
Manuscript accepted on :31-08-2022
Published online on: 12-09-2022
Plagiarism Check: Yes
Reviewed by: Dr. B Surendiran
Second Review by: Dr. Hind Shakir
Final Approval by: Dr. H Fai Poon
I Wayan Niryana1* , Steven Awyono2 , Kevin Kristian Putra2, Sri Maliawan1, Nyoman Golden1, Tjokorda Gde Bagus Mahadewa1 and Made Gemma Daniswara Maliawan1
, Steven Awyono2 , Kevin Kristian Putra2, Sri Maliawan1, Nyoman Golden1, Tjokorda Gde Bagus Mahadewa1 and Made Gemma Daniswara Maliawan1
1Neurosurgery Division, Department of Surgery, Faculty of Medicine, Universitas Udayana, Sanglah General Hospital, Bali, Indonesia.
2Neurosurgery Residency Program, Faculty of Medicine, Universitas Udayana, Sanglah General Hospital, Bali, Indonesia.
Corresponding Author E-mail: niryanawayan@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2518
Abstract
Dandy-Walker Malformation presents as a congenital anomaly that affects the posterior fossa. Presenting hydrocephalus as secondary to Dandy-Walker Malformation is the main concern and complication. The cyst formation in the posterior fossa obstructs the cerebrospinal flow that led to the hydrocephalus. Ideal management to treat Dandy-Walker malformation are varied. Shunting, cyst excision, and endoscopy third ventriculostomy are the proposed management. Case Report Presenting a case of a 1-month-age male baby who was diagnosed with vermis agenesis and posterior fossa enlargement by antenatal ultrasound. Later on, Magnetic Resonance Imaging revealed Dandy-Walker Malformation with hydrocephalus and aqueduct obstruction. Cystoperitoneal shunt was performed for this patient. Proximal shunt trajectory measured from Magnetic Resonance Imaging. As the goal of therapy is to achieve normal development, this patient needs long-term follow-up in collaboration with pediatric and physiotherapy. After 18 months of follow-up, he was able to crawl with routine and proper physiotherapy. Conclusion Hydrocephalus in Dandy-Walker Malformation patients related to aqueduct obstruction may be treated with a single Cystoperitoneal shunt. Aqueduct obstruction in these patients may be temporary due to high pressure on the posterior fossa that pushed the vermis forward. Cystoperitoneal shunt may reduce posterior fossa pressure and then deprive the pressure that obstructs aqueduct.
Keywords
Aqueduct Obstruction; Cystoperitoneal shunt; Dandy-Walker malformation; Hydrocephalus; Posterior Fossa Cyst Formation
Download this article as:| Copy the following to cite this article: Niryana I. W, Awyono S, Putra K. K, Golden N. Cystoperitoneal Shunting for Patient with Hydrocephalus Associated with Aqueductal Obstruction in Dandy-Walker Malformation: A Case Report. Biomed Pharmacol J 2022;15(3). |
| Copy the following to cite this URL: Niryana I. W, Awyono S, Putra K. K, Golden N. Cystoperitoneal Shunting for Patient with Hydrocephalus Associated with Aqueductal Obstruction in Dandy-Walker Malformation: A Case Report. Biomed Pharmacol J 2022;15(3). Available from: https://bit.ly/3qs1HsO |
Introduction
Dandy-Walker malformation (DWM) or Dandy-Walker syndrome is one of congenital anomalies that affects the posterior fossa. It has typical main radiographic features as described by Klein which include a large cystic lesion in midline posterior fossa that communicates with fourth ventricle. Although its relatively rare, one of the main issues related to DWM is hydrocephalus.1,2 Hydrocephalus as the primary concern and complication, may arise within 3 months and need cerebrospinal fluid (CSF) diversion.3,4 In general, there are two principles in managing these patients either by direct cyst fenestration or performing shunting procedures. Later on, the shunting procedure also has several techniques either by placing the proximal catheter on 1) lateral ventricle, 2) posterior fossa cyst, or 3) using two proximal catheters that are placed subsequently on the lateral ventricle and posterior fossa cyst that may have each own distal catheter, or involving Y-connector. It may vary for each individual that may be determined by patient symptoms and aqueduct patency.5,6 This paper reports a case of DWM with hydrocephalus and aqueductal obstruction that was treated using cystoperitoneal (CP) shunt placement.
Case Report
Table 1. Patient Details
| Birth Gestation Age | 34th week |
| Sex | Male |
| Birth Weight | 1550 g |
| Birth Length | 42 cm |
| Head Circumference | 33 cm |
| Birth Order | Second Born |
|
Ante Natal Care Status |
Every Trimester to obstetrician |
A baby boy was born by cesarean section at 34th-week of gestation age. Ultrasound antenatal care found vermis agenesis with enlargement of the posterior fossa on the 25th-week of gestation age. His birth weight was 1550 g and 42 cm in length. At that time, muscle contraction was low with hypotonicity. Head circumference was 33 cm with enlargement of posterior fontanelle. Magnetic resonance imaging (MRI) was performed and showed enlargement of the posterior fossa with large posterior cranial fossa cystic lesion, absence of vermis, elevation of torcular and lambdoid with cerebellar hemisphere hypoplasia. We then diagnose the patient with Dandy-Walker malformation with hydrocephalus and aqueduct obstruction.
 |
Figure 1: Preoperative MR evaluation A) Axial; B) Coronal; C) Sagittal, revealed a large posterior fossa cyst that suppresses cerebellum forward and leads to aqueductal obstruction. |
We then planned to perform cystoperitoneal shunting procedure using flat bottom, low pressure valve was performed on 36th day of age. On the day of surgery, the head circumference was 45 cm (Fig 1), with enlargement and bulging of the posterior fontanelle. Based on MRI, we then calculate the angle and depth of the trajectory which is very important to minimize shunt problems later on. Postoperative care was carried out in pediatric intensive care unit for one day and the patient is allowed to go home on the fifth day. As the goal of this surgery is to achieve normal growth and development, we worked closely with the pediatrician and medical rehabilitation unit to achieve it. Postsurgical MRI was performed one year after surgery and showed a reduction in cyst with minimal CSF flow from aqueduct and shunt placement on posterior fossa cyst. On the 18thmonth of follow-up, the head circumference was 48 cm and the patient was able to crawl with routine and proper physiotherapy.
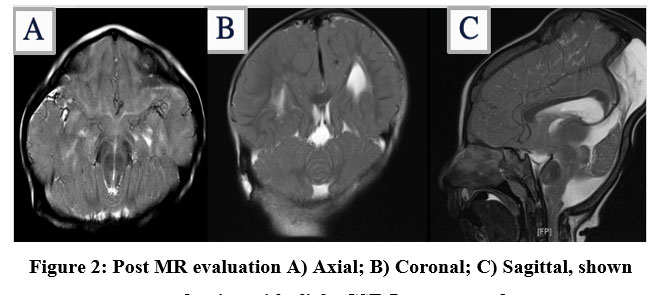 |
Figure 2: Post MR evaluation A) Axial; B) Coronal; C) Sagittal, shown cyst reduction with slight CSF flow on aqueduct. |
Discussion
Several concepts explained the etiopathogenesis of Dandy-Walker malformation such as atresia of Luschka and Magendie foramen which later explained that this malformation primarily occurs due to developmental anomaly of the neural tube on cerebellum level.6 Hydrocephalus as the complication of DWM mostly develops in the first 3 months and must be considered multifactorial.8 The impairment of cerebrospinal fluid (CSF) flow might occur both proximal and distal from the outlet of the fourth ventricle.9 Barkovich et al., also explain that hydrocephalus may be related to cyst compression on the cerebellum that mechanically obstructs CSF flow over the fourth ventricle outlets.(10) Aqueductal obstruction may develop due to the consequence of developmental abnormality or secondary to vermian herniation through the tentorial notch which may be called “functional aqueduct stenosis”.10–12
No superiority between Ventriculoperitoneal (VP) shunt, CP shunt, and Y-shunt.13 Sawaya and McLaurin proposed that CP shunt has superiority as commonly there are no stenosis between supratentorial and infratentorial compartments. The VP shunt placement may lead to aqueduct obstruction due to disturbance of CSF hydrodynamics.7 Recently, there was also a new endoscopic transaqueductal technique that was made to avoid complications of y-connector.13 Yüceer et al., found that DWM is commonly associated with other congenital anomalies that must be mentioned and explained to the family as the holistic approach to manage DWM patients. In their study, six out of thirteen patients have complication that commonly related to excision of the cyst and suggests to perform CP shunt or CP shunt with VP shunt subsequently to treat DWM.14 There are several reasons for failure in DWM with hydrocephalus such as obstruction, infection, and functional problem of the shunt system, and mailnly it just needs simple shunt revision.2,14
Several considerations may be used to determine the choice of proximal shunt placement such as patient symptoms and aqueduct patency. As aqueductal obstruction is rarely associated with DWM, usually single shunt placement is sufficient to treat CSF accumulation both supra- and infratentorial. Previous study had several findings regarding aqueductal obstruction in DWM patients.6 MRI evaluation may be used to evaluate this patency as obstruction may be seen as flow-void in T2-weighted images. Despite the success of shunt placement, there are reports of patients who have worsening conditions due to the thickened and adhesion of posterior fossa cyst arachnoid that later treated by performing open fenestration via suboccipital craniotomy.5 Talamonti et al., reported one patient with DWM and documented enlargement of occipital meningocele that was treated with cele resection. Unfortunately, on the 7th postoperative day there are large subcutaneous cerebrospinal fluid collections and need further CP shunt.16
The main advantage of VP Shunt is the relatively easier and more familiar procedure. It also has relatively lower incidence of migration or malposition. Nevertheless, in patients with aqueductal obstruction, VP shunt placement will reduce supratentorial pressure, thus increasing risk in developing central upward herniation. As for CP Shunt, the concept is that the proximal placement of shunt may accommodate CSF flow from supratentorial. Due to upward displacement of the tentorium, it is also easier to place the proximal shunt inside the cyst.11 Preoperative findings of aqueductal obstruction may be temporary due to mechanical compression from the vermis or cyst. This may also be relieved by shunt placement on the posterior fossa by removing the mechanical compression.
CP shunt and VP shunt may be performed simultaneously using two different systems or by using a y-connector placed to communicate between two proximal shunts. This procedure had relatively high complications such as malposition, shunt misplacement, intracranial hemorrhage, infection, shunt blockage, and even mortality. Several studies explained hydrocephalus in DWM patients may be caused by aqueduct obstruction due to upward herniation of the cyst or cerebellum.3,4,8,9,11) Others mentioned that uncal herniation may lead to ventricular blockage. This herniation might occur due to chronic negative pressure on supratentorial in relation to infratentorial.11, 13 A single shunt placement on the ventricle may lead to upward central herniation due to high pressure on the posterior fossa, especially on patients with aqueduct obstruction.14 Mandizawa et al., reported three groups of possible etiology for centra brain herniation 1) shunt related, 2) cyst related, and 3) other. As for our case, we demonstrated a successful CP shunt installment in DWM with aqueduct obstruction. This may be explained because this obstruction is due to temporary pressure caused by cyst to the cerebellum.17
As to optimizing and maximizing shunt-independent patient, several endoscopic techniques were performed.18)A posterior approach of endoscopic third ventriculostomy (ETV) with or without concomitant VP shunt may be performed, but these may need two-staged surgery and reported to need shunt revisions. Posterior approach for ETV has several obstacles and found to be difficult and also dangerous as it may conceal a deep draining vein structure with very thick arachnoid membranes that need more effort to penetrate it.13
Cerebellar development, intellectual function, and cerebellar dysfunction has no connection to cerebellar size preoperatively.19
Conclusions
Hydrocephalus in DWM patients may be related to aqueduct obstruction. This obstruction occurred due to temporary compression of the posterior fossa cyst that pushed the vermian forward. Although this obstruction separates CSF compartment of lateral and third ventricle with cyst and fourth ventricle, by releasing the cyst pressure using a single CP shunt may deprive the temporary compression and generate the connection between all CSF compartment.
Statement of Informed Consent
Written informed consent was obtained from the patient to publish this case report and accompanying images.
Acknowledgement
Not applicable.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding Source
There is no funding source.
References
- Shuto T, Sekido K, Ohtsubo Y, Saida A, Yamamoto I. Dandy-Walker Syndrome Associated with Occipital Meningocele and Spinal Lipoma. Neurol Med Chir. 1999;39:544–7.
CrossRef - Yengo-Kahn A, Wellons J, Hankinson T, Hauptman J, Jackson E, Jensen H et al. Treatment strategies for hydrocephalus related to Dandy-Walker syndrome: evaluating procedure selection and success within the Hydrocephalus Clinical Research Network. Journal of Neurosurgery: Pediatrics. 2021;28(1):93-101.
CrossRef - Spennato P, Cascone D, Martino G Di, Mirone G, Ruggiero C, Cinalli G. Dandy-Walker Malformations/Variants. In: Rocco C Di, Pang D, Rutka JT, editors. Textbook of Pediatric Neurosurgery. New York: Springer; 2020. p.831–56.
CrossRef - Dastoli PAD, Nicácio JM, Da Costa MDS, Suriano IC, Da Silva MC, Cavalheiro S. Hydrocephalus and Dandy- Walker Malformation: a review. Arch Pediatr Neurosurg. 2020;2(3(September-December)):e442020.
CrossRef - Villavicencio AT, Wellons JC, George TM. Avoiding Complicated Shunt Systems by Open Fenestration of Symptomatic Fourth Ventricular Cysts Associated with Hydrocephalus. Pediatr Neurosurg. 1999;29:314–9.
CrossRef - Mohanty A. Endoscopic Third Ventriculostomy with Cystoventricular Stent Placement in the Management of Dandy-Walker Malformation: Technical Case Report of Three Patients. Neurosurgery. 2003;53(5):1223–9.
CrossRef - Todo T, Usui M, Araki F. Dandy-Walker Syndrome Forming a Giant Occipital Meningocele. Neurol Med Chir. 1992;33:845–50.
CrossRef - Hirsch J, Pierre-kahn A, Renier D, Sainte-rose C, Hoppe-hirsch E. The Dandy-Walker malformation. J Neurosurg. 1984;61:515–22.
CrossRef - Stambolliu E, Ioakeim-Ioannidou M, Kontokostas K, Dakoutrou M, Kousoulis AA. The Most Common Comorbidities in Dandy-Walker Syndrome Patients: A Systematic Review of Case Reports. J Child Neurol. 2017;32(10):886–902.
CrossRef - Barkovich AJ, Kjos BO, Norman D, Edwards MS. Revised Classification of Posterior Fossa Cysts and Cystlike Malformations Based on the Results of Multiplanar MR Imaging. Am J Neuroradiol. 1989;10(5):977–88.
CrossRef - Spennato P, Mirone G, Nastro A, Buonocore MC, Ruggiero C. Hydrocephalus in Dandy – Walker malformation. Child’s Nerv Syst. 2011;27:1665–81.
CrossRef - Raimondi AJ, Samuelson G, Yarzagaray L, Norton T. Atresia of the foramina of Luschka and Magendie: The Dandy-Walker Cyst. J Neurosurg. 1969;31(2):202–16.
CrossRef - Unal OF, Aras Y, Aydin A, Akcakaya MO. Ascending transaqueductal Cystoventriculoperitoneal Shunting in Dandy-Walker Malformation : Technical Note. Pediatr Neurosurg. 2013;(48):389–93.
CrossRef - Yüceer N, Mertol T, Arda N. Surgical Treatment of 13 Pediatric Patients with Dandy-Walker Syndrome. 2007;358–63.
CrossRef - Dong Z, Jia Y, Gao Z, Li Q, Niu L, Yang Q et al. Y-shaped shunt for the treatment of Dandy-Walker malformation combined with giant arachnoid cysts: A case report. World Journal of Clinical Cases. 2022;10(7):2275-2280.
CrossRef - Talamonti G, Picano M, Debernardi A, Bolzon M, Teruzzi M, Aliberti GD. Giant Occipital Meningocele in an 8-year-old Child with Dandy – Walker Malformation. Child’s Nerv Syst. 2011;167–74.
CrossRef - Mandiwanza T, Kaliaperumal C, Caird J. Central brain herniation in shunted Dandy walker cyst. Child’s Nerv Syst. 2013;29:1035–8.
CrossRef - Almeida G, Matsuhita H, Mattosinho-França L, Shibata M. Dandy-Walker Syndrome: Posterior Fossa Craniectomy and Cyst Fenestration After Several Shunt Revisions. 1990;6:335–7.
CrossRef - Gerszten PC, Albright AL. Relationship between Cerebellar Appearance and Function in Children with Dandy-Walker Syndrome. Pediatr Neurosurg. 1995;23:86–92.
CrossRef

