A Comprehensive Review of Experimental Animal Models of Hepatopathy
 , Sachin Chaudhary2, Abdel-Nasser El-Shorbagi2, Udaivir Singh Sara3, Prashant Shukla3 , Sudhansu Ranjan Swain4, Jagannath Sahoo5 and P. N. Murthy6
, Sachin Chaudhary2, Abdel-Nasser El-Shorbagi2, Udaivir Singh Sara3, Prashant Shukla3 , Sudhansu Ranjan Swain4, Jagannath Sahoo5 and P. N. Murthy6 1Department of Pharmacology, Hygia Institute of Pharmaceutical Education and Research Lucknow, Uttar Pradesh, India
2Department of Medicinal Chemistry, College of Pharmacy, University of Sharjah, Sharjah, United Arab Emirates
3Department of Pharmaceutics, Hygia Institute of Pharmaceutical Education and Research Lucknow, Uttar Pradesh, India
4Department of Pharmacognosy, Moradabad Educational Trust Group of Institutions, Faculty of Pharmacy, Moradabad, Uttar Pradesh, India
5Department of Pharmaceutics, School pf Pharmaceutical and Population Health Information, Dehradun Institute of Technology University, Dehradun, Uttarakhand, India
6Department of Pharmaceutics, Royal College of Pharmacy and Health Sciences, Berhampur, Orissa, India
Corresponding Author E-mail; ram5880@gmail.com
DOI : http://dx.doi.org/10.13005/bpj/2397
Download this article as:
![]()
At this moment, liver dysfunction is a major source of destruction, and its widespreadity is accentuated in the developed republics. The liver is an imperative organ of the body and is involved in metabolism and regulation. The large number of medications, toxins, and plant-derived products has been claimed to cause liver dysfunction, which is potentially life intimidating to humans. Currently, there is a shortfall in encouraging treatment for treating patients with liver dysfunction due to the nonexistence of empathy for gesturing offenders serviceable in the pathogenesis of liver toxicity. Hepatic dysfunction is manifested by hepatic karyopyknotic, eosinophilic or acidophilic cell plasm, followed by excessive steatosis, liver injury, and oxidative degradation of lipids that cause centrilobular necrosis in hepatocytes. Different signaling mechanism, like activation of Kupffer cells, NK cells, inflammatory mediators, and ROS are associated with the pathogenesis of liver dysfunction. A good empathy of chief mechanisms is prerequisite for the scheming of novel curative medications. Consequently, animal models are being developed to impressionist hepatic ailments. From the several decades, researchers are using distinctive animal models for discovering and understanding pathogenesis of hepatic ailments and associated abusiveness. This current review has been framed to discuss numerous new and traditional experimental models for hepatotoxicity studies. Numerous animal models have been evolved to evaluate the pathogenesis and develop drugs for hepatotoxicity. Experimental modes of hepatotoxicity are influential for invention of novel molecular signaling trails for the improvement of human health.
KEYWORDS:Animal model; Hepatotoxicity; Hepatocytes; Kupffer cell; Necrosis; Pathogenesis
Introduction
The liver, an exuberant organ, acknowledged synchronizing gastrointestinal homeostasis and body function in general. Furthermore, it also serves to abruptly withdraw of toxicants. Consequently, the commanding functioning of the liver is imperative for elegant wellness. The inequality between the offensive and shielding services results in disfiguration and disservice to liver and miscellany mechanisms that are responsible for causing hepatic toxicity inclusive of environmental and chemical agents. In acute hepatic dysfunction, fast deterioration of liver occurs without apparent pre-existing continual liver illness, many of them can be reversed when defamatory agents are withdrawn; however, in peculiar exceptional settings a liver transplant is required.1 Drug triggered hepatic impairment is the predominant genesis of liver dysfunctioning in American and European population, computing for around 50% of acute liver dysfunctioning.2 The drug induced liver abrasion (DILA) is non-conventional in Chinese population; however, hepatitis B is the prominent source of chronic hepatic malfunctioning.3 The year-end prevalence amplitude of DILA permutated from 13.9 to 24.0 per 100,000 inhabitants.4 Plenteous of medications resulted in DILA, with distinctive levels of lethalness like drug used against bacterial infection, viral infection, fungal infection, drug against inflammation, anti-gout drugs, drug against ulcer, antidiabetic drugs, anti-tubercular drugs, and anti-cancer agents.5 The overdose of paracetamol is the intrinsic exposition for liver toxicity, far exceeding the other motives, whereas traditional natural remedy predominates as the purpose of DILA in China and Korea.3,6. The liver has more than one functions, so hepatic toxicity deviates from its normal functioning and it additionally rely on the nature of the medication or chemical exposure.7-8,9-26 Hence, for understanding the pathogenesis of DILA, several models are accessible to screen the anti-hepatotoxic endeavor of any substance. Since there are confines of the outcomes in every model, it is important to select special techniques for affirmation of the findings. This miniature review article highlights the hepatopathy models that are being used to observe the activities of liver injuries under hepatotoxic agents with a strong emphasis on examining whether or not the developed fashions are suitable for hepatic fibrosis under quite a number of conditions.
Experimental Animal Models of Hepatotoxicity
Animal models are important tools for determining the pathogenesis or mechanisms of toxicity in biomedical research. They have complexity in both in vivo and in vitro. The creatures as rodents, rabbits, mice, guinea pigs, sheep and monkeys, are used globally conduct an investigation into hepatotoxic footprints. These animals could be utilized to understand the fundamental mechanism of the xenobiotic. However, the experimental animal model is a promising prototype for the drug design and discovery of novel hepatoprotective agents. The summary of modes, pathological manifestation and mechanism of liver hepatopathy has been illustrated in (Table 1).
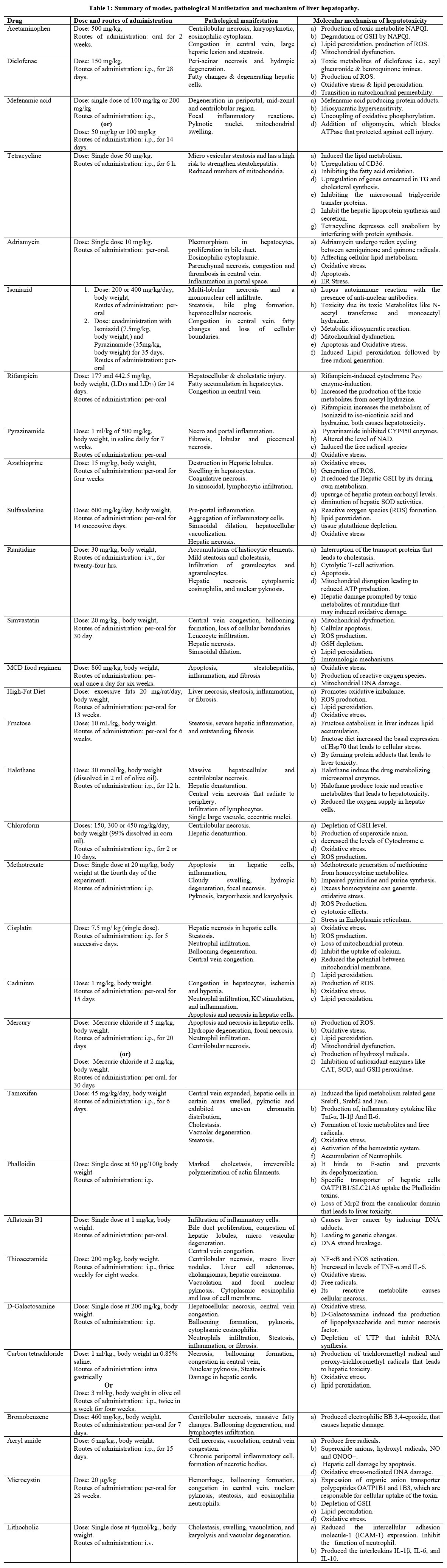 |
Table 1: Summary of modes, pathological Manifestation and mechanism of liver hepatopathy. |
Drug-Induced Hepatotoxicity (Hepatic Abrasion) Model
Non-steroidal anti-inflammatory drug-induced liver abrasion model
Paracetamol (acetaminophen) induced liver abrasion
The ideal therapeutic dose of paracetamol (acetaminophen) is proposed to be safe at regular intervals. However, its overabundance in the body can be observed, leading to liver dysfunction. The excessive dose of paracetamol is primary reason of drug-induced hepatic dysfunctioning in the Americans.27 The over/high dose of paracetamol gave rise to noxiousness of the centrilobular hepatocytes that were characterized by enormous hepatic abrasions. The oxidative product of paracetamol is N-acetyl-P-benzoquinoneimine, which causes decadency of the glutathione level and produces hepatic cellular destructiveness. Administration of paracetamol at dose of 500 mg/kg, for 2 weeks triggers liver abrasion in rats.28
Diclofenac Induced hepatic abrasion
Hepatotoxicity induced by diclofenac is a perfect specimen of idiosyncratic DILA. Diclofenac predominantly associated with the hepatocellular impression of hepatic malfunction. Diclofenac undergoes metabolic conjugation with glucuronidation to form highly unstable acyl glucuronide and acyl glucuronide upon further oxidation by the CYP2C8 enzyme produces 5-hydroxydiclofenac as a metabolic product. Both of these metabolites of diclofenac bind covalently to proteins and form adducts; that potentially expand the threat of hepatotoxicity. Furthermore, reactive metabolites resulted in high oxidative stress producing liver cells abrasion. Animals treated with diclofenac at dosage of 150 mg/kg, once daily for 28 days will increase the hepatic enzymes like AST, ALT, ALP and whole bilirubin as to positive control. Diclofenac also causes variations in antioxidant and lipid peroxidation levels.30 The increase in liver serum marker may be due to the accumulation of reactive metabolites produced during the diclofenac metabolism in the liver that leads to a greater level of lipid peroxidation that affects the bio membranes and liver serum markers. Histopathological assessment direct towards the severe peri-acinar necrosis, hydropic degeneration, fatty changes, and degenerating hepatic cells.29-30
Mefenamic acid-induced liver abrasion
A single dose of intraperitoneal (IP) injection of mefenamic acid at 100 mg/kg or 200 mg/kg (in 10% DMSO / Vegetable oil), or treated every day with IP mefenamic acid (at 50 mg/kg or 100 mg/kg in 10% dimethyl sulfoxide/palm oil) for 14 days in male Balb/C mice causes liver dysfunction. Control animals dosed with equal amount of vehicle (10% DMSO/vegetable oil). Blood samples had been collected from the tail vein of mice for subchronic study (50 µL) and placed in 0.3 ml heparinized vials. Blood samples subjected to centrifugation at 4000 rpm for 15 minutes and the plasma used to be transferred to eppendorf tubes where they have been stored at (-20 ºC) till analysis. Hepatic serum markers level measured. Six hours later, after the final dose (single and sub-chronic doses), mice had been sacrificed via cervical dislocation. The liver sample of mice dealt with an excessive dose of mefenamic acid (100 mg/kg for 14 days) confirmed huge degeneration involving the periportal, mid-zonal and centrilobular region. Scattered areas of necrosis were mentioned with some focal inflammatory reactions, many hepatocytes with pyknotic nuclei had been seen in liver sample. Hepatocyte degeneration was detected in the periportal and midzonal regions of the liver in mice treated with mefenamic acid 50 mg/kg. An Abundance of pyknotic nuclei had been located (not shown). The liver of mice dealt with a single dose of 100 mg/kg mefenamic acid confirmed moderate focal degenerative modifications at the periportal region. Midzonal degeneration with hepatocytes pyknosis was found in the liver as an end result of the high dose (200 mg/kg) mefenamic acid treatment. Liver sections of the control mice confirmed normal histology at the periportal, centrilobular and mid-zonal regions.31-32
Antibacterial agents triggered liver toxic animal mode
Tetracycline prompted hepatic abrasion
Tetracycline is related with drug-triggered hepatitis.32 It is recognized to induce fatty liver and has a high risk to liver cirrhosis.33,34 This model was hooked up with a single tetracycline intra peritoneal injection at 50 mg/kg, causes hepatic dysfunction in rats.35 Six hours later, histopathological analysis confirmed apparent abnormal fat accumulation within hepatocytes and elevation in hepatic, serum triglyceride levels. Tetracycline effects lipid metabolic pathways following the four uppermost route way: (1) extended fatty acid uptake with the aid of upregulation of CD36, (2) retarding fatty acid oxidation process, (3) increasing the cellular response of genes engaged in synthesis of TG and cholesterol, and (4) by lowering the generation of TG-rich VLDL due to inhibition of microsomal triglyceride transfer protein.33,36-37 It has been reported that levels of triacylglycerol, total cholesterol method, serum ALT and AST were elevated in male Sprague-Dawley rats treated with 200 mg/kg, body weight, tetracycline (i.p) in saline.38
Adriamycin (doxorubicin) caused liver abrasion
Doxorubicin (Adriamycin) is among the most fascinating drugs in opposition to interdisciplinary extent of malignancy. However, it is scientific manageable due to extreme leukemic adverse outcomes. It is investigated that doxorubicin at (10 mg/kg, single dose) triggered hepatic noxiousness in rats.39
Isoniazid, rifampicin and pyrazinamide precipitated liver abrasion
Antitubercular therapeutic regimens can potentially leads to serious liver toxicity during the antitubercular therapy. Thus, isoniazid, rifampicin and pyrazinamide are hepatotoxic; nevertheless, on administration in combined dosage forms, their harmful impact is increased. Monoacetyl hydrazine is the primary metabolite of Isoniazid (INH) that causes hepatosteatosis. The person accompanying rifampicin treatment have fast tracked instances of liver inflammation due to toxic metabolites produced during rifampicin-induced CYP450 enzyme-induction. In an investigation in rodents, pyrazinamide inhibited CYP450 isoenzymes (2B, 2C, 2E1, 3A), however an examination of individual person liver microsomes confirmed that pyrazinamide has no inhibitory impact on CYP450 isoenzymes.40 Hepatotoxicity was once induced by the combination of three antitubercular tablets namely rifampicin, isoniazid, and pyrazinamide (10, 7.5, and 35 mg/kg, body weight) p.o. daily once for a period of 35 days or administration of isoniazid at 200 or 400 mg/kg/day weekly produced liver toxicity.41 Anomalous expansion of hepatic markers in the systemic circulation is a sign of hepatocellular harm and a marker of necrosis. Rifampicin at dose of 177 and 442.5 mg/kg, for 2 weeks used to estimate LD10 and LD25. Uprising grades of hepatic serum AST, ALT, ALP, TBL and LDH denote the presence of hepatocellular harm and necrosis.42
Anti-Rheumatic Medications
Anti-rheumatic therapeutics are resulted into troublesome liver dysfunctioning. Hepatotoxicity have been observed in the patients treated with sulfasalazine and azathioprine.43
Azathioprine (AZA) prompted hepatic abrasion
AZA is practiced in autoimmune disease and in discontinuing graft rejection. AZA leads to GSH depletion. Prior GSH depletion enhanced toxicity while supplemental GSH used to be protective. GSH in hepatocytes is eaten up throughout uptake of Azathioprine to 6-mercaptopurine. The lipid peroxidation mechanism transformed in-vivo a proportion of endogenous scavengers that are indices of oxidative stress. It has been investigated that oral intake of AZA at dose of 15 mg/kg for 28 days triggered liver abrasion in rodents.43,44
Sulfasalazine outcomed hepatic abrasion
Sulfasalazine is used to treat arthritis and psoriatic arthritis. It is reported to cause liver toxicity in arthritic patients. Most case began in the month of beginning of sulfasalazine therapy, around 25% of sufferers are jaundiced followed by rapidly developing liver failure.45 Sulfasalazine therapy also affects renal function. Both hepatic and renal dysfunctioning analyzed by estimating serum extent of creatinine, ALT, AST, LDH, and ALP. Sulfasalazine-dosed animals were found to have elevated magnitude oxidative stress and lipid peroxidation profile. Furthermore, the intake of sulfasalazine resulted in the depletion of the glutathione level. The histopathology of kidney and liver tissues additionally authenticated the lesions. Sulfasalazine at 600 mg/kg/day, p/o. for 2 consecutive weeks caused kidney and liver damage in rodents.46
Anti-ulcer drug tempted hepatopathy
Ranitidine induced liver abrasion
The metabolic side product of ranitidine is responsible for liver abrasion and oxidative damage. However, one of its metabolites caused an allergic immune allergic response by inducing infiltration of hepatocytes. Histopathological observations confirmed the hepatic inflammation with centrilobular and bridging necrosis. Histopathological analysis also answered focal necrosis of the liver parenchyma with a few accumulations of histiocytic elements and mild steatosis and cholestasis. The study acknowledged fibrosis, bile duct escalation, and hepatocyte infiltration. Hepatic damage demonstrated the upraised proportions of serum AST, plasma bilirubin, and ALP. The intake of ranitidine by intravenous injection for twenty four hours at dosage of 30 mg/kg induce hepatopathy in rodents.47,48
Statin induced liver abrasion
Simvastatin induced liver abrasion
Liver toxicity of simvastatin occur due to drug-drug interactions. There were several cases that were reviews that describe the toxicity of simvastatin with other medications such as flutamide, and diltiazem.49 Liver toxicity was prompted by the ingestion of simvastatin (20 mg/kg, p.o.) for 1 month. On the 31th day, blood samples have been collected, and all the animals were sacrificed by using cervical disconnection and liver sample have been harvested, rinsed in saline for in addition biochemical analysis. The liver harm caused by simvastatin represents changes in liver cell metabolism that result in exclusive changes in liver serum markers. The increased levels of liver serum markers such as SGOT, SGPT, ALP, bilirubin, and decreased inside albumin were found in simvastatin-dosed animals. Simvastatin treated animals also change the cell membrane permeability that represents the severity of hepatocellular damage.50
Dietary models for hepatic abrasion
A diet deficient in methionine and choline-induced liver abrasion
Methionine is an obligatory amino acid required in DNA methylation and glutathione biosynthesis. Methionine Choline deficient diet (MCD) is the most common nutritional model for studying nonalcoholic fatty liver. In this approach, the animals were classified into three classes, each class with eight animals. Class (I) rats serves as normal control and were provided with pellet diet for 60 days, however Class (II, III) were provided with MCD diet for 60 days. Class II served as a positive control and Class III was provided with MLN (melatonin, 10 mg/ kg p.o.,) for the last two consecutive weeks. Concomitantly animals in both group-II and I were provided with water (5 mL/kg p.o).51 Class-II and III animals were provided with MCD diet throughout the whole 14 days. MCD diet outcome in proliferation of essential liver enzymes, total and direct bilirubin in respect to the normal control class. In addition to that, decreased level of albumin was observed in animals fed MCD diet. The MCD diet fed rats with MLN (10 mg/kg/day, orally) for two successive weeks showed reconstruction of serum levels of liver enzymes, total and direct bilirubin. The process resulting in fatty liver due to MCD diet is because methionine and choline deficiency interfere with phosphatidylcholine synthesis that causes oxidative stress, fibroblast growth and increase in the interleukin 6 (IL-6) levels. Furthermore, the MCD diet also triggers nuclear factor-kβ (NF-kβ) resulting in oxidative stress, cell death and liver abrasion.52,53
High-Fat diet induced liver abrasion
Rats dosed with excessive fats (20 mg/rat/day for 13 week) significantly gain liver and body weight.54 Excess fat fed to rats extensively increased serum levels such as GOT, GPT, ALP, and bilirubin with reduced total protein levels. However, the levels of all parameters were considerably restored closer to normalization by the sesame meal treatment. Highly rich fat diet is extensively resulted in liver cells deaths, infiltration of fats in cells, and inflammation. The high fat diet model of hepatic harm promotes oxidative disproportion, heart associated illness that ultimately could provoke hepatic illness.55
Fructose induced hepatic abrasion
Fructose metabolism in the liver instigates lipogenesis and consequently ensuing in lipid accumulation.56 Increased degrees of fructose utilization are related to nonalcoholic fatty liver disease (NAFLD); however, rodents provided with an excessive fructose food plan have been reported to not strengthen fibrosis. Therefore, an accelerated model was developed through the combination of a high-fructose diet with a high-fat diet that could result in fat accumulation in hepatocytes, critical liver inflammation, and fibrosis.57 HFD had been prepared by making an emulsion of 50 ml of solution A prepared by dissolving 6 g of fructose in 125 ml of tween 80 in water with solution B prepared by dissolving 0.4 g of cholesterol in 50 ml of oily solution, and this emulsion is administered at a dose of 10 ml/kg. After intoxication with HFD, to the animals orally for 6 weeks serum levels of a number of enzymes have been recorded. Serum levels of GOT, GPT, ALT, ALP, TB, complete protein and cholesterol level have been assessed.58
Anesthetics models for liver abrasion
These agents are responsible for an adaptable loss of pain and sensitivity. The anesthetic agents are classified as, local and general anesthetics and are responsible for hepatocellular harm, intervene with bilirubin metabolism, and trigger cholestasis.59
Halothane prompted liver abrasion
Halothane is considered a general inhalational anesthetic. The intake of halothane at (30 mmol/kg, intra peritoneal injection form dissolved in 2 ml of olive oil to female and male rodents resulted in liver injury at 12 hours after drug intake. Liver sample of halothane-dosed rat indicates massive hepatocellular and centrilobular necrosis with denaturation. In human beings, it also altered the cerebral glucose-6-phosphate dehydrogenase activities.59
Chloroform prompted liver abrasion
Chloroform was first used by Simpson in 1847. Chloroform causes the hepatic, renal and nasal toxicity by oxidative metabolized with microsomal cytochrome P450. Through the oxidative metabolism of chloroform form inorganic chloride, CO2, phosgene, and some hepatic covalently bound carbon. These carbon atoms bind extensively to liver and kidney tissues and trigger hepatic centrilobular and renal proximal tubular necrosis.60 Rats were dosed with single dose of CHCl3 i.p., (99% dissolved in corn oil) at dosage of 150, 300 or 450 mg/kg, daily. Control animals were provided with the vehicle for 2 days (48 hour group) or 10 consecutive days (10 days group). Animals have been sacrificed 24 hours after the last CHCl3 dosing. Dosing solutions were prepared immediately before administration and had been administered in the amount of 1 ml/kg, body weight. Variations in antioxidant and biochemical markers reflect liver injury. However, the dose-monitored and time-framed consequences of chloroform had been tested on most of the reactive oxygen species producing indices, including GSH depletion. In mild subjection, chloroform accelerated the activities of aminotransferase enzyme and additionally declined the level of mitochondrial proteins.61
Hepatotoxic model of anticancer drug
Methotrexate temped liver abrasion
The mechanisms underlying methotrexate hepatotoxicity are still not clear; however, the cellular pathway of this drug could be the leading cause of liver toxicity.62 Methotrexate take up the folate transporter 1 and is eliminated through the ATP-binding cassette (ABC) family of transporters. Methotrexate is reserved in the cell as a polyglutamate that inhibits dihydrofolate reductase, thymidylate synthase, and 5-aminoimidazole-4-carboxamide-ribonucleotide transformylase, causing a decreased pathway for the RNA and DNA synthesis.63 The remedy of methotrexate in arthritis sufferers has been proven to increase plasma homocysteine levels, however, it is based on simultaneous intake of folate. Animals were injected with a single dose of MTX (20 mg/kg, intra peritoneal) at the 4th of the procedure. Methotrexate increased the level of GOT, GPT, ALP, and LDH while reducing the total protein and albumin level.64
Cisplatin temped hepatic abrasion
Cisplatin is anti-malignant agent used globally, but its overdose could result into severe adverse outcomes including liver toxicities. It has been reported that, intake of cisplatin at 7.5 mg/ kg single i.p., causes hepatic abrasion. Liver toxicity was verified by the estimating elevated levels of essential liver enzymes, along with nitric oxide, albumin, calcium and reduced antioxidant activities of SOD, GSHPx, and GSH.65
Heavy metal precipitated liver abrasion model
Cadmium triggered liver abrasion
Cadmium metals and metalloids influence various human body organs, including the liver. Long-term disclosure to cadmium outcome into hepatic abrasions.66 Cadmium induces oxidative damage in distinct tissues. Cadmium toxicity resulted in the production of reactive oxygen species and later leads to lipid peroxidation, congestive liver, which could result in significant hepatocellular abrasion. Cadmium intensified the serum level of urea, creatinine, glucose, AST, acid phosphatase, ALP, AST, ALT, and serum bilirubin while lowering the serum protein and tissue protein concentration. It has been investigated that intake of cadmium orally at dose of 1 mg/kg, for 15 days in rodents confirmed elevation in hepatic serum markers, acid phosphatase, that outcomes to hepatic tissue abrasion.68
Mercury induced hepatic abrasion
Mercury belongs to the class of heavy metals; it accelerates the production of reactive oxygen species that elevates lipid peroxides and hydroxyl radicals causing the biomembrane injury followed by cell destruction. Mercury also inhibits the enzymes such as CAT, SOD, and GSH peroxidase. The excess production of ROS by mercury can block the permeability of the transition pore in mitochondria. It is cited that post intake of mercuric chloride at dosage of (5 mg/kg, intra peritoneal injection) for 20 days and oral dose of (2 mg/kg) for 30 days triggered hepatopathy in rodents.69
Hormones precipitated liver abrasion
Tamoxifen prompted liver abrasion
However, the novel androgens are used in the hormonal manipulation of breast carcinoma and increase the chance of intrahepatic cholestasis followed by hepatic malfunction. The persistent use of any 17-alkyl androgen has outcome into hepatic adenocarcinomas. Cholestatic hepatitis, probably idiosyncratic, has been pronounced the use of the anti-androgen like flutamide for prostate neoplasm, megestrol acetate and tamoxifen remedy for breast cell carcinoma.70-72 Rats dosed with tamoxifen at the dose level of 45 mg/kg/day, i.p. in 0.1 mL of dimethyl sulfoxide and isotonic saline solution for 6 days triggered hepatotoxicity.73
Toxins precipitated hepatopathy model
Phalloidin precipitated liver abrasion
The green death cap of the mushroom (Amanita phalloides) produced phalloidin toxins, which are cyclopeptide. The intravenous administration of phalloidin in rat at the dose of 50 µg/100g, body weight, induces a cytolytic lesion in liver. It causes severe hepatic damage characterized by cholestasis, which is due in section to irreversible polymerization of actin filaments.74
Aflatoxin B1 (AFB1) caused liver abrasion
Naturally occurring fungal toxin like Aflatoxin B1 (AFB1) that motives both acute hepatic dysfunction as well as hepatic carcinoma in humans and animals. It produces the hepatopathy by forming adducts with DNA, in rat liver.75 The animal treated with single dose (1 mg/kg, orally) of aflatoxin will increase hepatic serum markers like GOT, GPT, ALP and bilirubin, while reduce the serum cholesterol level. Hemorrhage, necrosis, and huge accumulation of lipid were seen in liver sample that confirmed the hepatotoxicity.76
Miscellaneous Drugs
Thioacetamide prompted hepatic abrasion
The metabolic product of thioacetamide is accountable for hepatic abrasion by interfering with the movement of RNA from the nucleus to the cytoplasm. Thioacetamide decreases the number of viable hepatocytes by reducing the rate of oxygen consumption. In addition, it decreases the volume of bile and its content, such as bile salts, cholic, and deoxycholic acid. It also oxidized to ROS like S-oxide that is answerable for the modification in cell permeability, increases the intracellular Ca2+ level, and obstructs mitochondrial endeavor that clues to cell death.77 Rat dosed with thioacetamide at 200 mg/kg, body weight, i.p thrice weekly for eight weeks to prompted hepatopathy.78
D-Galactosamine caused liver abrasion
D-Galactosamine is a well-known model of hepatopathy that strictly resembles acute liver failure. D-Galactosamine activates macrophages and Kupffer cells to produce TNF-α, TNF-α triggers caspases and transcription factors such as NF-κB that leading to cell demise. On the other hand, it selectively depletes liver uridine nucleotides and inhibits RNA synthesis in liver cells.79 A single dose of D-Galactosamine can precipitate hepatocellular necrosis followed by fatty liver. Its toxic mechanism motives to loss of the activity of various ion by enhancing the cellular membrane permeability that lead to the liberation of enzymes and extend the intracellular Ca2+ level, which is accountable for hepatic cell death.80,81 Intraperitoneal single dose injection of D-galactosamine at 200 mg/kg, body weight, prompted the hepatotoxicity in rat.82
Carbon tetrachloride prompted hepatic abrasion
CCl4 is not a drug, but its excess dose (≥1 mL/kg) motive reproducible acute liver damage. CCl4 is tempted hepatopathy model is the most frequent model of acute liver injury.83 CCl4 is tempted toxicity is depends on the metabolism of CCl4 by Cyp-P450 enzymes to trichloromethyl radical (CCl3·) and peroxy-trichloromethyl radicals (·OOCCl3) which is a reactive metabolite. Both free radicals covalently bind to macromolecules structure of hepatic cells such as proteins, lipids and nucleic acids and induce the necrosis in centrilobular region. Administration of CCl4 at 1 ml/kg, body weight, of saline (0.85%) intra-gastrically and olive oil (3 ml/kg, body weight) intraperitoneally twice a week for four weeks causes the alteration in hepatic serum markers (GOT, GPT, ALT and ALP), antioxidant enzymes (like GSH and MDA) and inflammatory mediator like TNF-α. Alteration of these parameters indicates liver damage. The biochemical observations were supported by histological answers in rat liver in CCl4 dosed animals.84
Bromobenzene prompted hepatic abrasion
Bromobenzene is an industrial solvent that causes necrosis in the liver cells. It hydrolyzed by monooxygenases CYPs. CYPs mediated epoxidation yields the enormously electrophilic BB 3,4-epoxide that produce liver as well as renal toxicity. Administration of bromobenzene at 460 mg/kg, p.o., in mice for 7 days causes hepatopathy. Mice were sacrificed, 24 hours after the last administration of the test drug. Blood samples were collected for the determination of liver serum markers like AST, ALT, and ALP. Hepatotoxicity in mice was confirmed due to an increase in the level of liver serum marker. In histological study, bromobenzene treated group shows severe centrilobular necrosis, massive fatty changes, ballooning degeneration, and lymphocytes infiltration. In another model the rat dosed with Bromobenzene at 0.5, 2.0 and 5.0 mmole/kg, body weight, dissolved in corn oil, 40% v/v) administered orally for 10-12 weeks is accountable for hepatotoxicity in rats.85
Acrylamide (AA) triggered liver abrasion
Acrylamide is a vinyl monomer employed in the manufacturing of polyacrylamides. It has been reported to induce various noxious outcomes in rodents. In the human body, it is metabolized to epoxide glycidamide (2, 3-epoxypro-pionamide) by oxidation through CYP4502E1. Acryl amide undergoes biotransformation in conjugation with GSH. Rats treated every day at dose of 6 mg/kg of acrylamide, intra peritoneal injection for 15 days were investigated to have liver abrasions.86
Microcystin precipitated hepatic abrasion
Microcystin is a potent hepatotoxin produced by the blue-green algae Microcystis aeruginosa. Pathological examination of livers of mice and rats showed the severe, centrilobular hepatocellular apoptosis, and hemorrhage. Mice that received sublethal doses of microcystin at 20 g/kg for 28 weeks developed liver cirrohosis.87
Lithocholic acid induced liver abrasion
Lithocholic acid continuation in the dietary regimen develop hepatic cholestasis and bile canalicular membrane infarction. It is a water repelling bile acid produced by the reduction of chenodeoxycholic acid in the gastrointestinal tract. The assembling of lithocholic acid caused its precipitation and obstruction of bile network resulting into hepatocellular necrosis and neutrophils aggregation. Therefore, these alterations revealed liver toxicity. Lithocholic acid intake as intravenous dosage of 4 μmol/kg developed hepatocellular necrosis in animals.88
TNF inhibitors induced liver abrasion
Increase transaminases levels had been reported after treatment with broadly studied TNF inhibitors, namely adalimumab, etanercept, and infliximab. In an investigation involving 6,861 arthritis patients over 14 thousand patients, it was concluded that liver enzyme indices increased to more than double in 0.6% of patients on the anti-TNF regimen compared to normal healthy individuals89. The etiology of liver injury with anti-TNF agents may be correlated to the promising fact that monoclonal antibodies form immune complexes promptly to greater extent than etanercept.90
Conclusion
The catalogue of medications that cause liver abrasion is enormous and total inclusion is troublesome. Additionally, a numerous drugs are the utilized for various restorative signs that are harmful to the liver after continuous administration with high dose for long term. Overall, significant progress is being made in our understanding of experimental animal models, but considerable work in future, remains to be done.
Acknowledgement
Hygia Institute of Pharmaceutical Education and Research, Lucknow, Uttar Pradesh, India supported this work.
Conflict of Interest
No conflict of interest is associated with this review work.
Funding Sources
There is no Funding sources
References
- Ichai P, Samuel D. Epidemiology of liver failure. Clin. Res. Hepatol. Gastroenterol., 2011; 35(10): 610-617.
CrossRef - Lee WM. Drug-induced hepatotoxicity. N. Eng. J. Med., 2003; 349(5): 474-485.
CrossRef - Zhao P, Wang C, Liu W, Chen G, Liu X, Wang Xi, Wang B, Yu L, Sun Y, Liand X, Yang H, Zhang F. Causes and outcomes of acute liver failure in China. Plos One, 2013; 8(11): 1-6.
CrossRef - Suk KT, Kim DJ. Drug-induced liver injury: present and future. Clin. Mol. Hepatol., 2012; 18(3): 249-257.
CrossRef - Chen M, Vijay V, Shi Q, Liu Z, Fang H, Tong W. FDA-approved drug labeling for the study of drug-induced liver injury. Drug Discov. Today., 2011; 16(15-16): 697-703.
CrossRef - Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS, Reisch SJ, Sciodt FV, Ostapowicz G, Shakil AO, Lee WM. Acetaminophen induced acute liver failure: results of a United States multicenter, prospective study. Hepatol., 2005; 42(6): 1364-1372.
CrossRef - Kaplowitz, N. Drug-induced liver disorders: implications for drug development and regulation. Drug Saf., 2001; 24(7): 483-490.
CrossRef - Senior JR. Drug hepatotoxicity from a regulatory perspective. Clin Liver Dis., 2007; 11(3): 507-524.
CrossRef - Chaudhary S, Semwal A, Kumar H, Verma HC, Kumar A. In-vivo study for anti-hyperglycemic potential of aqueous extract of basil seeds (Ocimum basilicum linn) and its influence on biochemical parameters, serum electrolytes and haematological indices. Biomed. Pharmacother., 2016; 84: 2008-2013.
CrossRef - Chaudhary S, Kumar H, Verma H, Rajpoot A. Synthesis and biological screening of proline rich cyclic heptapeptide. Int. J. Pharmtech Res., 2012; 4(1): 194-200.
- Gupta RK, Chaudhary S, Vaishali, Singh RK. Antihepatotoxic influence of aqueous extract of Ipomoea carnea against carbon tetrachloride induced acute liver toxicity in experimental rodents. Asian J. Pharm. Clin. Res., 2012; 5(Suppl 4): 262-265.
- El-Shorbagi AN, El-Naggar M, Tarazi H, Chaudhary S, Abdu-Allah H, Hersi F, Omar H. Bis-(5-substituted-2-thiono-1,3,5-thiadiazinan-3-yl) butane as a scaffold of anti-proliferative activity, blended by a multicomponent process. Med. Chem. Res., 2018; 27(4): 1103-1110.
CrossRef - Chaudhary S, Negi A, Dahiya V. The study of in vitro antimicrobial activity and phytochemical analysis of some medicinal plants in Chamoli Garhwal Region. Pharmacogn. J., 2010; 2(12): 481-485.
CrossRef - Chaudhary S, Gupta RK, Kumar A, Tarazi H. Hepatoprotective and antioxidant potential of Nyctanthes arbortristis leaves against antitubercular drugs induced hepatotoxicity. J. Phar. Pharmacogn. Res., 2018; 6(3): 205-215.
- Chaudhary S, Verma HC, Gupta MK, Kumar HK, Swain SR, Gupta RK, El-Shorbagi AN. Antidiabetic aptitude of Cordia sebestena and its outcome on biological parameters, serum electrolytes, and hematological markers. Pharmacogn. J., 2019; 11(2): 418-423.
CrossRef - El-Shorbagi AN, Chaudhary S. Monobactams: A unique natural scaffold of four-membered ring skeleton, recent development to clinically overcome infections by multidrug-resistant microbes. Lett. Drug. Des. Discov., 2019; 16(12): 1305-1320.
CrossRef - Chaudhary S, Singh RK, Gupta RK. Synthesis and biological activity of peptide derivatives of 2-hydroxy-5-(6-iodo-2-methyl-4-oxoquinazolin-3(4H)-yl) benzoic acid. Asian J. Pharm. Clin. Res., 2012; 5(4): 196-200.
- Chaudhary S, Gupta RK, Gupta MK, Verma HC, Kumar HK, Kumar A, Swain SR, El-Shorbagi AN. Hepatoprotective response of Cordia sebestena fruits against simvastatin induced hepatotoxicity. J. Phar. Pharmacogn. Res., 2020; 8(4): 327-335.
- Chaudhary S, Hisham H, Mohamed D. A review on phytochemical and pharmacological potential of watercress plant. Asian J. Pharm. Clin. Res., 2018; 11(12): 102-107.
CrossRef - Gupta RK, Swain SR, Sahoo J, Chaudhary S, Gupta A. Isolation, characterization and hepatoprotective activity of naturally occurring protopine against simvastatin induced liver toxicity in experimental rodents. Curr. Bioact. Compd., 2020, 16(5): 568-575.
CrossRef - Chaudhary S, Kumar S, Tarazi H. Peptide derivatives of 1,2-dihydro-3-methyl-2-oxoquinoxaline-6-carboxylic acid: synthesis and evaluation of antimicrobial, antifungal and antiviral potential. Pharm. Chem. J., 2016; 50(5): 331-338.
CrossRef - Gupta MK, Kumar S, Chaudhary S. Synthesis and Investigation of antidiabetic response of new coumarin derivatives against streptozotocin induced diabetes in experimental rats. Pharm. Chem. J., 2020; 53(12): 1122-1127.
CrossRef - El-Shorbagi AN, Chaudhary S, Alshemali KA, Alabdulrazzaq RF, Alqahtani FY. A comprehensive review on management of Parkinson’s disease, inclusive of drug discovery and pharmacological approaches. J. Appl. Pharm. Sci., 2020; 10(10): 130-150.
- Chaudhary S, Kumar S. Synthesis and biological activity of peptide derivatives of 1,2-dihydro-3-methyl-2-oxoquinoxaline-6-carboxylic acid. Der Pharma Chem., 2015; 7(9): 210-220.
- Chaudhary S, Pal A. Indian Medicinal Plants used in liver disease: A short review. Pharmacogn. J., 2011; 3(19): 91-94.
CrossRef - Gupta RK, Singh RK, Kr N. Screening of anti-hepatotoxic potential of Solanum xanthocarpum leaf against CCl4 induced acute hepatopathy in experimental rodents. Asian J. Pharm. Clin. Res., 2012; 5(4): 211-214.
- McGill MR, Jaeschke, H. Mechanistic biomarkers in acetaminophen-induced hepatotoxicity and acute liver failure: from preclinical models to patients. Expert Opin.Drug Metabol. Toxicol., 2014; 10(7): 1005-1017.
CrossRef - Eliwa HA, El-Denshary ES, Nada SA, Elyamany MF, Omara EA, Asaaf N. Evaluation of the therapeutic effect of whey proteins on the hepatotoxicity induced by paracetamol and alcohol co-administration in rats. J.Pharma. Res. Biosci., 2014; 3(2): 295-314.
- Aithal GP. Hepatotoxicity related to antirheumatic drugs. Rev. Rheumatol., 2011; 7(3): 139-150.
CrossRef - Maity T, Ahmad A, Pahari N, Ganguli S.. Hepatoprotective activity of Mikania scandens (L.) willd. against diclofenac sodium induced liver toxicity in rats. Asian J. Pharm. Clin. Res., 2012; 5(2): 185-189.
- Somchit N, Sanat F, Gan EH, Shahrin AW, Zuraini A. Liver injury induced by the non-steroidal anti-inflammatory drug mefenamic acid. Singapore Med. J., 2004; 45(11): 530-532.
- Connor NO, Dargan PI, Jones AL. Hepatocellular damage from non-steroidal anti-inflammatory drugs. J. Med., 2003; 96: 787-791.
CrossRef - Serafini-Cessi, F. Conversion of allyl alcohol into acrolein by rat liver. J., 1972; 128(5): 1103-1107.
CrossRef - Esterbauer H, Zollner H, Scholz N. Reaction of glutathione with conjugated carbonyls. Zeitschrift fur Naturforschung Section C: Biosci., 1975; 30(4): 466-473.
CrossRef - Boyland E, Chasseaud LF. Enzyme-catalysed conjugations of glutathione with unsaturated compounds. J., 1967; 104(1): 95‑102.
CrossRef - Jaeschke H, Kleinwaechter C, Wendel A. The role of acrolein in allyl alcohol-induced lipid peroxidation and liver cell damage in mice. Pharmacol., 1987; 36(1): 51-57.
CrossRef - Starckx S, Batheja A, Verheyen GR, Jonghe SD, Steemans K, Dijck BV, Singer M, Bogdan N, Snoeys J, Vinken P, Sasaki JC, Gompel JV, Guzzie-Peck P, Lampo A, Lammens L. Evaluation of miR-122 and other biomarkers in distinct acute liver injury in rats. Pathol., 2013; 41(5): 795-804.
CrossRef - McLain GE, Sipes IG, Brown BRJ. An animal model of halothane hepatotoxicity: Roles of enzyme induction and hypoxia. Anesthesiol., 1979; 51(4): 321-326.
CrossRef - Sakr SA, Abo-El-Yazid SM. Effect of fenugreek seed extract on Adriamycin-induced hepatotoxicity and oxidative stress in albino rats. T Ind. Health., 2012; 28(10): 876-885.
CrossRef - Nishimura Y, Kurata N, Sakurai E, Yasuhara H. Inhibitory effect of anti-tuberculosis drugs on human cytochrome P450-mediated activities. Pharmacol. Sci., 2004; 96: 293-300.
CrossRef - Hussain T, Gupta RK, Sweety K, Khan MJ, Hussain MS, Arif M, Hussain A, Faiyazuddin M, Rao CV. Evaluation of antihepatotoxic potential of Solanum xanthocarpumfruit extract against antitubercular drugs induced hepatopathy in experimental rodents. Asian Pac. J. Trop. Biomed., 2012; 2(6): 454-460.
CrossRef - Tostmann A, Boeree MJ, Aarnoutse RE, de Lange WCM, Ven AJAM, Dekhuijzen R. Anti-tuberculosis drug-induced hepatotoxicity: Concise up-to-date review. Gastroenterol. Hepatol., 2008; 23: 192-202.
CrossRef - Raza M, Ahmad M, Gado A, Al-Shabanah OA. A comparison of hepatoprotective activities of aminoguanidine and N-acetylcysteine in rat against the toxic damage induced by azathioprine. Comp. Biochem. Physiol C. Toxicol. Pharmacol., 2003; 134(4): 451-456.
CrossRef - Bolkent S, Arda-Pirincci P, Bolkent S, Yanardag R, Tunali S, Yildirim S. Influence of zinc sulfate intake on acute ethanol induced liver injury in rats. World J. Gastrenterol., 2006; 12(27): 4345-4351.
CrossRef - Jobanputra P, Amarasena R, Maggs F, Homer D, Bowman S, Rankin E, Filer A, Raza K, Jubb R. Hepatotoxicity associated with sulfasalazine in inflammatory arthritis: a case series from a local surveillance of serious adverse events. BMC Musculoskelet. Disord., 2008; 9(48): 1-7.
CrossRef - Linares V, Alonso V, Albina ML, Belles M, Sirvent JJ, Domingo JL, Sanchez DJ. Lipid peroxidation and antioxidant status in kidney and liver of rats treated with sulfasalazine. Toxicology, 2009; 256(3): 152-156.
CrossRef - Hemieda FA, Abdel-Hady el-SK EMA. Biochemical and histological studies on H2-receptor antagonist ranitidine-induced hepatotoxicity in rats. J. Exp. Biol., 2005; 43(9): 782-785.
- Maddox J F, Luyendyk JP, Cosma GN, Breau AP, Bible RJ, Harrigan GG, Goodacre R, Ganey PE, Cantor GH, Cockerell GL, Roth RA. Metabonomic evaluation of idiosyncrasy-like liver injury in rats cotreated with ranitidine and lipopolysaccharide. Appl. Pharmacol., 2006; 212(1): 35-44.
CrossRef - Gupta RK, Swain SR, Sahoo J, Gupta A, Chaudhary S. Hepatoprotective Potential of Trichosanthes dioica Roxb in hepatotoxicity induced by simvastatin and its consequences on biochemical and haematological indices. J., 2018; 10(4): 720-724.
CrossRef - Caldwell SH, Hespenheide EE, Borstel RW. Myositis, microvesicular hepatitis, and progression to cirrhosis from troglitazone added to simvastatin. Dis. Sci., 2001; 46(2): 376-378.
CrossRef - Amini R, Yazdanparast R, Aghazadeh S, Ghaffari SH. Teucrium polium reversed the MCD diet-induced liver injury in rats. Human Exp. Toxicol., 2011; 30(9): 1303-1312.
CrossRef - Pan M, Song YL, Xu JM, Gan HZ. Melatonin ameliorates nonalcoholic fatty liver induced by high-fat diet in rats. Pineal Res., 2006; 41(1): 79-84.
CrossRef - Dela PA, Leclercq I, Field J, George J, Jones B, Farrell G. NF-kappa B activation, rather than TNF, mediates hepatic inflammation in a murine dietary model of steatohepatitis. Gastroenterol., 2005; 129: 1663-1674.
CrossRef - Wang N, Li P, Wang Y, Peng W. Hepatoprotective effect of Hypricum japonicum extract and its function. J. Ethanopharmacol., 2008; 116: 1-6.
CrossRef - Kakimoto PA, Kowaltowski AJ. Effects of high fat diets on rodent liver bioenergetics and oxidative imbalance. Redox , 2016; 8: 216-225.
CrossRef - Alisi A, Manco M, Pezzullo M, Nobili V. Fructose at the center of necroinflammation and fibrosis in nonalcoholic steatohepatitis. Hepatology, 2011; 53(1): 372-373.
CrossRef - Ge CX, Yu R, Xu MX, Li PQ, Fan CY, Li JM, Kong LD. Betaine prevented fructose-induced NAFLD by regulating LXRa/ PPARa pathway and alleviating ER stress in rats. J. Pharmacol., 2016; 770: 154-164.
CrossRef - Sharma A, Chakraborty KK, Handa SS. Anti-hepatotoxic activity of some Indian herbal formulations as compared to silymarin. Fitoterapia, 1991; 62: 229-235.
- You Q, Cheng L, Reilly TP, Wegmann D, Ju C. Role of neutrophils in a mouse model of halothane-induced liver injury. Hepatology, 2006; 44(6): 1421-1431.
CrossRef - Njoku D, Laster MJ, Gong DH. Biotransformation of halothane, enflurane, isoflurane and desflurane to trifluoroacetylated liver proteins: association between protein acylation and hepatic injury. Analg., 1997; 84(1): 173-178.
CrossRef - Larson JL, Wolf DC, Mery S, Morgan KT, Butterworth BE. Toxicity and cell proliferation in the liver, kidneys and nasal passages of female F-344 rats, induced by chloroform administered by gavage. Food Chem.Toxicol., 1995; 33(6): 443-456.
CrossRef - Kremer JM. Toward a better understanding of methotrexate. Arthritis Rheum., 2004; 50(5): 1370-1382.
CrossRef - Chandran V, Schentag CT, Gladman DD. Reappraisal of the effectiveness of methotrexate in psoriatic arthritis: results from a longitudinal observational cohort. Rheumatol., 2008; 35(3): 469-471.
- Hemeida RAM, Mohafez OM. Curcumin attenuates methotrexate-induced hepatic oxidative damage in rats. Egypt Natl. Canc. Inst., 2008; 20(2): 141-148.
- Mansour HH, Hafez HF, Fahmy NM. Silymarin Modulates Cisplatin-Induced Oxidative Stress and Hepatotoxicity in Rats. Biochem. Mol. Biol., 2006; 39(6): 656-661.
CrossRef - Järup L, Berglund M, Elinder CG, Nordberg G, Vahter M. Health effects of cadmium exposure- A review of the literature and a risk estimate. Scand J Work Environ Health., 1998; 24(1): 1-51.
- Stohs SJ, Bagchi D, Hassoun E, Bagchi M. Oxidative mechanisms in the toxicity of chromium and cadmium ions. Environ. Pathol., Toxicol. Oncol., 2000; 19(3): 201-213.
- Singh N, Rani P, Gupta M, Goel N, Tandon N. Effects of aqueous extract of Camellia sinensis on liver markers of cadmium treated rats. E3 J. Biotech. Res., 2013; 4(5): 89-93.
- Jagadeesan G, Sankarsami PS. Hepatoprotective effects of taurine against mercury induced toxicity in rats. Environ. Biol, 2007; 28(4): 753‑756.
- Rosman AS, Frissora-Rodeo C, Marshall AT, Reiter BP, Paronetto F. Cholestatic hepatitis following flutamide. Dis. Sci., 1993; 38(9): 1756‑1759.
CrossRef - Foitl DR, Hyman G, Lefkowitch JH. Jaundice and intrahepatic cholestasis following high-dose megestrol acetate for breast cancer. Cancer, 1989; 63(3): 438-439.
CrossRef - Pinto HC, Baptista A, Camilo ME, De Costa EB, Valente A, de Moura MC. Tamoxifen-associated steatohepatitis Report of three cases. Hepatol., 1995; 23(1): 95-97.
CrossRef - Oh JM, Jung YS, Jeon BS, Yoon BI, Lee KS, Kim BH, Oh SJ, Kim SK. Evaluation of hepatotoxicity and oxidative stress in rats treated with tert-butyl hydroperoxide. Food Chem. Toxicol., 2012; 50(5): 1215-1221.
CrossRef - Herraez E, Macias RI, Vazquez-Tato J, Hierro C, Monte MJ, Marin JJG. Protective effect of bile acid derivatives in phalloidin-induced rat liver toxicity. Appl. Pharmacol., 2009; 239(1): 21-28.
CrossRef - Essigmann JM, Croy RG, Nadzan AM, Jr BWF, Reinhold VN, Buchi G, Wogan GN. Structural identification of the major DNA adduct formed by aflatoxin B1 in vitro. Natl. Acad. Sci. USA, 1977; 74(5): 1870-1874.
CrossRef - Sharmila BG, Kumar G, Murugesan AG. Effect of ethanolic leaf extract of Trianthemaportulacastrum on aflatoxin induced hepatic damage in rats. Ind. J. Clin. Biochem., 2009; 24(4): 414-418.
CrossRef - Amin ZA, Bilgen M, Alshawsh MA, Ali HM, Hadi HA, Abdulla MA. Protective role of Phyllanthus niruri extract against thioacetamide-induced liver cirrhosis in rat model. Based Complement. Alternat. Med, 2012; 2012(5): 241583.
CrossRef - Ambrose AM, Deeds F, Rather LJ. Further studies on toxicity of thioacetamide in rats. Pro. Soc. Exp. Biol. Med., 1950; 74(1): 132-134.
CrossRef - Simeonova R, Kondeva-Burdina M, Vitcheva V. Some in vitro/in vivo chemically-induced experimental models of liver oxidative stress in rats. BioMed Res. Int., 2014; 2014; 1-6.
CrossRef - Lim HK, Kim HS, Choi HS, Oh S, Jang CG, Choi J, Kim SH, Chang MJ. Effects of acetyl bergenin against d-galactosamine-induced hepatotoxicity in rats. Res., 2000; 42(5): 471-474.
CrossRef - Raj PV, Nitesh K, Prateek J, Sankhe MN, Rao JV, Rao CM, Udupa N. Effect of lecithin on d-galactosamine induced hepatotoxicity through mitochondrial pathway involving Bcl-2 and Bax. Ind. J. Clin. Biochem., 2011; 26(4): 378-384.
CrossRef - Poli G. Pathogenesis of liver fibrosis: role of oxidative stress. Mol. Aspects Med., 2000; 21(3): 49-98.
CrossRef - Weber LW, Boll M, Stampfl A. Hepatotoxicity and mechanism of action of haloalkanes: carbon tetrachloride as a toxicological model. Crit. Rev. Toxicol., 2003; 33(2): 105-336.
CrossRef - Khan RA, Khan MR, Sahreen CCl4-induced hepatotoxicity: protective effect of rutin on p53, CYP2E1 and the antioxidative status in rat. BMC Complement. Altern. Med., 2012; 12(178): 1-6.
CrossRef - Kalantari H, Rashidi I, Nazari Z, Keliddar A, Foruozandeh H, Kalantar M. Study of the Protective Effect of Livergol against Liver Toxicity Caused by Bromobenzene in Mice. I J. Pharm. Sci., 2014; 10(1): 11-20.
- Khan MR, Afzaal M, Saeed N, Shabbir M. Protective potential of methanol extract of Digera muricataon acrylamide induced hepatotoxicity in rats. J. Biotechnol., 2011; 10(42): 8456-8464.
CrossRef - Clark SP, Davis MA, Ryan TP, Seafoss GH, Hooser SB. Hepatic gene expression changes in mice associated with prolonged sublethal microcystin exposure. Pathol., 2007; 35(4), 594-605.
CrossRef - Bonvicini F, Gautier A, Gardiol D, Borel GA. Cholesterol in acute cholestasis induced by taurolithocholic acid. A cytochemical study in transmission and scanning electron microscopy. Invest., 1978; 38(4): 487-495.
CrossRef - Sokolove J, Strand V, Greenberg JD, Curtis JR, Kavanaugh A, Kremer JM, Anofrei A, Reed G, Leonard C, Hooper M, Baumgartner S, Furst DE. Risk of elevated liver enzymes associated with TNF inhibitor utilization in patients with rheumatoid arthritis. Rheum. Dis., 2010; 69(9): 1612-1617.
CrossRef - Strand V, Kimberly R, Isaacs JD. Biologic therapies in rheumatology: lessons learned future directions. Rev. Drug Discov., 2007; 6(1): 75-92.
CrossRef




