, stress and lifestyle among residents of UAE. Methods: This case-control study was conducted in Ajman, United Arab Emirates. The participants were in the age group of 35 to 70 years. The duration of this study was six months. Patients with type-2 diabetes mellitus and without diabetes mellitus were chosen randomly, and data were collected using a questionnaire. After obtaining the questionnaire with the desired sample size, data analysis was carried out using SPSS-26. The Chi-square test was used to find an association between the categorical variables and a two-sided P-value < 0.05 was taken as significant. The sample size was calculated by taking the level of significance as 5% and the power of the study as 80%. As per the previous study, the stress in the general population reported was 30% and the crude OR for DM those who are stressed as 2.4. This basic information is used to calculate the minimum required sample size for this study. The case-control ratio is taken as 1:2. The total participants for this study was 195 (65 cases and 130 controls). The inclusion criteria were both male and female patients of all nationalities and the exclusion criteria were patients with other disease conditions such as CVD, cancer and pregnant women. Results: A total of 205 participants were included in the study (71 cases; 134 controls). The study results showed that the prevalence of diabetes mellitus was not associated with marital status, type of job, total income, exercise, BMI (Body mass index), and the nature of work seen in Table 1 and Table 2. The age of the participants and the prevalence of diabetes mellitus showed a significance of P<0.001. The psychologic stress also showed a significant association (P<0.05). This study also showed a significant association between the educational qualification of the participant and Diabetes mellitus. This study showed an association between age and diabetes, as well as stress and diabetes. Conclusion: This study shows age and stress are significantly associated with diabetes. Age is a non-modifiable risk factor, while stress is a modifiable risk factor, so reducing stress levels can help reduce the risk and progression of diabetes mellitus.
Keywords
Age; Diabetes Mellitus; Education; Lifestyle; Stress
Download this article as:| Copy the following to cite this article: Harikrishnan S, Pulate R, Terrance S, Shikfa O, Sreedharan J. Role of Lifestyle and Stress on Diabetes Mellitus: A Case-Control Study. Biomed Pharmacol J 2023;16(2). |
| Copy the following to cite this URL: Harikrishnan S, Pulate R, Terrance S, Shikfa O, Sreedharan J. Role of Lifestyle and Stress on Diabetes Mellitus: A Case-Control Study. Biomed Pharmacol J 2023;16(2). Available from: https://bit.ly/3CGHXYk |
Introduction
Type-2 diabetes mellitus is a chronic, heterogeneous metabolic disease in which insulin resistance and reduced insulin paired with increased hepatic glucose production lead to hyperglycemia. 90-95% of adult cases are caused by type-2 diabetes mellitus. A pathophysiological viewpoint reveals that the three main abnormalities that a patient with type-2 diabetes mellitus demonstrates are: resistance to the action of insulin in peripheral tissues, particularly muscle, fat, and liver, defects in insulin secretion, particularly in response to a glucose stimulus and an increased glucose production by the liver. Many factors lead to the development of type-2 diabetes mellitus, such as an increase in calorie intake, an increase in fat mass and a sedentary lifestyle, the inability of beta cells in pancreatic cells to adapt to less insulin sensitivity or an increase in insulin resistance. The genetic predisposition to T2DM determines how frequently and which beta failure happens, but no single genetic alteration has been identified that causes beta cell failure. Other factors increase the burden on beta cells, like overeating, leading to weight gain, puberty, pregnancy and a sedentary lifestyle1.
Some modifiable risk factors include BMI, physical inactivity, diet, and non-modifiable variables such as genetic factors and age2. Obesity has been associated with Type-2 Diabetes Mellitus for decades. Visceral/intra-abdominal fat is known to cause insulin resistance alongside several other metabolic variables, such as elevated total plasma cholesterol, insulin, and glucose concentrations. It has also been linked to high triglyceride and decreased plasma high-density lipoprotein cholesterol concentration. However, some studies have suggested that subcutaneous fat helps against insulin resistance. On these grounds, the association between insulin resistance and abdominal fat is independent of total adiposity. The correlation between an abnormal metabolism and intra- abdominal fat has not yet been clearly defined, but several hypotheses have been proposed to explore this association2.
A recent study on lifestyle’s effect on patients with diabetes mellitus found that people who consumed alcohol had the highest HbA1c levels. In the case of patients who practiced smoking, they had a higher risk of diabetes mellitus. However, light to moderate consumption of alcohol showed decreased risk in the case of cardiovascular diseases3. In the case of diet, low salt consumption was found effective in T2DM patients and also in managing the risk of cardiovascular diseases. Exercises play a very important role in the management of diabetes mellitus3. Sleep disturbances can also affect insulin action, alter leptin secretion and ghrelin, stimulate appetite, increase inflammatory cytokine production, and alter other risk factors. It was found that the alterations in the normal feeding pattern attuned to the circadian metabolism can change the relationship between the nutrient-metabolizing and nutrient-appearance enzymes. The alterations in fatty acid appearance concerning the lipoprotein lipase activity can lead to altered partitioning of lipids concerning vulnerable tissues, further leading to lipotoxicity and decreased leptin secretion, thereby increasing appetite. Another risk factor for insulin resistance and diabetes is Obstructive sleep apnea. Obstructive sleep apnea combines sleep fragmentation and hypoxemia. There is growing evidence of glucose control in patients with T2DM, which can be improved by treating sleep apnea, though poor compliance to therapy is a major barrier to success4.
Higher stress levels are attributable to diabetes displayed in both cross-sectional and longitudinal relationships with HbA1c. Stress is a potential contributor to chronic hyperglycemia in diabetes. Stress has long been shown to have major effects on metabolic activity. Stress stimulates the release of various hormones, resulting in elevated blood glucose levels. Although this is of adaptive importance in a healthy organism, in diabetes,stress-induced glucose increases cannot be metabolized properlydue to the relative or absolute lack of insulin.
Furthermore, regulation of these stress hormones may be abnormal in diabetes5. Although human studies on the role of stress in the onset and course of type II diabetes are few6. IL-6 is a protein the body produces to stimulate immune response and healing. It is a biomarker of acute and chronic stress that also has been associated with a greater likelihood of diabetes and high blood glucose7. Literature showed individuals with low inhibition were more likely to have diabetes than those with high inhibition due to the pathway from high anxiety5. This research is aimed to determine the association between diabetes mellitus and, stress and lifestyle among residents of UAE.
Materials and methods
This case-control study was conducted among the residents of Ajman, UAE, within the age group of 35-70 years. The study setting was Thumbay University Hospital, Ajman. Both male and female patients of all nationalities were included; pregnant women and patients with other disease conditions, such as cardiovascular diseases and cancer, were excluded. The minimum required sample obtained was 195 (65 cases and 130 controls), but collected data from 71 cases and 134 controls. This research was approved by the Institution Review Board of Gulf Medical University. Written consent was taken from the participants. Participants were provided with a brief description of the purpose of this research. Anonymity, privacy and confidentiality were maintained.
A draft questionnaire was developed and sent to the experts for content validation. The suggestions of the experts were included in the questionnaire before finalizing. The ‘Perceived stress scale’, a global self-assessment tool, analyzed the patient’s stress. The smoking and alcohol levels were also inquired in the questionnaire; the ex-user is defined as anyone who previously abstained from drinking alcohol and smoking for more than six months. The final questionnaire was distributed to the selected participants and asked to complete the information. Data were then entered into the Excel sheet, after which the analysis was done. This was recorded in the Excel sheet and then coded into SPSS version 27 for analysis. The descriptive statistics such as frequency, percentage, mean and SD was calculated. To assess the association, the Chi-Square test was used, t-test was also used to test the mean of the continuous variables. Simple and multiple logistic regression analyses were used to get the factors.
Results
This study included 71 cases and 134 controls, out of which 43 controls and 7 cases were below 40 years of age, 85 controls and 57 cases were between 40-59 years of age and 5 cases and seven controls were over the age of 60. Sixty-six controls and 39 cases were male, while 68 controls and 32 cases were female. Ten controls and five cases were single; 66 cases and 124 controls were married. Fourteen controls and 16 cases had a below-graduate level of education. Twenty-nine cases and 54 controls were graduates, whereas 66 controls and 26 cases were postgraduates. Fifty-six controls and 31 cases earned less than 4000 USD per month and 23 cases and 54 controls earned more than 4000 USD per month. Thirty-three controls and 12 cases were gold-collar workers, and 37 cases and 61 controls were white-collar workers. Eleven controls and seven cases were blue-collar workers, 27 controls and 15 cases said they were unemployed. The Chi-square test showed that the participant’s age and the presence of diabetes mellitus were associated (P <0.001). A statistically significant association was observed with education (P<0.05); cases were more in the higher education group compared to the control group. There was no statistically significant association between gender, marital status, income, occupation, and diabetes mellitus (table 1).
Table 1: Association of diabetes mellitus and sociodemographic variables
|
Variable |
Group |
Control |
Cases |
Total |
P |
||
|
No. |
% |
No. |
% |
||||
|
Age |
<40 |
43 |
32.1 |
7 |
9.8 |
50 |
<0.001 |
|
40 -59 |
86 |
64.2 |
57 |
80.3 |
143 |
||
|
>=60 |
5 |
3.7 |
7 |
9.5 |
12 |
||
|
Gender |
Male |
66 |
49.3 |
39 |
54.9 |
105 |
NS |
|
Female |
68 |
50.7 |
32 |
45.1 |
100 |
||
|
Marital Status |
Single |
10 |
92.5 |
5 |
7 |
15 |
NS |
|
Married |
124 |
7.5 |
66 |
93 |
190 |
||
|
Education |
Below Graduate |
14 |
10.4 |
16 |
22.5 |
30 |
<0.05 |
|
Graduate |
54 |
40.3 |
29 |
40.8 |
83 |
||
|
Postgraduate |
66 |
49.3 |
26 |
36.6 |
92 |
||
|
Income |
No income |
24 |
17.9 |
17 |
43.7 |
41 |
NS |
|
<15000 |
56 |
41.8 |
31 |
32.4 |
87 |
||
|
> 15000 |
54 |
40.3 |
23 |
32.4 |
77 |
||
|
Occupation |
Gold Collar |
33 |
25.0 |
12 |
16.9 |
45 |
NS |
|
White Collar |
61 |
46.2 |
37 |
52.1 |
98 |
||
|
Blue-collar |
11 |
8.3 |
7 |
9.9 |
18 |
||
|
Unemployed |
27 |
20.5 |
15 |
21.1 |
42 |
||
The chi-square test was used to assess the association.
This study showed the likelihood of diabetes increases as age increases. Figure 1 shows the association between age and diabetes. The yellow colour represents those with diabetes and the blue represents those without diabetes. A significant association was found between age and diabetic status (P<0.001). An increase in age showed an increase in the prevalence of diabetics by several folds. The adjusted OR observed was 4.2 and 9.7, respectively.
 |
Figure 1: Association between age and diabetes among cases and control. |
In Figure 2, the yellow colour represents those with diabetes and the blue represents those without diabetes. As seen, there is a significant association between stress and diabetes (P<0.05), i.e., an increase in stress levels and an increase in the prevalence of diabetes was observed. Stress significantly increases glucose concentrations in patients with Type-2 diabetes.
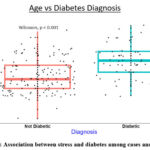 |
Figure 2: Association between stress and diabetes among cases and control. |
Figure 3 shows the combined impact of stress and age on diabetes. This graph is split into four quadrants based on the median age and median stress. The four quadrants are those with High stress with older age, high stress with younger age, low stress with old age and low stress with older age. The highest prevalence of diabetes is seen in those with high stress and old age, while the lowest prevalence is seen in the quadrant with low stress and younger age. This shows that age and stress increase the prevalence of diabetes independently, but those of older age with increased stress levels increase the prevalence of diabetes by further folds.
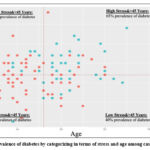 |
Figure 3: Prevalence of diabetes by categorizing in terms of stress and age among cases and control. |
The study investigated the association between various lifestyle factors and diabetes. This study observed an association between fast-food consumption and diabetes mellitus (P<0.01). Among the cases, about 20% used to take fast food more than once a week, whereas, in the control group, it was only 13%. Among the participants without diabetes, 26.9% had low stress and 73.1% had high stress, whereas, among the participants with diabetes, 11.3% had low stress and 88.7% had high stress. The results showed no association between smoking habits, alcohol consumption, type of diet, consumption of foods with high sugar content, carbonated drinks, and coffee/tea consumption with the status of the disease. However, there was an inverse association between fast food consumption and disease status (P<0.001). The consumption of white rice was not associated with the status of the disease.
The study categorized the participants into a control group and a case group. In the control group, 36 participants reported low-stress levels, while 98 reported high-stress levels. In contrast, in the cases group, only 8 participants reported low-stress levels, while 63 reported high-stress levels. The study found a statistically significant association between stress levels and disease status (P<=0.05), suggesting that higher stress levels may be a risk factor for developing diabetes (Table 2).
Table 2: Association of diabetes mellitus and other variables
|
Variable |
Group |
Control |
Cases |
Total |
P |
||
|
No. |
% |
No. |
% |
||||
|
FH of diabetes |
No |
35 |
26.1 |
15 |
21.1 |
50 |
NS |
|
Yes |
99 |
73.9 |
56 |
78.9 |
155 |
||
|
Exercise |
No |
44 |
32.8 |
25 |
35.2 |
69 |
NS |
|
Yes |
90 |
67.2 |
46 |
64.8 |
136 |
||
|
BMI |
Normal Weight |
32 |
23.9 |
22 |
31.0 |
54 |
NS |
|
Overweight |
65 |
48.5 |
30 |
42.3 |
95 |
||
|
Obese |
37 |
27.6 |
19 |
26.8 |
56 |
||
|
Smoking habit |
Current User |
12 |
9 |
10 |
14.1 |
22 |
NS |
|
Ex-User |
8 |
6 |
7 |
9.9 |
15 |
||
|
Never User |
114 |
85.1 |
54 |
76.1 |
168 |
||
|
Alcohol use |
Current User |
29 |
21.6 |
11 |
15.5 |
40 |
NS |
|
Ex-User |
13 |
9.7 |
5 |
7 |
18 |
||
|
Never User |
92 |
68.7 |
55 |
77.5 |
147 |
||
|
Consumption of fast food |
Never |
18 |
13.4 |
23 |
32.4 |
41 |
<0.001 |
|
Once a week |
99 |
73.9 |
34 |
47.9 |
133 |
||
|
> Once a week |
17 |
12.7 |
14 |
19.7 |
31 |
||
|
Stress |
Low Stress |
36 |
26.9 |
8 |
11.3 |
44 |
<0.05 |
|
High Stress |
98 |
73.1 |
63 |
88.7 |
161 |
||
The chi-square test was used to assess the association.
Crude and adjusted OR of variables associated with Diabetes Mellitus:
The study found that age and stress were significant risk factors for developing the disease. The crude OR for the age group between the age of 40 to 59 shows four times increase in the chance of developing diabetes mellitus, while those greater than or equal to 60 show nine times. Concerning stress, the crude OR shows three times increase in the likelihood of diabetes mellitus among those with stress. The adjusted OR for the age group between 40 to 59 also shows a four times higher chance and those above 60 show an almost ten times higher likelihood of developing diabetes mellitus. The study found that people between the ages of 40 and 59 were four times more likely to develop the disease than younger people. Similarly, people over 60 were nine times more likely to develop the disease than younger people. The study also found that people with high stress were three times more likely to develop the disease than those with low stress. This means that stress was a significant risk factor for developing the disease. (Table 3).
Table 3: Crude and adjusted Odds Ratio.
|
Variable |
Group |
Crude |
Adjusted |
||
|
OR |
CI |
OR |
CI |
||
|
Age |
<40 |
1 |
— |
1 |
— |
|
40-59 |
4.1 |
1.7-9.7 |
4.2 |
1.8-10.1 |
|
|
>=60 |
8.6 |
2.1-34.9 |
9.7 |
2.3-40.6 |
|
|
Stress |
Low stress |
1 |
— |
1 |
— |
|
High stress |
2.8 |
1.3-6.6 |
3.1 |
1.3-7.3 |
|
Discussion
Diabetes mellitus and Age
The OR observed for the variable age showed a high likelihood compared to other factors; the onset of diabetes is closely related to the ageing process. In the last few decades, the elderly population has increased worldwide, resulting in a high prevalence of diabetes mellites. Age was the most significant variable in this study. An increase in age showed an increase in the prevalence of diabetics by several folds6,7. The adjusted OR observed was 4.2 and 9.7, respectively. A systematic review of the studies from the Arabic countries reported that more than 50% of the studies agree that age is one of the main determinants of Type-2 DM8. Older people have more chances to practice a sedentary lifestyle which may also lead to obesity and T2DM9.
Diabetes mellitus and stress
The present study observed an association between stress and the status of diabetes mellitus. A Swiss study also supports the finding of the current study10. A study from the USA also observed the same finding; the study reported that as the levels of depression, distress and anxiety decreased, a downward trend was observed in the levels of HbA1c11.These studies were conducted in different populations and reported the same results. Growing evidence suggests that stress is associated with an increased risk of developing diabetes. A study investigated the relationship between stress and diabetes and found that chronic stress may contribute to developing the disease12. It is possible to conclude that there is an association between stress and Diabetes Mellitus.
Diabetes mellitus and fast-food consumption
The present study observed an association between fast food consumption and diabetes mellitus; patients who had diabetes consumed less fast food. A study from Cambridge University found that more fast-food outlets increased the odds of diabetes cases; for every additional two outlets per neighborhood can expect one additional diabetes case11,12.
Another study also reported a strong positive association between weight gain and insulin resistance, suggesting that fast food increases the risk of obesity and type-2 diabetes13,14. Most studies show a significant association between fast food and diabetes, while our study shows an inverse association. This could be because of the diet advised by their physician to maintain and improve their blood glucose levels, as the cases included were prevalent. Most studies attempt to establish a relationship between fast food consumption and diabetes, suggesting that fast food contributes to the disease’s development. However, my study indicates an inverse relationship between fast food intake and the incidence of diabetes15,16.
. This unexpected finding suggests that the relationship between fast food consumption and diabetes may not be as straightforward as previously assumed and warrants further investigation. A Systematic Review observed that statistically significant association between diabetes mellitus and age. The disease’s prevalence was higher among older age groups in urban dominance17.18.These studies concur with our study and show a significant association between age and the prevalence of diabetes mellitus.
Diabetes mellitus and, family history and BMI
This study did not observe any statistically significant association with a family history of diabetes mellitus, even though studies have found that family history is an important risk factor for prediabetes, especially for combined impaired glucose tolerance and impaired fasting glucose9,16. Although there was no association between BMI and Diabetes in the present study, a study in India found that the likelihood of being diabetic is higher among overweight and obese individuals than among non-overweight individuals19,20.
Conclusion
This study observed a significant association between age and stress to type 2 diabetes mellitus. Based on this study, it can be inferred that age and stress are both factors associated with the development of diabetes. Specifically, the study suggests that individuals who experience high levels of stress may have an increased risk of developing diabetes and that older individuals may also be at a greater risk for developing the condition. These findings highlight the importance of managing stress and maintaining healthy lifestyle habits as people age, to reduce the risk of developing diabetes.
Conflict of Interest
There is no conflict of interest.
Funding sources
There are no funding sources
References
- Papaetis GS, Papakyriakou P, Panagiotou TN. Central obesity, type 2 diabetes and insulin: exploring a pathway full of thorns. Arch Med Sci. 2015;11(3):463–482.
CrossRef - Johansson A, Drake I, Engström G, Acosta S. Modifiable and Non-Modifiable Risk Factors for Atherothrombotic Ischemic Stroke among Subjects in the Malmö Diet and Cancer Study. Nutrients. 2021 Jun 6;13(6):1952.
CrossRef - Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman Med J. 2012 Jul;27(4):269-73.
CrossRef - Knutson KL. Impact of sleep and sleep loss on glucose homeostasis and appetite regulation. Sleep Med Clin. 2007;2(2):187–197.
CrossRef - Kyle W. Murdock, Angie S. LeRoy, Tamara E. Lacourt, Danny C. Duke, Cobi J. Heijnen, Christopher P. Fagundes. Executive functioning and diabetes: The role of anxious arousal and inflammation. Psychoneuroendocrinology, 2016; 71: 102.
CrossRef - Mussa BM, Schauman M, Kumar V, Skaria S, Abusnana S. Personalized intervention to improve stress and sleep patterns for glycemic control and weight management in obese Emirati patients with type 2 diabetes: a randomized controlled clinical trial. Diabetes Metab Syndr Obes. 2019 Jun 28; 12:991-999.
CrossRef - Nunes MA, Kučerová K, Lukáč O, Kvapil M, Brož J. Prevalence of diabetes mellitus among Roma populations—a systematic review. International journal of environmental research and public health. 2018 Nov;15(11):2607.
CrossRef - Edward G. Lakatta, MD and Daniel Levy, MD, Arterial and Cardiac Aging: Major Shareholders in Cardiovascular Disease Enterprises, Volume 107, Issue 2, Jan 21 2003, Pages 346-354.
CrossRef - Milibari AA, Matuure EY, Gadah EM. Prevalence, determinants and prevention of Type 2-Diabetes Mellitus (T2DM) in Arabic countries: A systematic review study. ICUS Nurs Web J 2020. Available at http://www.hsj.gr/. Accessed on Oct 10 2022.
- Faulenbach M, Uthoff H, Schwegler K, Spinas GA, Schmid C, Wiesli P. Effect of psychological stress on glucose control in patients with Type 2-diabetes. Diabet Med. 2012 Jan;29(1):128-31.
CrossRef - Bodicoat DH, Carter P, Comber A, Edwardson C, Gray LJ, Hill S, Webb D, Yates T, Davies MJ, Khunti K. Is the number of fast-food outlets in the neighbourhood related to screen-detected type 2-diabetes mellitus and associated risk factors? Public Health Nutr. 2015 Jun;18(9):1698-705.
CrossRef - Sharma Kumar Vivek and Singh Gurjeet Thakur *, Chronic Stress and Diabetes Mellitus: Interwoven Pathologies, Current Diabetes Reviews 2020; 16(6) . https://dx.doi.org/10.2174/1573399815666191111152248
CrossRef - Pereira MA, Kartashov AI, Ebbeling CB, Van Horn L, Slattery ML, Jacobs DR Jr, Ludwig DS. Fast-food habits, weight gain, and insulin resistance (the CARDIA study): 15-year prospective analysis. Lancet. 2005 Jan 1-7;365(9453):36-42.
CrossRef - Al-Rifai RH, Majeed M, Qambar MA, Ibrahim A, AlYammahi KM, Aziz F. Type 2 diabetes and prediabetes mellitus: a systematic review and meta-analysis of prevalence studies in women of childbearing age in the Middle East and North Africa, 2000–2018. Systematic reviews. 2019 Dec 1;8(1):268.
CrossRef - Chowdhury EA, Richardson JD, Holman GD, Tsintzas K, Thompson D, Betts JA. The causal role of breakfast in energy balance and health: a randomized controlled trial in obese adults. J Am Heart Assoc. 2016 Dec 20;5(12):e003327. doi: 10.1161/JAHA.116.003327. PMID: 27999003; PMCID: PMC5216626.
CrossRef - Robery L Barbieri, David A Ehrmann. Clinical manifestations of polycystic ovary syndrome in adults: UpToDate;2020.
- Adnan M, Aasim M. Prevalence of type 2 diabetes mellitus in adult population of Pakistan: a meta-analysis of prospective cross-sectional surveys. Annals of Global Health. 2020;86(1).
CrossRef - Cai H, Li G, Zhang P, Xu D, Chen L. Effect of exercise on the quality of life in type 2-diabetes mellitus: a systematic review. Qual Life Res. 2017 Mar;26(3):515-530.
CrossRef - Reinehr T Type 2 diabetes mellitus in children and adolescents. World J Diabetes. 2013;4(6):270-281
CrossRef - Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, D’Alessio DA, Davies MJ. 2019 update to: management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes care. 2020 Feb 1;43(2):487-93.
CrossRef

