
Manuscript accepted on :28-05-22
Published online on: 30-06-2022
Plagiarism Check: Yes
Reviewed by: Dr. Swastika Maity
Second Review by: Dr. Sharad Kamble
Final Approval by: Dr. Omar M. E. Abdel-Salam
Nishad Kassim*, Monalisa Pattnaik, Patitapaban Mohanty and Mary Kavi
Swami Vivekanand National Institute of Rehabilitation Training and Research, Olatpur, Cuttack, Odisha, India.
Corresponding Author E-mail: kassim.nishad@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2404
Abstract
Abstract Background: Functional gait training in cerebral palsy can involve over ground gait training or treadmill-based gait training which incorporates partial body weight support (PBWS) system. Insufficient clinical evidence prevails to recommend the superiority over the other intervention. ICF model has created a paradigm shift in understanding motor learning mechanisms, with the use of repetitive, task-specific movements beneficial to restructuring motor pathways. Objective: The primary aim of the study was to compare the effect of integrated task oriented Body Weight Supported overground Training (BWSOGT) against the Body Weight Supported Treadmill Training (BWSTT) and the conventional gait training protocols to improve the functional mobility in Cerebral Palsy. Methods: A Single-blinded, randomised control design. Sixty-children with GMFCS Level of III, IV were recruited in the study with an age ranges between 4 to 14 years (mean age = 9). Participants were randomly assigned into three groups using simple randomisation method with 20 subjects in each group for 8 weeks. The training programme consists of Group A with 40% of body weight supported walker with overhead pulley system which allows multiple degrees of freedom. Body weight- supported treadmill training (Group B) in a closed environment and conventional gait protocol using standard walkers (Group C). Outcome measures: Gross Motor Function Measure dimension-88 (GMFM-88) score. Gait kinematics (Stride length, Step length, Cadence) and 10 meter walk test. Tukey’s Post Hoc for group and time interactions, Krushkal Wallis test for overall significance and Mann Whitney’s U test to compare the significance between the groups. Results: BWSOGT group showed significance over the BWSTT and Control group in GMFM score with p = 0.000 p = 0.002, respectively. Step length of gait parameter remained unchanged in all the three groups. Conclusions: Integrated task oriented BWSOGT might be an effective intervention to improve functional ambulation in children with spastic cerebral palsy due to the usage of a context specific environment and the training protocol.
Keywords
BWS Over Ground Training; GMFM; Gait Parameters; NDT; Task Oriented Training; Treadmill Training
Download this article as:| Copy the following to cite this article: Kassim N, Pattnaik M, Mohanty P, Kavi M. Comparison of Integrated Task Oriented Bodyweight Supported Overground Training with Body-Weight Supported Treadmill Training to Improve Functional Mobility in Children with Spastic Diplegic Cerebral Palsy - A Single Blinded Randomized Control Trial. Biomed Pharmacol J 2022;15(2). |
| Copy the following to cite this URL: Kassim N, Pattnaik M, Mohanty P, Kavi M. Comparison of Integrated Task Oriented Bodyweight Supported Overground Training with Body-Weight Supported Treadmill Training to Improve Functional Mobility in Children with Spastic Diplegic Cerebral Palsy - A Single Blinded Randomized Control Trial. Biomed Pharmacol J 2022;15(2). Available from: https://bit.ly/3bETiOw |
Introduction
Cerebral palsy [CP] is defined as the permanent and non-progressive disorders of the developing brain resulting in disorders of posture and movement1.The worldwide incidence of CP is approximately 2 to 2.5 cases per 1000 live births. In India, it is estimated at around 3 cases per 1000 live births; however, being a developing country the actual figure may be much higher than probable figures. There are about Twenty-five hundred thousand CP children in India as per the available statistical information2.
The Gait pattern is altered in individuals with spastic diplegia due to increase in muscle tone causing scissoring pattern of lower limbs3. The delicate integration of vision, vestibular system, and proprioception has jeopardised the entire locomotion in children affected with CP4. The neuromuscular dysfunction in spastic diplegia includes, loss of selective motor control, altered muscle tone, leading to an imbalance between agonist and antagonist muscles. In addition; they have significant coordination disorders and motor planning difficulties5. In recent years, gait training on a treadmill has been used in the treatment of children with CP aiming to enhance postural stability. Treadmill training is believed to improve postural control by allowing multiple repetitions of the gait cycle in a rhythmic pattern, thereby improving synchronization between agonist and antagonist muscles and thus resulting in improved static and dynamic balance6.
Improvement in the mobility function has been an important concept in the recent rehabilitation approaches7. Motor theory suggests that the best way to improve a motor skill is to conduct a context specific repetitive task training8. Modern concept of motor learning indicates that the training is most effective; when a training activity is most specific to the intended outcome9. The optimal improvement in function will occur as a result of precise and structured training programme10.
Currently partial body-weight-supported treadmill training [PBWSTT] has been more widely used in rehabilitating people with neurological conditions. The available literatures, either has insufficient sample size or lack of randomisation in the study.
There are limited evidences towards the effect of robotic and treadmill training in the field of paediatric rehabilitation especially for children with central motor dysfunction11. There are several studies which reported the superiority of over-ground gait training above the treadmill training with effectiveness of task oriented training for functional recovery in cerebral palsy children12.
Body weight-supported training over level ground is affordable. This is predominantly important consideration for the low and middle-income countries. The current study is focusing on evaluating the efficiency of an integrated task-oriented BWSOGT over the BWSTT and the conventional over ground training.
Aims and objectives
Our study aims at comparing the effect of integrated task oriented body weight supported over ground training [BWSOGT] over the body weight supported treadmill training [BWSTT] and the conventional gait training protocols to improve the functional mobility in Cerebral Palsy.
Methodology
A Single-blinded (Assessor) Randomised Control Trial with 60 children recruited from the paediatric rehabilitation unit; Department of Physiotherapy; SVNIRTAR. The children were included after signing the informed consent forms by the parents, and the study was approved as per Helsinki ethical declaration. Age group ranged from 4 years to 14 years (with mean age 9); divided into three groups with 20 subjects in each group, namely BWSOGT group [mean age 8.75], BWSTT [mean age 8.10] and conventional group [mean age 8.45] 66.7% of subjects were males & 33.3 % of subjects were females. The children were randomised using a simple random sampling method and allocated sequentially in to group A, B and C respectively using chit paper method.
Inclusion criteria
Children diagnosed as spastic diplegic CP, whose age range between 4 to 14 years with GMFCS level III to IV. Participant should be able to follows instructions and independent in standing with aids.
Exclusion criteria: Children with the following were excluded. Intellectual Disability, epileptic attack in past 6 months, hemiplegic, athetoid, ataxic, and flaccid CP, cardio vascular illness, visual and cognitive deficits, under another gait training protocol, congenital musculoskeletal defects, dislocations of hip, significant hip and knee contractures, behavioural disorders, recent botulinum toxin injections.
Dependent Variables
Gross Motor Function Measure dimension [GMFM-88] score, Gait kinematics [Stride length, Step length, Cadence], 10 meter walk test [self-dependent and fast velocity].
Instrumentation
BWSOGT
It’s a custom made walker system; attached four wheels with brake facility. Dimension of the walker is 160 x 53 [LXB]. The walker frame has a suspension system with adjustable overhead- pulley through which a string is introduced. One end of the string is attached with the suspension harness; whereas the other end attached to a removable weighted system which allows addition and removal of the weights.
 |
Figure 1: Ramp Training. |
 |
Figure 2: Balancing. |
 |
Figure 3: Overhead Throw. |
BWSTT
The Tech-Med; Physio200model treadmill was used in this study.
Running surface: 53 x150 cm, Speed range: 0.1 to 10 km/h, Inclination: level 6. Partial body weight support system: Tech med body weight support system which works with a hydraulic lift system with a total lift capacity of 200 kg.
 |
Figure 4: Treadmill was used. |
Control group: Standard walking frame.
Procedure
Subjects who met the inclusion criteria were screened using GMFCS and were randomly allocated in to three groups A, B, and C respectively. All participants underwent an initial baseline assessment of Gross Motor Function Measure, Gait kinematics including cadence, step length, stride length, and the 10 Meter Walk test. Participants in all three groups were subjected to the regular NDT protocol; which included functional stretching, task oriented activities for trunk control and balance. The gait training for the participants were performed using the specific interventions like BWSOGT, BWSTT, Conventional gait training using parallel bars and walkers in group A, B, C respectively. The intervention period was of 8 weeks duration, 3 days/week, 30 minutes/session.
Group A: Body Weight Support Overground Training
The participants of this group were initially trained with the modified walker. Initially, 40% of the participant’s bodyweight was added through weights to the pulley system. Knee flexion during the stance phase of walking was used as an indication for increasing the weight support, and heel off during the stance phase as an indication for reducing the weight support. Gait efficiency was checked by allowing a trial walk of 10 meters to adjust the weight support if required. Participants were allowed to walk at their self-selected speed; which eliminated the need of manual assistance of legs during the training. The assistance of one person was required to progress the suspension frame for those who had limited ability to propel the suspension frame. The subjects were directed to perform certain activities like picking up ball from the ground and pass the ball to care taker, kicking the ball, obstacle clearance, stepping over a small foot stool.
Group B: Body weight-supported treadmill training
Participants in Group B were trained on a body weight supported treadmill. Gait efficiency was checked by allowing them to walk for one minute in order to adjust the weight support. Manual guidance of the legs was provided until independence in stepping was achieved. Inclination of the treadmill was altered as a progression in order to equalize the difficulty level in all the groups.
Group C: Conventional gait training
The participants of this group after the regular therapy session were provided with gait training using standard walking frames and parallel bars. Walking experiences were naturalized, except that the body was suspended and addition of a task to enrich the learning experience. The subjects were allowed to use the orthosis during the training session.
After completion of 8 weeks all participants received follow up assessments of Gross Motor Function Measure, gait kinematics[stride length, step length, cadence], 10MWT.
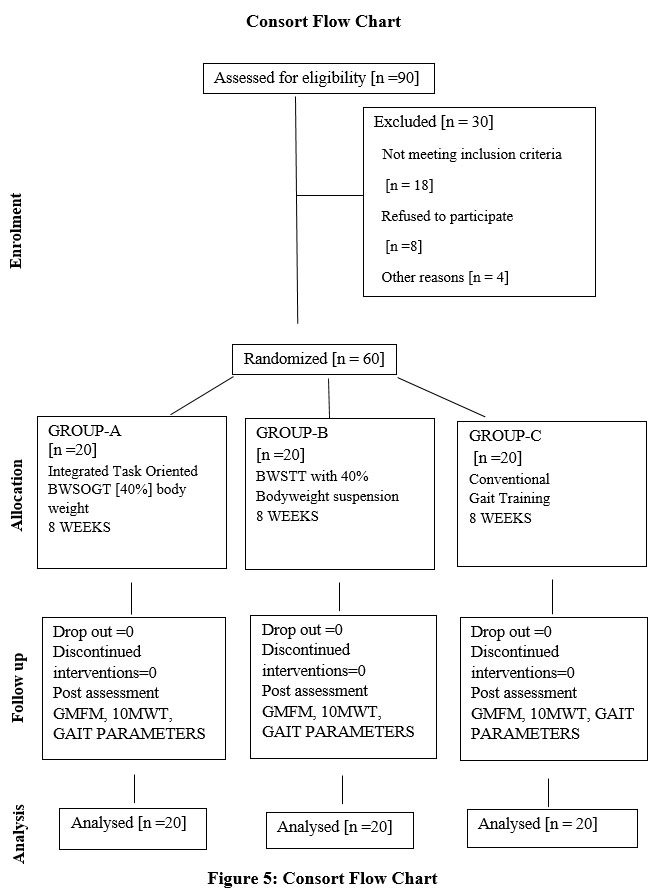 |
Figure 5: Consort Flow Chart |
Data Analysis
Statistical analysis was performed using SPSS version 23.0.
The Gait kinematics [Stride length, Step length, Cadence] and 10MWT were analysed using a [GLM] General Linear Model ANOVA, 2×3 with 2 as a time factor and 3 as a group factor. There was one between factor [group] with three levels [Groups: A, B and C] and one within factor [time] with two levels [time: Pre and Post]. All pair wise, post – hoc comparisons were analysed using a 0.05 level of significance.
The change in function post to pre between the groups, as the data followed a positively skewed curve and falls under non normative distribution. Krushkal Wallis test was used to determine the overall difference between the groups. The effect between the groups were analysed with Mann-Whitney U test by calculating the median of GMFM-88 [post minus pre scores]. Separate comparisons between the groups were obtained and tabulated.
Results
Demographics
A total number of 60 subjects with mean age 6.3 were taken & divided into three groups with 20 subjects in each group, namely BWSOGT [mean age 8.75] & BWSTT [mean age 8.10] and conventional group [mean age 8.45]. 66.7% of subjects were males & 33.3% of subjects were females.
1OMWT
There was a significant improvement in scores for all the three groups from pre to post-test measurements. However, the BWSOGT group showed greater improvement than BWSTT and Control group. There was no significance between BWSTT and control group at the end of 8 weeks intervention.
Gait Kinematics
Stride Length Left
There was a significant improvement in stride length scores for all the three groups from pre to post-test measurements. However, the BWSOGT group showed significantly greater improvement than BWSTT and Control group. There was no significance between BWSTT and control group at the end of 8 weeks of intervention.
Stride Length Right
There was a significant improvement in stride length score for all the three groups from pre to post-test measurements. BWSOGT group showed significantly greater improvement than BWSTT and Control group. There was no significance between BWSTT and control group at the end of 8 weeks of intervention
Step Length
There was a clinical significance; on the contrary it failed to register statistical significance between the groups and within the group.
Cadence
There was a significant improvement in cadence score for all the three groups from pre to post-test measurements. However, the BWSOGT group showed significantly greater improvement than BWSTT and Control group. BWSTT had significance over control group at the end of 8 weeks of intervention.
Gross Motor Function Measures Goal Area-[GMFM -88]
A Kruskal-Wallis test was conducted to determine whether the GMFM score remain same in all three groups or they had variability among the performance after the intervention across the groups. Results of that analysis indicated that there was significance difference in GMFM Goal area function between the 3 groups with H= [2] =15.412 and p=0.000.
Gross Motor Function Measures Goal Area – [GMFM -88]
BWSOGT had statistical significance over the BWSTT and the control, BWSTT had significance over the control group.
Discussion
The overall result of this study showed that all the three groups [Body weight supported Over ground training, Body weight supported treadmill training and Conventional gait training] had statistical significance in terms of Gross Motor Function Measure, cadence, stride, and 10 MWT from pre to post-test measurements. However, Step length parameter has showed no significance in all the three groups. From the present synthesis of data in our study comparing all three groups BWSOGT group with BWSTT showed a large effect on GMFM, while BWSIT showed better improvement than Conventional group.
Walking velocity and gait kinematics
On comparing inter-group on walking velocity using 10MWT showed significance in all three groups. BWSOGT had a difference of 13.47%, 13.51% self-selected velocity when compared to the other two groups. While, BWSTT compared to the control group had a difference of 0.04% velocity.
Similarly on inter-group comparison BWSOGT had a difference of 9.99%, 14.65% in cadence, 7.67% to 8.6% in stride length and 1.31% – 0.2% in step length. Whereas, BWSTT had a difference of 4.12 % cadence, 1.25% stride length, 1.31% step length when compared to the control group.
The improvement in the control group may be attributed to practice in the natural environment. On the other hand, they had minimal opportunity for exploring environment due to holding the walker. It was also noted; children were unable to complete the session, often take a break or discontinue the session which decreased the repetitive training protocol. Decreased degree of freedom due to the necessity of holding the walker also contributed to the poor sustainability13.
The improvement in the BWSTT group could be because of the repetitive training pattern. Moreover, the constant speed and the moving platform provided a trigger to initiate the ambulation. This allowed the children to improve the gait parameters which could be another reason for the fast velocity. The training would have enabled the development of the Central Pattern Generators. Over ground gait velocity increased post adaptation due to increased stride length and decreased stride duration after motor adaptation during treadmill walking14.
The treadmill provides an objective measurement of speed and a precise measurement of distance, which can be quantified and progressed. Although over ground walking allows the participant to practice the target skill, it is difficult for the individual to maintain a consistent speed over longer distances15.
Our results suggested that the faster walking speeds may have been accomplished after the BWSOGT training by increasing the cadence. Motor theory suggests the best way to improve a motor skill is repetitive practice. BWSOGT also has advantages over treadmill training by preparing patients for walking in the real-life environments16. During treadmill locomotion with body weight-support, the ground moves relative to the person but the visual surround remains the same. In the real-world, a person moves relatively to the ground and the visual surroundings17.
The control group and the BWSTT group were not provided with the task-oriented skill training, which would have lowered the motivation than the BWSOGT group.
It’s well established, that task- oriented programmes are necessary for motor learning to occur and functional reorganisation. Therefore, optimal training effect occurs; when the training is similar to that of the real-life task18,19.
There was a common phenomenon that occurred in all the three groups. In our study, it was observed there is clinical significance in step length. However, the interventions failed to register as statistically significance. This could be because in diplegic CP both the lower limbs were equally involved and spasticity would have restricted the smooth movement of the limbs. Spasticity causes wide range of ambulatory disorders which explains the individual difficulties in maintaining and restores both the static and dynamic balance20. There is a strong relationship between balance and single leg support time, which indicated as a test to measure the upright postural stability after upper motor neuron lesion21.
The use of the treadmill imposes a different context altering propulsion and balance patterns22. Individual must apply sufficient force toward the floor to propel limbs forward. On a treadmill, the propulsion generated by the limbs is not necessarily proportional to velocity23,24, as the belt allows for the limbs to passively move with the minimized levels of muscle activation25,26. CP children may adopt a different strategy in balance control, as they would adopt while walking over- the ground. The functional anticipatory postural actions may be substantially preserved in CP27.
The anticipatory postural actions are considered to be an essential factor in the postural adaptations. In case of the treadmill, training over the moving platform applies a constant demand on the subject for propulsion, where the subject is not prepared for the specific action and cause a poor learning experience with regards to the initiation factor. This demand might increase the abnormal muscle activation in the subjects. A sustained stretching pattern is believed to reduce the spasticity in the central motor dysfunctions, or any voluntary motor initiation is necessary for the proper sequenced activation of the muscles.
BWSOGT training might subtly have modulated the recruitment patterns and the anticipatory adjustment patterns. On comparing the suspension over ground system with treadmill training, BWSOGT provides more functional performance, by providing both the trigger for walking and lateral shift. The moving platform of the treadmill helps in the initiation of the gait and provides a shift of equilibrium. However, it lacks lateral weight shift.
Gross Motor Function Measure
Our results showed that BWSOGT had 5.7%, 6.49% of GMFM functional score when compared to the other two groups. BWSTT had 0.79% better performance when compared to control group.
The significance could be because of the task-specific motor activities, in comparison with the traditional activities, resulted in long-lasting cortical reorganisation specific to corresponding area being used during practice28,29, recent evidences has shown the task oriented interventions are effective strategies to promote meaningful motor response30.
BWSTT group had a repetitive gait pattern using partial body weight gait training, which assists them in mobility increased the children motivation and participation. The games and the activities incorporated were a real-life task. The participants were devoid of the manual support, which provided a better learning opportunity and the trigger initiated by the moving platform initiated the gait pattern which would have resulted in the cortical reorganisation31.
Generally, children with cerebral palsy deprived with limited environment stimulation that is necessary for learning experiences. Mobility factor plays a major hindrance in these children to become less exploratory and delayed in skills like language development.
BWSOGT system is flexible depends on the subject needs. Based on the progression, the amount of body weight suspended was reduced, which increased the challenges to the participant and leads to a better learning experience. BWSOGT system enabled the subjects to practice the various components of the GMFM -88; maybe this could be the reason for better GMFM scoring in this group.
Our results were similar to a study, that BWSOGT system improves gait speed and cadence. In addition, the article suggests that the influence on gait speed may be because of massed practice. There did not appear to be a significant observable change in gait pattern32.
Table 1: Descriptive Table
| BWSOGT | BWSTT | Conventional | ||||
| Pre-test | Post-test | Pre-test | Post-test | Pre-test | Post-test | |
| 10MWT
(meters) |
0.2[.015] | 0.26[.02] | 0.19[.009] | 0.21[.010] | 0.16[.009] | 0.19[.012] |
| Stride Length Left | 25.4[1.30] | 30.45[1.30] | 24.85[1.20] | 28.[1.17] | 22.95[1.33] | 25.65[1.29] |
| Stride Length Right | 25.7[1.21] | 30.95[1.30] | 24.8[1.11] | 27.85[1.18] | 22.9[1.38] | 25.50[1.38] |
| Step
Length |
11.9[.65] | 14.10[.60] | 11.1[.57] | 13.[.52] | 10.15[.54] | 12.25[.56] |
|
Cadence |
37.3[1.81] | 48.15[2.58] | 35.8[1.85] | 42.35[1.88] | 33.80[1.58] | 38.85[1.82] |
|
In the table – Mean [Standard Error of Mean] |
||||||
Table 2: Post hoc test table
| Post hoc test table | |||
| Time
1,57,0.05 |
Group
2,57,0.05 |
Group x time
2,57,0.05 |
|
| 10MWT | F=46.346, p= 0.000. | F=3.855, p= 0.027. | F=5.321, p=0.027 |
| Step length | F=154.084, p=0.000 | F= 2.595, p= 0.083. | F= 0.281, p=0.756, |
| Stride length left | F=177.957, p=0.000 | F=2.131, p= 0.128 | F=6.991, p=0.002 |
| Stride length right | F=155.951, p=0.000 | F=2.757, p= 0.072 | F= 12.472, p= 0.000. |
| Cadence | F =231.18, p=0.000 | F = 2.853, p= 0.066. | F= 12.472, p= 0.000. |
Table 3: Mann Whitney’s table
| Mann Whitney’s table | |
| BWSOGT(V/S) BWSTT | (Z)=-3.219 (p) = 0.001 |
| BWSTT(V/S) CONTROL | (Z)=-1.447 (p) = 0.148 |
| BWSOGT(V/S) CONTROL | (Z)=-3.327 (p) = 0.001 |
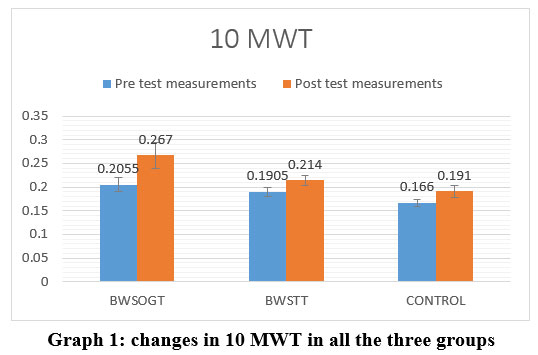 |
Graph 1: changes in 10 MWT in all the three groups |
The BWSOGT group showed greater improvement as compared to the BWSTT and control group.
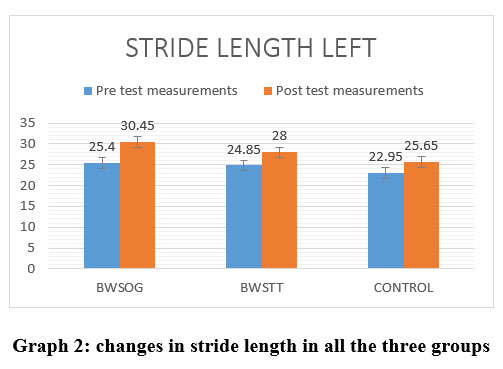 |
Graph 2: changes in stride length in all the three groups. |
The BWSOGT group showed greater improvement as compared to the BWSTT and control group.
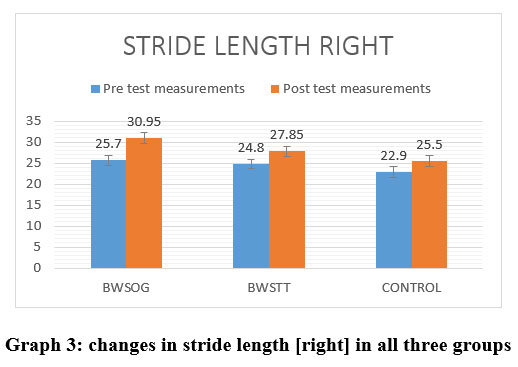 |
Graph 3: changes in stride length [right] in all three groups. |
The BWSOGT group showed greater improvement as compared to the BWSTT and control group.
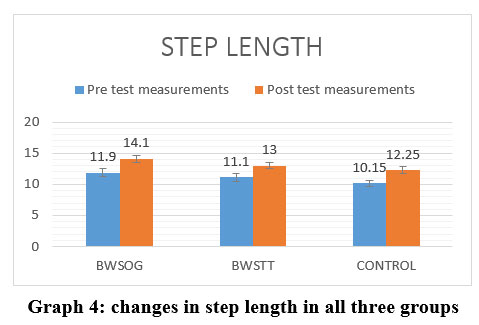 |
Graph 4: changes in step length in all three groups |
Mild improvement in distance covered in step length in all the three groups following treatment for 8 weeks.
 |
Graph 5: changes in cadence in all three groups |
The BWSOGT group showed greater improvement as compared to the BWSTT and control group.
 |
Graph 6: changes in GMFM between the groups |
The BWSOGT group showed greater improvement as compared to the BWSTT and control group
Conclusion
Children with spastic diplegia showed significant improvement in terms of gait parameters and functional performance. BWSOGT followed a training protocol in an open environment like walking in plane, irregular surfaces, ramp and play integrated activities like picking up and passing the ball along with a self-adjusting BWS system. This proves BWSOGT is better than BWSTT in a closed environment and the conventional gait training without BWS system. Conversely, both the training programme was found superior in terms of cadence and gross motor function measure against the open ground unsupported gait training. Few limitations were the subjects were chosen from a similar geographical location. Carry over effect and measure of impairment has not been studied. Energy expenditure index was not calculated for endurance parameter.
Recommendations for future studies
Further studies on clinically possible outcome measures to check endurance in non-ambulant CP. Usage of EMG analysis can be used to detect precise changes in muscle function and advanced investigatory procedures are recommended to prove the neuronal reorganization similar study may be conducted on other CP children.
Clinical utility: Despite the limitations, the results were promising for the clinicians working with CP children. The study emphasizes on the usage of a task-oriented activity based gait training with customised BWSOGT for CP children. BWSOGT system is cost effective; when compared with the expensive treadmill with the partial body weight support system.
Acknowledgement
The author would like to acknowledge all faculties of Swami Vivekanand National Institute of Rehabilitation Training and Research and the parents and children who volunteered to participate in this study. Gratitude’s to my family and Friend Mr. Sankar for their constant moral support.
Conflict of Interest
The author declares no conflict of interest.
Funding Sources
There are no funding source.
References
- Rosenbaum P, Paneth N, Leviton A, et al. A Report: The Definition and Classification of Cerebral Palsy. Dev Med Child Neurol. 2007; 109:8-14
- Incidence of Cerebral Palsy Remains Constant in India on Indian Health News. Available from :http://www.medindia.net/ news/Incidence-of-Cerebral-Palsy-Remains-Constant-in-India-74912-1.htm .cdc.gov
- American Physical Therapy Association, 2001], [“Facts about Cerebral Palsy,” 2015]. https://www.cdc.gov/ ncbddd/HYPERLINK, “https://www.cdc.gov/ncbddd/cp/facts.html”CPHYPERLINK “https://www.cdc.gov/ncbddd/cp/facts.html”/facts.html.
- Nashner LM, Shumway-Cook A, Marin O. Stance posture control in selective groups of children with cerebral palsy: Deficits in sensory organization and muscular coordination. Experimental Brain Research. 1983; 49:393–409.
CrossRef - Shumway-Cook A, Hutchinson S, Kartin D, Price R, Woollacott M. [2003] the effect of balance training on recovery of stability in children with cerebral palsy. Dev Med Child Neurol 45: 591–602
CrossRef - Smania N, Bonetti P, Gandolfi M, Cosentino A, Waldner A, Hesse S, Werner C, Bisoffi G, Geroin C, Munari D: Improved gait after repetitive locomotor training in children with cerebral palsy. Am J Phys Med Rehabil 2011; 90:137Y149.
CrossRef
- H Barbeau and J Flung. The role of rehabilitation in the recovery of walking in the neurological population, Current opinion in neurology, 14[2001], 735-740.
CrossRef - Willoughby KL, Dodd KJ, Shields N, Foley S. Efficacy of partial body weight–supported treadmill training compared with overground walking practice for children with cerebral palsy: a randomized controlled trial. Arch Phys Med Rehabil 2010; 91:333-9.
CrossRef - H I Ma, G A Trombly and C Robinson – Podolski The effect of context of skill acquisition and transfer, American Journal Of Occupational therapy, 53[1999 138-144].
- N A Bayona J Bitensky, K Salter R Teasell, The role of task specific\training in rehabilitation therapy, Top Stroke Rehabilitation,12,[2005] 58-65.
CrossRef - Damiano, D. L., & Abel, M. F. [1998]. Functional outcomes of strength training in spastic cerebral palsy. Archives of Physical Medicine and Rehabilitation, 79[2], 119-125. doi: S0003-9993[98]90287-8].
CrossRef - Effect of Gait Training With Overground Gait Trainer Support Versus Partial Body Weight Supported Treadmill Training in Children with Spastic Diplegic Cerebral Palsy Nia M. Torres, 2015
- Moreau, N. G., Bodkin, A. W., Bjornson, K., Hobbs, A., Soileau, M., & Lahasky, K. (2016). Effectiveness of rehabilitation interventions to improve gait speed in children with cerebral palsy: Systematic Review and Meta-analysis. Physical therapy, 96(12), 1938–1954. https://doi.org/10.2522/ptj.20150401.
CrossRef - Fosdahl, M. A., Jahnsen, R., Kvalheim, K., & Holm, I. (2019). Effect of a combined stretching and strength training program on gait function in children with cerebral palsy, GMFCS Level I & II: A Randomized Controlled Trial. Medicina (Kaunas, Lithuania), 55(6), 250.
CrossRef - DeJong & Damiano, D. L, S. L. [2009]. A systematic review of the effectiveness of treadmill training and body weight support in pediatric rehabilitation. Journal of Neurological Physical Therapy, 33[1], 27–44
CrossRef - Hyun-Kyung Hana, and Yijung Chungb Effects of task-oriented training for Gross Motor Function Measure, balance and gait function in persons with cerebral palsy. Phys Ther Rehabil Sci 2016;5:9-14
CrossRef - Nishi Gupta Rajeev Mehta Comparison of gait performance of spinal cord injury subjects: body weight supported treadmill training versus over ground gait training Apollo Medicine Volume 6, Issue 1, March 2009, Pages 21-27
CrossRef - Lee JH, Sung IY, Yoo JY. Therapeutic effects of strengthening exercise on gait function of cerebral palsy. Disabil Rehabil. 2008; 30[19]:1439-1444.
CrossRef - Kazon S, Grecco LA, Pasini H, Corrêa JC, Christovão TC, de CarvalhoPde T, et al. Static balance and function in children with cerebral palsy submitted to neuromuscular block and neuromuscular electrical stimulation: study protocol for prospective, randomized, controlled trial. BMC Pediatr. 2012; 16:12:53
CrossRef - Johnston TE, Watson KE, Ross SA, Gates PE, Gaughan JP, Lauer RT, Tucker CA, Engsberg JR. Effects of a supported speed treadmill training exercise program on impairment and function for children with cerebral palsy. Dev Med Child Neurol. 2011; 53[8]:742- 750.
CrossRef - Norman, K. E., Pepin, A., Ladouceur, M., & Barbeau, H. [1995]. A treadmill apparatus and harness support for evaluation and rehabilitation of gait. Archives of Physical Medicine and Rehabilitation, 76, 772–778.
CrossRef - Goldberg, E. J., Kautz, S. A., & Neptune, R. R. [2008]. Can treadmill walking be used to assess propulsion generation Journal of Biomechanics, 41, 1805–1808.
CrossRef - Harris-Love, M. L., Macko, R. F., Whitall, J., & Forester, L. W. [2004]. Improved hemiparetic muscle activation in treadmill versus overground walking. Neurorehabilitation and Neural Repair, 18, 154–160.
CrossRef - Han, Y. G., & Yun, C. K. (2020). Effectiveness of treadmill training on gait function in children with cerebral palsy: meta-analysis. Journal of exercise rehabilitation, 16(1), 10–19. https://doi.org/10.12965/jer.1938748.374
CrossRef - Stackhouse C, Shewokis PA, Pierce SR, Smith B, McCarthy J, Tucker C. [2007] Gait initiation in children with cerebral palsy. Gait Posture 26: 301–8.
CrossRef
- Ming Wu,Janis Kim, Pooja Arora, Deborah J. Gaebler-Spira, and Yunhui Zhang Kinematic and EMG Responses to pelvis and leg assistance force during treadmill walking in children with cerebral palsy Neuroplasticity Hindawi Volume 2016 |Article ID 5020348 | https://doi.org/10.1155/2016/5020348
CrossRef - Pavão, S. L., dos Santos, A. N., Woollacott, M. H., & Rocha, N. A. (2013). Assessment of postural control in children with cerebral palsy: a review. Research in developmental disabilities, 34(5), 1367–1375. https://doi.org/10.1016/j.ridd.2013.01.034
CrossRef - J Crompton,C. Imms,A T McCoy M Randall B Eldridge B Scoullar M P Galea, Group based task related training for children with cerebral palsy, A Pilot study, Physical and Occupational Therapy in Paediatrics 2007, 43-65
CrossRef - Papale, A. E., & Hooks, B. M. (2018). Circuit changes in motor cortex during motor skill learning. Neuroscience, 368, 283–297. https://doi.org/10.1016/j.neuroscience.2017.09.010
CrossRef
- Wu, Y. W., Day, S. M., Strauss, D. J., &Shavelle, R. M. [2004]. Prognosis for ambulation in cerebral palsy: a population-based study. Pediatrics, 114[5], 1264-1271. doi: 114/5/1264 [pii]10.1542/peds.2004-0114.
CrossRef
- Kurz MJ, Stuberg W, DeJong S and Arpin DJ. Overground body-weight-supported gait training for children and youth with neuromuscular impairments. Phys OccupTherPediatr 2013; 33: 353–365.
CrossRef
- Wonsetler, E. C., & Bowden, M. G. (2017). A systematic review of mechanisms of gait speed change post-stroke. Part 1: spatiotemporal parameters and asymmetry ratios. Topics in stroke rehabilitation, 24(6), 435–446. https://doi.org/10.1080/10749357.2017.128574
CrossRef

