
Manuscript accepted on :20-01-2022
Published online on: 03-02-2022
Plagiarism Check: Yes
Reviewed by: Dr. Abdelmonem Hegazy
Second Review by: Dr. Vasanth Kumar
Final Approval by: Dr. Fai poon
Esakkiammal. N1* , Archana. R2 and WMS Johnson 3
, Archana. R2 and WMS Johnson 3
1Department of Anatomy, Bharath Institute of Higher Education and Research, Chennai, India, 600126.
2Department of Anatomy, Sree Balaji Medical College and Hospital, BIHER, Chennai, India,600044.
Corresponding Author E-mail: esakki510@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2338
Abstract
The posterior intercostal veins drain the thoracic wall and lie in the costal grooves along with the intercostal arteries and nerves posterior to the thoracic sympathetic chain. During routine dissection of the posterior mediastinum of a formalin-fixed male cadaver in the Anatomy department of an undergraduate and postgraduate teaching medical college in India, a large-sized posterior intercostal vein was identified crossing anterior to the thoracic sympathetic chain at the level of the 3rd intercostal space on the right side. The presence of such variation may hinder the surgical procedure of the posterior mediastinum and will pose an increased risk of intraoperative or postoperative bleeding. Knowledge of such variation is necessary to avoid laceration of the posterior intercostal vein, which is the potential cause of bleeding in the region of the thorax.
Keywords
Posterior Intercostal Vein; Posterior Mediastinum; Thoracic Surgery
Download this article as:| Copy the following to cite this article: Esakkiammal N, Archana R, Johnson W. M. S. Unusual Course of Posterior Intercostal Vein at the 3rd Intercostal Space – A Case Report. Biomed Pharmacol J 2022;15(1). |
| Copy the following to cite this URL: Esakkiammal N, Archana R, Johnson W. M. S. Unusual Course of Posterior Intercostal Vein at the 3rd Intercostal Space – A Case Report. Biomed Pharmacol J 2022;15(1). Available from: https://bit.ly/3sflvAb |
Introduction
There are 11 posterior intercostal veins and one subcostal vein on each side of the thoracic wall. The first posterior intercostal vein directly drains into the brachiocephalic vein on both sides. The second and third and occasionally fourth intercostal veins unite to form a trunk, the superior intercostal vein, which drains into the brachiocephalic vein on the left side and the azygos vein on the right side1 (Fig.1)2.
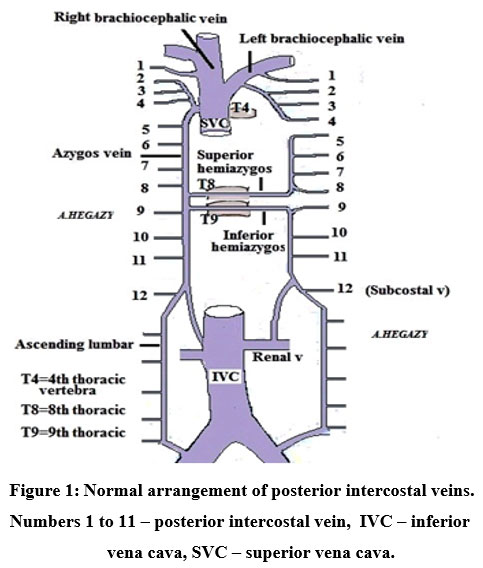 |
Figure 1: Normal arrangement of posterior intercostal veins. Numbers 1 to 11 – posterior intercostal vein, IVC – inferior vena cava, SVC – superior vena cava. |
Endoscopic thoracic sympathectomy is regarded as a safe efficient technique usually performed at the level of T2 sympathetic ganglion to block postganglionic sympathetic stimulus for the treatment of a variety of autonomic disorders such as primary palmar hyperhidrosis, facial blushing, and certain vascular disorders 3. However, there are some instances of failure of the treatment due to additional nerve fibres (Nerve of Kuntz) directly connecting the sympathetic fibres from the 2nd thoracic ganglion to the brachial plexus. Surgeons to avoid this prefer the third or fourth thoracic ganglia for sympathectomy to reduce the recurrence of the postoperative symptoms 4. Anatomical variations of the posterior intercostal veins at the level of 3rd and 4th intercostal space may disrupt while sympathectomy leads to complications such as bleeding. Therefore, in the present case report, we explain an anatomical variation of the anterior crossing of the posterior intercostals vein in the 3rd intercostal space and its surgical significance.
Case description
During routine dissection of the posterior mediastinum of the formalin-fixed male cadaver, the posterior intercostals vein crossed anteriorly to the thoracic sympathetic chain at the level of the 3rd intercostals space on the right side and drains into the superior intercostal vein in the Anatomy department of an undergraduate and postgraduate teaching medical college in India. The external diameter of the vein was measured (24.4mm) and photographed (Fig.2).
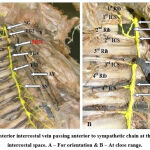 |
Figure 2: Posterior intercostal vein passing anterior to sympathetic chain at the level of 3rd intercostal space. A – For orientation & B – At close range. |
SG – stellate ganglion, INK – intrathoracic nerve of Kuntz TG2, TG4 – thoracic ganglion, 1st ICS, 2nd ICS, 3rd ICS – intercostal space, TST – thoracic sympathetic trunk, AV – azygos vein, SN – splanchnic nerve, PICV – posterior intercostal vein.
Discussion
Haam et al found a large posterior intercostal vein crossing anteriorly to the sympathetic trunk in 27.3% of cases on the 3rd and 15.9% of cases on the 4th intercostal spaces on the right side 5. In 12% of cases, the 2nd posterior intercostals vein crossed anteriorly on the right side observed by Ramsaroop et al study 6. In the present case report is also in agreement to the previous literatures (Haam et al & Ramsaroop et al) reports of a large posterior intercostal vein crossed the sympathetic trunk anteriorly at the level of the 3rd intercostal space on the right side. During surgical procedures posterior intercostal veins passing anteriorly to the sympathetic trunk are not commonly noticed but if it is present the prevalence of bleeding is more. Gossot et al studied and reported that 5.3% of cases during sympathectomy injury to the posterior intercostal vein lead to hemothorax 7. The incidence percentage of hemothorax is 5.6% while endoscopic thoracic sympathectomy was reported by Reisfeld et al and Rodriguez et al and 0.3 % of cases are documented by Ueyama et al 8-10. The iatrogenic injury of the posterior intercostals vein is the potential cause of bleeding in the region of the thorax while surgeons operating in the 3rd and 4th intercostal spaces on the right side.
Kim et al. revealed that the posterior intercostal vein runs over the rib head in the right-side 3rd, 4th, and 5th rib levels, in 13.6%, 31.8%, 56.8%, and 4.5%, 4.5%, and 18.2% on the left sides respectively. Since the right sympathetic trunk has a greater affinity for medial move compared to the left cause due to the large posterior intercostal veins, runs over or under to the sympathetic trunk at these levels 11. Haam et al stated that the crossing veins anteriorly are not as significant; the kind of crossing vein is important 5.
Conclusion
Surgical procedures of the posterior mediastinum structure may have increased risks due to this large anterior crossing of posterior intercostal veins specifically at the level of 3rd and 4th intercostal space. Surgeons’ operating in the region of the thorax is should be aware of anatomical variations in the size and course of the posterior intercostal vein to avoid complications of intraoperative or postoperative bleeding successfully.
Acknowledgment
None
Conflicts of interest
There is no conflict of interest
Funding source
There is no funding source.
References
- Standring S. Gray’s Anatomy The Anatomical Basis Of Clinical Practice 40th edition, Elsevier Health Sciences UK, 2008; p. 1723-6.
- Hegazy A. Clinical Anatomy of Thorax for Medical Students and Doctors. LAP LAMBERT Academic Publishing, 2018; P.16-21.
- Reisfeld R. Endoscopic thoracic sympathectomy for hyperhidrosis: experience with both cauterization and clamping methods. Surg Laparosc Endosc Percutan Tech, 2002;12:255-267.
CrossRef - Zhang B, Li Z, Yang X, Wang Y, Cheng J et al. Anatomical variations of the upper thoracic sympathetic chain. Clin Anat, 2009;22:595-600.
CrossRef - S, kim. D, Hwang. J, Paik. H Lee. D Anatomical study of the relationship between the sympathetic trunk and intercostal veins of the third and fourth intercostal spaces during thoracoscopy. Clin Anat. 2010: 23(6):702-6.
CrossRef - Ramsaroop L, Singh B, Moodley J, Partab P, Satyapal KS. Anatomical basis for a successful upper limb sympathectomy in the thoracoscopic Clin Anat 2004.17:294–299.
CrossRef - Gossot D, Kabiri H, Caliandro R, Debrosse D, Girard P, Grunenwald D. Early complications of thoracic endoscopic sympathectomy: A prospective study of 940 procedures. Ann Thorac Surg 71:1116–1119.
CrossRef - Reisfeld R, Nguyen R, Pnini A. Endoscopic thoracic sympa- thectomy for treatment of essential hyperhidrosis syndrome: Experience with 650 patients. Surg Laparosc Endosc Percutan Tech 10:5–10.
CrossRef - Rodriguez PM, Freixinet JL, Hussein M, Valencia JM, Gil RM, Herrero J, Caballero-Hidalgo A. Side effects, complications and outcome of thoracoscopic sympathectomy for palmar and axillary hyperhidrosis in 406 Eur J Cardiothorac Surg 2008.34:514–519.
CrossRef - Ueyama T, Matsumoto Y, Abe Y, Yuge O, Iwai T. Endoscopic thoracic sympathicotomy in Japan. Ann Chir Gynaecol 2001.90:200–
- Kim do H, Hong YJ, Hwang JJ, Kim KD, Lee Topographical considerations under video-scope guidance in the T3,4 levels sympathetic surgery. Eur J Cardiothorac Surg 2008.33:786–789.
CrossRef

