
Manuscript accepted on :21-07-2022
Published online on: 25-07-2022
Plagiarism Check: Yes
Reviewed by: Dr. Nicolas Padilla
Second Review by: Dr. Ahmed Salah
Final Approval by: Dr. Ayush Dogra
Neha Daniel George, Sonal Bhat and Sunil B. V
Department of Anaesthesiology, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal India.
Corresponding Author E-mail: sonalbhat27@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2490
Abstract
Background : Analgesia post knee arthroplasties are crucial in early postoperative recovery and discharge . The objective of this study was to compare the analgesic efficacy of Adductor canal block with that of femoral nerve block in patients undergoing knee arthroplasties. Methods : 140 participants aged 18 years & above under American Society of Anaesthesiologists 1 and 2 physical status undergoing knee arthroplasty under spinal anaesthesia were included and were divided into 2 groups – Adductor canal block and femoral nerve block who were administered blocks under ultrasound guidance. The preoperative Visual Analog Scale score, haemodynamic variables and postoperative Visual Analog Scale scores were recorded. Results : The Visual Analog Scale scores between the two groups were not statistically significant however, a significant difference in the time taken by the Adductor canal block participants to request analgesia and to ambulate. Conclusion: Adductor canal block with Dexmedetomidine was equally efficacious when compared to Femoral nerve block with Dexmedetomidine in patients undergoing Total knee arthroplasty.
Keywords
Dexmedetomidine; Femoral nerve block; Postop Analgesia; Total Knee Arthroplasty; Ultrasonography guided nerve blocks Adductor canal block
Download this article as:| Copy the following to cite this article: George N. D, Bhat S, Sunil B. V. Comparison of Femoral Nerve Block with Dexmedetomidine and Adductor Canal Block with Dexmedetomidine for Postoperative Analgesia for Total Knee Arthroplasty. Biomed Pharmacol J 2022;15(3). |
| Copy the following to cite this URL: George N. D, Bhat S, Sunil B. V. Comparison of Femoral Nerve Block with Dexmedetomidine and Adductor Canal Block with Dexmedetomidine for Postoperative Analgesia for Total Knee Arthroplasty. Biomed Pharmacol J 2022;15(3). Available from: https://bit.ly/3oqkbsH |
Introduction
The very severe pain after Total Knee Arthroplasty (TKA) required adequate postoperative analgesia which proved crucial for early rehabilitation(1,2). Due to this established fact, Peripheral Nerve Block ( PNB ) were preferred as other modes of pain management such as Epidural analgesia and patient controlled analgesia were seen to be associated with side effects(3-6). PNBs were implemented to facilitate early ambulation, rehabilitation, reduced hospital stay, cost of treatment and patient satisfaction(3). Femoral nerve block ( FNB ) is the widely used standard peripheral nerve block to provide postop analgesia but has the major downside of weakening the quadriceps weakness and hence delaying rehabilitation.(7- 9) Adductor canal block (ACB), an alternative nerve block, has gained popularity as it provides optimal pain relief while maintaining the motor function in the postoperative period(10-25). Pain relief offered by femoral nerve block was seen to compromise the preservation of muscle strength concluding that the ideal nerve block for TKA should provide effective analgesia while preserving the muscle power to expedite the recovery Dexmedetomidine, an alpha 2 agonist is being used as an additive at a of 1 mcg/kg for blocks as it is known to prolong the duration of the block. Dexmedetomidine acts by inhibition of hyperpolarisation-activated cation current. Other mechanism are centrally mediated pain relief in peripheral nerve blockades, alpha 2B adrenoceptor- mediatedvasoconstrictory effects,weakening of the inflammatory response and direct action on peripheral nerve.Dexmedetomidine enhances activity dependent hyperpolarisation by inhibiting hyperpolarisation activated cation current which plays a key role in cell excitation, especially its firing frequency in both the central and peripheral nervous systems. (26-28) Hence by conducting the study we compared the postoperative analgesic efficacy of FNB and ACB with dexmedetomidine, along with their effect on patient hemodynamics, time for rescue analgesia and success of postoperative ambulation.
Materials and methods
This study was designed to be a comparative, observational study which was conducted at Kasturba Medical College Hospitals, Mangalore. The duration of the study was from September 2019 to June 2021 with study subjects included throughout the duration.
All patients between 18-70 years with BMI < 35 kg/m2 who were ASA I, II posted for elective TKA were chosen. Those who refused to participate, with h/o Local anaesthetic allergy, Coagulopathy or Bleeding diathesis, H/o peripheral neuropathy, Local skin infection, Significant psychiatric or mental disorders and Neurological deficits involving lower limbs were excluded. Institutional Ethics Committee approval was obtained. (IEC KMC MLR 08-19/347).
Written and informed consent was taken from all the patients participating in this observational study.
Pre-anaesthetic checkup was conducted thoroughly and patients were explained the procedure, benefits and risks associated with it.
The study was conducted on 140 patients who were designated into two groups: Group ACB (Those who received Adductor Canal Block) and Group FNB (Those who received Femoral Nerve Block) with 70 participants each . The sample size was calculated using the formula –
Where Z1-α = 1.96 (at 5% level of significance with 95 % confidence interval)
Z1-β = 0.84 (with 80% power)
σ = 1.96 ( standard deviation )
d = 0.9 ( clinically significant difference )(23)
n=70 in each group
Monitors were connected are Electrocardiogram, Pulse oximetry and noninvasive Blood pressure in the preoperative area. An appropriate sized intravenous cannula were secured for drug and fluid administration. Spinal Anaesthesia was administered with 0.5% heavy Bupivucaine using 25/23 G QBS needle. Adequate blockade was achieved.
The study participants were sub-divided into two :
Group ACB – Subjects received ACB with 20 ml of 0.25% bupivacaine and 50 microgram of dexmedetomidine under ultrasound guidance .
GROUP FNB – Subjects received FNB with 20 ml of 0.25% bupivacaine and 50 microgram of dexmedetomidine under ultrasound guidance .
A VAS score was recorded before and immediately after the block at 5 and 10 minutes. Immediate post operative pain was measured at 2, 6,10, 12 and 24 hours using VAS score. If the VAS score was >4, rescue analgesia; injection paracetamol 10mg/kg iv infusion was given over 10 to 15 minutes w. Post-operative time of first analgesic request and the total dose were recorded . The time required by the subject to ambulate were also recorded.
Data Analysis
To analyze the data, SPSS version 25 (IBM) was used . Unpaired t-têst & chì-square test were used to compare between 2 groups. Paìred-t test used to compare analgesic efficacy of ACB and FNB. Repeated measures AN0VA was performed to compare the data across various time periods, also post-hòc analysís was done by Bonferronï test. Statistical significance of p-value less than 0.05 were considered significant .
Results
One hundred and forty patients were included in this study with seventy participants allotted to each group .
The mean age in the study was 65.9 ± 6.27 years in the ACB group while it was 67.54 ± 5.01 years. (Table 1).
Table 1: Patient demographics – Age ( mean ).
| N* | Mean | Std. Deviation | t test p value | |||
| Age (yrs ) | ACB | 70 | 65.90 | 6.27 | 0.089 | NS** |
| FNB | 70 | 67.54 | 5.01 | |||
* N- Number
** NS – Not Significant
It was noted that the majority of the study population belonged to the age group of 61-70 years in both the groups followed by the those above 70 years old. ( Figure 1).
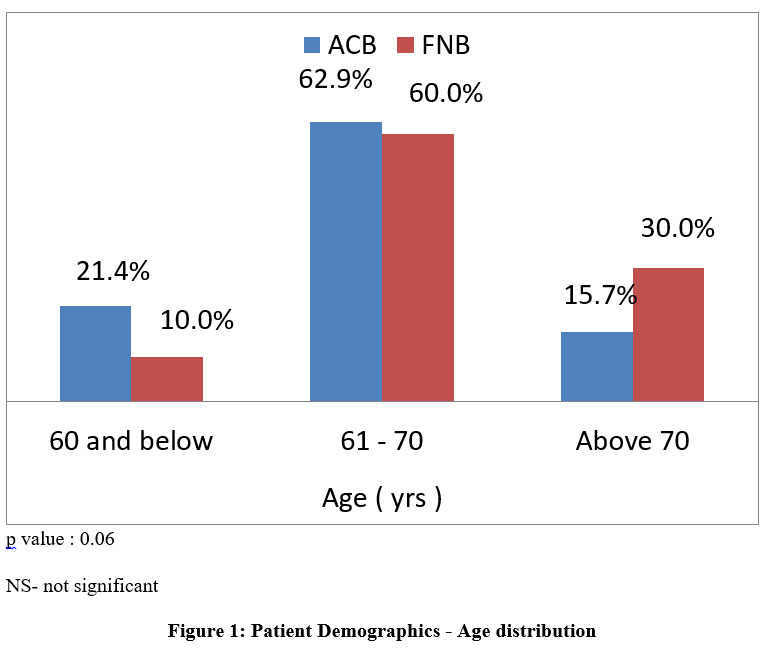 |
Figure 1: Patient Demographics – Age distribution. |
Among all the participants, females accounted for the majority at 55.7% in the ACB group and 62.9% in FNB group. (Figure 2).
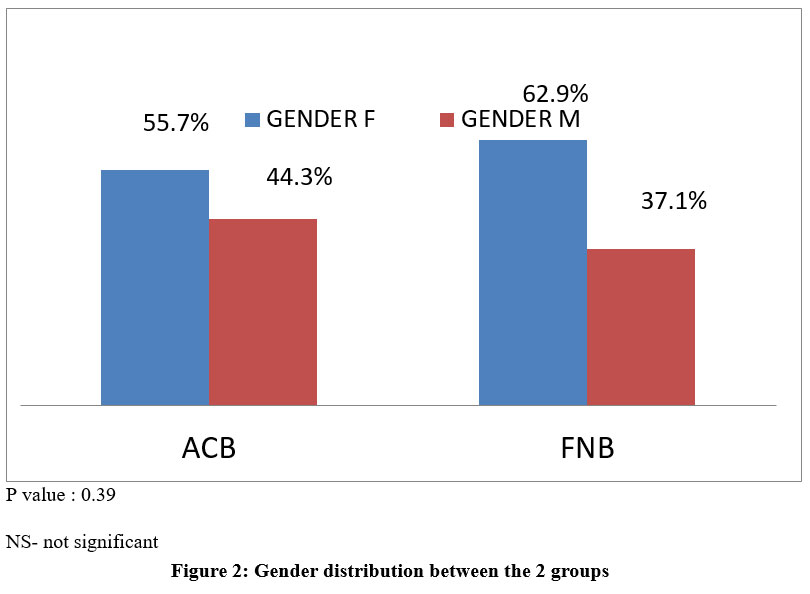 |
Figure 2: Gender distribution between the 2 groups. |
The Mean intraoperative and postoperative HR (Heart rate) among the 2 group showed statistical significance at 2, 4 and 6 hours postoperatively ( p = 0.000; 0.001 and 0.04 respectively ) (Table 2 ).
Table 2 : Mean intraoperative and postoperative Heart rate ( HR ) between the 2 groups .
|
Parameter |
N | Mean | Std. Deviation | 95% Confidence Interval for Mean | t test p value | ||||
| Lower Bound | Upper Bound | ||||||||
| HR | baseline | ACB | 70 | 91.87 | 11.79 | 89.06 | 94.68 | 0.675 |
NS |
| FNB | 70 | 92.74 | 12.74 | 89.70 | 95.78 | ||||
| 5 min | ACB | 70 | 87.66 | 9.86 | 85.31 | 90.01 | 0.382 | NS | |
| FNB | 70 | 89.13 | 9.99 | 86.75 | 91.51 | ||||
| 10 min | ACB | 70 | 81.70 | 9.03 | 79.55 | 83.85 | 0.381 | NS | |
| FNB | 70 | 83.04 | 9.04 | 80.89 | 85.20 | ||||
| 2 hr | ACB | 70 | 79.16 | 10.03 | 76.76 | 81.55 | 0.000 | HS* | |
| FNB | 70 | 86.27 | 10.06 | 83.87 | 88.67 | ||||
| 4 hr | ACB | 70 | 77.30 | 6.32 | 75.79 | 78.81 | 0.001 | HS | |
| FNB | 70 | 82.39 | 11.38 | 79.67 | 85.10 | ||||
| 6hr | ACB | 70 | 81.09 | 6.83 | 79.46 | 82.71 | 0.041 | Sig | |
| FNB | 70 | 84.06 | 9.94 | 81.69 | 86.43 | ||||
| 8hr | ACB | 70 | 78.93 | 7.68 | 77.10 | 80.76 | 0.075 | NS | |
| FNB | 70 | 81.87 | 11.40 | 79.15 | 84.59 | ||||
| 10 hr | ACB | 70 | 78.96 | 7.70 | 77.12 | 80.79 | 0.059 | NS | |
| FNB | 70 | 76.66 | 6.53 | 75.10 | 78.21 | ||||
| 12 hr | ACB | 70 | 76.01 | 8.68 | 73.95 | 78.08 | 0.006 | HS | |
| FNB | 70 | 80.07 | 8.62 | 78.02 | 82.13 | ||||
| 24 hr | ACB | 70 | 80.33 | 6.12 | 78.87 | 81.79 | 0.402 | NS | |
| FNB | 70 | 78.67 | 15.32 | 75.02 | 82.32 | ||||
*HS – Highly Significant
The Mean MAP (Mean Arterial Pressure) among the 2 groups both before and after the respective blocks were statistically significant at the time of block , 5 minutes, 10 minutes, 4 hour , 6 hour and 8 hours. (Table 3).
Table 3: Mean and standard deviation of Mean Arterial Pressure ( MAP ) of the 2 groups.
|
Parameter |
N | Mean | Std. Deviation | 95% Confidence Interval for Mean | t test p value | ||||
| Lower Bound | Upper Bound | ||||||||
|
MAP |
baseline | ACB | 70 | 85.09 | 7.48 | 83.30 | 86.87 | 0.002 | HS |
| FNB | 70 | 89.31 | 8.00 | 87.41 | 91.22 | ||||
| 5 min | ACB | 70 | 80.89 | 9.16 | 78.70 | 83.07 | 0.002 |
HS |
|
| FNB | 70 | 86.07 | 10.52 | 83.56 | 88.58 | ||||
| 10 min | ACB | 70 | 81.16 | 6.65 | 79.57 | 82.74 | 0.000 | HS | |
| FNB | 70 | 90.49 | 6.45 | 88.95 | 92.02 | ||||
| 2 hr | ACB | 70 | 78.63 | 6.92 | 76.98 | 80.28 | 0.731 | NS | |
| FNB | 70 | 79.17 | 11.19 | 76.50 | 81.84 | ||||
| 4 hr | ACB | 70 | 76.66 | 6.27 | 75.16 | 78.15 | 0.000 | HS | |
| FNB | 70 | 81.90 | 9.90 | 79.54 | 84.26 | ||||
| 6hr | ACB | 70 | 79.51 | 6.44 | 77.98 | 81.05 | 0.004 | HS | |
| FNB | 70 | 76.16 | 7.01 | 74.49 | 77.83 | ||||
| 8hr | ACB | 70 | 78.59 | 5.51 | 77.27 | 79.90 | 0.014 | Sig* | |
| FNB | 70 | 81.81 | 9.29 | 79.60 | 84.03 | ||||
| 10 hr | ACB | 70 | 78.36 | 5.96 | 76.94 | 79.78 | 0.862 | NS | |
| FNB | 70 | 78.53 | 5.68 | 77.17 | 79.88 | ||||
| 12 hr | ACB | 70 | 79.73 | 6.11 | 78.27 | 81.18 | 0.818 | NS | |
| FNB | 70 | 79.49 | 6.33 | 77.98 | 80.99 | ||||
| 24 hr | ACB | 70 | 81.39 | 5.43 | 80.09 | 82.68 | 0.000 | HS | |
| FNB | 70 | 86.97 | 7.25 | 85.24 | 88.70 | ||||
*Sig – Significant
The VAS scores between the 2 groups were comparable both before and after administration of the respective blocks (‘t’ test p values > 0.05 (Table 4 ).
Table 4: VAS scores at various time intervals post administration of the block.
|
Parameter |
N | Mean | Std. Deviation | 95% Confidence Interval for Mean | t test p value | ||||
| Lower Bound | Upper Bound | ||||||||
| VAS | baseline | ACB | 70 | 8.54 | 0.56 | 8.41 | 8.68 | 0.900 | NS |
| FNB | 70 | 8.56 | 0.77 | 8.37 | 8.74 | ||||
| 5 min | ACB | 70 | 7.04 | 0.86 | 6.84 | 7.25 | 0.603 |
NS |
|
| FNB | 70 | 7.13 | 1.08 | 6.87 | 7.39 | ||||
| 10 min | ACB | 70 | 5.99 | 0.63 | 5.84 | 6.13 | 0.270 | NS | |
| FNB | 70 | 5.84 | 0.88 | 5.63 | 6.05 | ||||
| 15 min | ACB | 70 | 4.41 | 0.73 | 4.24 | 4.59 | 0.754 | NS | |
| FNB | 70 | 4.46 | 0.88 | 4.25 | 4.67 | ||||
| 2 hr | ACB | 70 | 1.04 | 0.75 | 0.86 | 1.22 | 0.261 | NS | |
| FNB | 70 | 1.19 | 0.75 | 1.01 | 1.36 | ||||
| 4 hr | ACB | 70 | 3.06 | 0.98 | 2.82 | 3.29 | 0.587 | NS | |
| FNB | 70 | 2.97 | 0.88 | 2.76 | 3.18 | ||||
| 6hr | ACB | 70 | 3.36 | 0.90 | 3.14 | 3.57 | 0.658 | NS | |
| FNB | 70 | 3.43 | 1.00 | 3.19 | 3.67 | ||||
| 8hr | ACB | 70 | 4.53 | 0.93 | 4.31 | 4.75 | 0.927 | NS | |
| FNB | 70 | 4.51 | 0.91 | 4.30 | 4.73 | ||||
| 10 hr | ACB | 70 | 5.23 | 0.78 | 5.04 | 5.42 | 0.769 | NS | |
| FNB | 70 | 5.27 | 0.93 | 5.05 | 5.49 | ||||
| 12 hr | ACB | 70 | 5.84 | 0.69 | 5.68 | 6.01 | 0.217 | NS | |
| FNB | 70 | 6.01 | 0.92 | 5.79 | 6.23 | ||||
| 24 hr | ACB | 70 | 6.81 | 0.64 | 6.66 | 6.97 | 0.713 | NS | |
| FNB | 70 | 6.86 | 0.73 | 6.68 | 7.03 | ||||
The average time taken by participants to request for analgesia were 8.14 ± 0.92 (7.92-8.36) hours in the ACB group and 6.49 ± 1.32 (6.18-6.81) hours in the FNB group ( Table 5).
Table 5: Mean Time ( hours ) for rescue analgesia as requested by the patient.
| N | Mean | Std. Deviation | 95% Confidence Interval for Mean | t test p value | ||||
| Lower Bound | Upper Bound | |||||||
| Postop Time ( hr ) for rescue analgesia | ACB | 70 | 8.14 | 0.92 | 7.92 | 8.36 | 0.000 |
HS |
| FNB | 70 | 6.49 | 1.32 | 6.18 | 6.81 | |||
The Average time taken by the participants to have active movements in their operated limb in the ACB group was 4.23 ± 0.90 hours (4.01-4.44 hours) while it was 7.06 ± 7.04 ( 5.38-8.73) hours in the FNB group.( Table 6 ).
Table 6: Mean Time ( in hours ) for postoperative ambulation between the 2 groups.
| N | Mean | Std. Deviation | 95% Confidence Interval for Mean | t test p value | ||||
|
Lower Bound |
Upper Bound |
|||||||
| Postoperative hours of ambulation | ACB | 70 | 4.23 | 0.90 | 4.01 | 4.44 | 0.001 |
HS |
| FNB | 70 | 7.06 | 7.04 | 5.38 | 8.73 | |||
Discussion
Our study demonstrated that the postoperative analgesia provided by ACB was equivalent to that provided by FNB with the added advantages of prolonged duration of action and early ambulation postoperatively.
A previous study comparing ACB and FNB as a part of multimodal postop analgesia following TKA concluded that at six to eight hours post-block, ACB group showed relative sparing of quadriceps strength which was not inferior to FNB in any aspect (23) .
Our study also demonstrated similar results in terms of Postoperative analgesia; both blocks being equally efficacious, Reduced analgesic requirement in the patients who received ACB and early ambulation postoperatively.
Another randomized controlled study compared the effect of ACB and FNB on the early postoperative course following total knee arthroplasty concluded that ACB may promote early ambulation after total knee arthroplasty without decrease in analgesia demonstrated by their ability to perform TUG test and 10 minute walk test on Postoperative day 1 & 2 (17)
The post-operative time taken by patients with ACB were shorter in our study when compared to those who received FNB.
Another recent study compared the pain control offered by ACB with that of FNB following anterior cruciate ligament reconstruction concluded that in those patients who received ACB required lesser analgesia but greater quadriceps strength (29).
However our study subjects were those who underwent TKA, contrary to the study mentioned those who received ACB were seen to ambulate earlier with similar analgesia when compared to those who received FNB.
A previous study that evaluated the postop analgesic efficacy of ACB and FNB after TKA showed that there were no differences in VAS score at rest or ambulation, quadriceps strength, the duration of hospital stay and postoperative nausea and vomiting (30).
Similar to this study, the VAS scores of our study subjects post administration of the block were not statistically different . However , contrary to this study , it was noted that those who received Adductor canal block ambulated earlier and had prolonged analgesia which can be attributed to the addition of Dexmedetomidine to our local anaesthetic solution .
In a previous study on volunteers those who received ACB reported early ambulation in the postoperative period and the analgesic effect was comparable to that of FNB (31) .
This finding in our study were similar to that of previous studies that deduced the ACB was comparable to that of FNB with added advantage of maintaining muscle strength enabling the patients to ambulate earlier
Another randomized control study conducted on 12 healthy volunteers regarding effect of ACB and FNB on quadriceps weakness concluded that FNB reduced the quadriceps strength by 49% as compared to the 8% reduction produced by adductor canal block demonstrating decreased ability to ambulate (24)
Our study also showed similar results as the ACB group ambulated earlier implying greater quadricep strength compared to the FNB group similar to other previous studies (32)
In conclusion ACB with Dexmedetomidine provides longer duration of analgesia, early postoperative ambulation and is equally efficacious as FNB with Dexmedetomidine in patients undergoing knee arthroplasty.
Limitations of the study
VAS score being subjective hence could not be completely reliable. The probability of spinal anaesthesia interfering with study outcomes could not be ruled out which are the limitations of this study. Future scope would be doing the surgeries solely on peripheral nerve blocks.
Acknowledgement
We are extremely thankful to Kasturba Medical College, Mangaluru & Manipal Academy of Higher Education, Manipal, Karnataka, India for their support and guidance in conducting this study.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Funding Sources
there is no funding Source.
References
- Grosu I, Lav and ‘homme P, Thienpont E. Pain after knee arthroplasty: an unresolved issue. Knee Surg Sports Traumatol Arthrosc. 2014;22(8):1744e1758.
CrossRef - Liu SS, Buvanendran A, Rathmell JP, et al. Predictors for moderate to severe acute postoperative pain after total hip and knee replacement. Int Orthop.2012;36(11):2261e2267
- Gaffney CJ, Pelt CE, Gililland JM, Peters CL. Perioperative pain management in hip and knee arthroplasty. Orthop Clin North Am. 2017;48(4):407e419.
CrossRef - Jiang J, Teng Y, Fan Z, Khan MS, Cui Z, Xia Y .The efficacy of periarticular multimodal drug injection for postoperative pain management in total knee or hip arthroplasty. J Arthroplasty.2013 28:1882–1887
CrossRef - Fowler SJ, Symons J, Sabato S, Myles PS. Epidural analgesia compared with peripheral nerve blockade after major knee surgery: a systematic review and meta-analysis of randomized trials. BJA 2008 ;100:154–164
CrossRef - Gerrard AD, Brooks B, Asaad P, Hajibandeh S, Hajibandeh S. Meta-analysis of epidural analgesia versus peripheral nerve blockade after total knee joint replacement. Eur J Orthop Surg Traumatol. 2017;27(1):61e72
CrossRef - Paul JE, Arya A, Hurlburt L, Cheng J, Thabane L, Tidy A, Murthy Y Femoral nerve block improves analgesia outcomes after total knee arthroplasty: a meta-analysis of randomized controlled trials. Anesthesiology 2010;113:1144–62
CrossRef - Sharma S, Iorio R, Specht LM, Davies-Lepie S, Healy WL Complications of femoral nerve block for total knee arthroplasty. Clin Orthop Relat Res. 2010; 468:135–40. ,
CrossRef - Wasserstein D, Farlinger C, Brull R, Mahomed N, Gandhi R . Advanced age, obesity and continuous femoral nerve blockade are independent risk factors for inpatient falls after primary total knee arthroplasty. J Arthroplast. 2013 ; 28:1121–4
CrossRef - Burckett-St Laurant D, Peng P, Giron Arango L, et al. The nerves of the adductor canal and the innervation of the knee: an anatomic study. Reg Anesth Pain Med. 2016;41(3):321e327
CrossRef - Leung P, Dickerson DM, Denduluri SK, et al. Postoperative continuous adductor canal block for total knee arthroplasty improves pain and functional recovery: a randomized controlled clinical trial. J Clin Anesth. 2018;49(Sep):46e52
CrossRef - Enstrup, M. T., Jæger, P. ,Lund, J. , Fomsgaard, J. S., Bache, S. , Mathiesen, O. , Larsen, T. K. And Dahl, J. B. . adductor canal blockade for TKA. Acta anaesthesiolscand 2012; 56: 357-364
CrossRef - Thacher RR, Hickernell TR, Grosso MJ, et al. Decreased risk of knee buckling with adductor canal block versus femoral nerve block in total knee arthroplasty: a retrospective cohort study. Arthroplast Today.2017;3(4):281–285
CrossRef - Zhao XQ, Jiang N, Yuan FF, Wang L, Yu B. The comparison of adductor canal block with femoral nerve block following total knee arthroplasty: a systematic review with meta-analysis. J Anesth. 2016;30(5):745e754
CrossRef - Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M . In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. J Arthroplasty 2012; 27(823–828):e821
CrossRef - Zuo W, Guo W, Ma J, Cui W. Dose adductor canal block combined with local infiltration analgesia has a synergistic effect than adductor canal block alone in total knee arthroplasty: a meta-analysis and systematic review. J Orthop Surg Res. 2019;14(1):101
CrossRef - Hegazy N, Sultan S. Comparison between effects of adductor canal block and femoral nerve block on early postoperative course in total knee arthroplasty: A prospective double-blind, randomized controlled study. Ain-Shams J Anaesthesiol. 2015;8(1):124
CrossRef - Patterson ME, Bland KS, Thomas LC, et al. The adductor canal block provides effective analgesia similar to a femoral nerve block in patients undergoing total knee arthroplasty – a retrospective study. J Clin Anesth 2015;27:39–44
CrossRef - Elkassabany NM, Antosh S, Ahmed M, et al. The risk of falls after total knee arthroplasty with the use of a femoral nerve block versus an adductor canal block: a double-blinded randomized controlled study. Anesth Analg 2016;122(5):1696.
CrossRef - Shah NA, Jain NP. Is continuous adductor canal block better than continuous femoral nerve block after total knee arthroplasty? Effect on ambulation ability, early functional recovery and pain control: a randomized controlled trial. J Arthroplasty 2014;29(11):2224.
CrossRef - Grevstad U, Mathiesen O, Valentiner LS, et al. Effect of adductor canal block versus femoral nerve block on quadriceps strength, mobilization, and pain after total knee arthroplasty: a randomized, blinded study. Reg Anesth Pain Med 2015;40(1):3.
CrossRef - Li D, Ma GG. Analgesic efficacy and quadriceps strength of adductor canal block versus femoral nerve block following total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2016;24(8):2614.
CrossRef - Kim DH, Lin Y, Goytizolo EA, Kahn RL, Maalouf DB, Manohar A, et al. Adductor Canal Block versus Femoral Nerve Block for Total Knee Arthroplasty. Anesthesiology [Internet]. 2014;120(3):540–50
CrossRef - Pia Jæger, Zbigniew J.K. Nielsen, Maria H. Henningsen, Karen Lisa Hilsted, Ole Mathiesen, Jørgen B. Dahl; Adductor Canal Block versus Femoral Nerve Block and Quadriceps Strength: A Randomized, Double-blind, Placebo-controlled, Crossover Study in Healthy Volunteers. Anesthesiology 2013; 118:409–415
CrossRef - Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand 2011; 55:14–19
CrossRef - Thapa D, Ahuja V, Pandey K, Gombar S, Gupta R. Evaluation of analgesic efficacy of dexmedetomidine as adjuvant with ropivacaine in ultrasound-guided adductor canal block in patients following anterior cruciate ligament reconstruction surgeries. Vol. 13, British Journal of Pain. 2019:91–8
CrossRef - Kumar H, Tripathi A, Somvanshi M. Efficacy of dexmedetomidine as an adjuvant to ropivacaine in femoral nerve block for acute pain relief in patients with fracture of femoral shaft and neck. Indian J Pain. 2018;32(2):86
CrossRef - Abdulatif M, Fawzy M, Nassar H, Hasanin A, Ollaek M, Mohamed H. The effects of perineural dexmedetomidine on the pharmacodynamic profile of femoral nerve block: adose-finding randomised, controlled, double-blind study. Anaesthesia. 2016;71(10):1177–85.
CrossRef - El Ahl M. Femoral nerve block versus adductor canal block for postoperative pain control after anterior cruciate ligament reconstruction: A randomized controlled double blind study. Saudi J Anaesth. 2015;9(3):279
CrossRef - Dong CC, Dong SL, He FC. Comparison of Adductor Canal Block and Femoral Nerve Block for Postoperative Pain in Total Knee Arthroplasty: A Systematic Review and Meta-analysis. Medicine (Baltimore). 2016;95:12
CrossRef - Kwofie MK, Shastri UD, Gadsden JC, et al. The Effects of Ultrasound-Guided Adductor Canal Block Versus Femoral Nerve Block on Quadriceps Strength and Fall Risk: A Blinded, Randomized Trial of Volunteers . Regional Anesthesia & Pain Medicine 2013;38:321-325
CrossRef - Mudumbai, S.C., Kim, T.E., Howard, S.K. et al. Continuous Adductor Canal Blocks Are Superior to Continuous Femoral Nerve Blocks in Promoting Early Ambulation After TKA. Clin Orthop Relat Res. 2014; 472, 1377–1383 .
CrossRef

