
Manuscript accepted on :08-09-2021
Published online on: 17-12-2021
Plagiarism Check: Yes
Reviewed by: Dr. Khalil Alhadidy
Second Review by: Dr. Maha Jalal
Final Approval by: Dr. Francesca Gorini
Jan Hruda1,2 , Martin Helán1,2*, Monika Dvořáková Heroldová3, Milada Dvořáčková3, Lenka Gescheidtová4, Lenka Zdražilová-Dubská4,5, Dalibor Valík4 and Vladimír Šrámek1
, Martin Helán1,2*, Monika Dvořáková Heroldová3, Milada Dvořáčková3, Lenka Gescheidtová4, Lenka Zdražilová-Dubská4,5, Dalibor Valík4 and Vladimír Šrámek1
1Department of Anaesthesiology and Intensive Care, Faculty of Medicine, Masaryk University and St. Anne's University Hospital, Brno, Czech Republic.
2International Clinical Research Center, St. Anne's University Hospital, Brno, Czech Republic.
3Department of Microbiology, Faculty of Medicine, Masaryk University and St. Anne's University Hospital, Brno, Czech Republic.
4Department of Laboratory Medicine, Masaryk Memorial Cancer Institute, Brno, Czech Republic.
5Department of Laboratory Medicine, University Hospital Brno, Czech Republic.
Corresponding Author E-mail: martin.helan@fnusa.cz
DOI : https://dx.doi.org/10.13005/bpj/2286
Abstract
During the first wave of the SARS Cov-2 virus pandemic, we faced a rapidly spreading infection in the Czech Republic. The lack of experience with a pandemic of such magnitude and the inconsistent information on the situation in China and Italy meant that we were forced to introduce an effective anti-epidemic measures in a very short period to protect our patients. One of the key measures that significantly contributed to the successful management of the first wave of the pandemic was to prevent the spread among healthcare professionals who directly cared for patients with active infection. During and after the first wave of the pandemic, we conducted a local observational study to assess the infection rate in ICU health care professionals who were in direct contact with infected patients. We believe that the successful management of the first wave of the pandemic and the experience gained by the entire team will help to manage the further course of this pandemic as well as other epidemics in the future. Here we bring our own experience from University Hospital ICU, which was selected to treat critically ill Covid-19 positive patients from whole region.
Keywords
Covid-19; Health Care Professionals; Infection Protection; ICU; SARS cov-2
Download this article as:| Copy the following to cite this article: Hruda J, Helán M, Heroldová M. D, Dvořáčková M, Gescheidtová L, Dubská L. Z, Valík D, Šrámek V. Strict Adherence to Anti-Epidemic Measures Prevents ICU Staff from SARS-Cov2 Infection. Biomed Pharmacol J 2021;14(4) |
| Copy the following to cite this URL: Hruda J, Helán M, Heroldová M. D, Dvořáčková M, Gescheidtová L, Dubská L. Z, Valík D, Šrámek V. Strict Adherence to Anti-Epidemic Measures Prevents ICU Staff from SARS-Cov2 Infection. Biomed Pharmacol J 2021;14(4). Available from: https://bit.ly/3mf3Iqp |
Introduction
In the Czech Republic, the impending pandemic started to be perceived as a real threat by the end of February 2020, when the Czech Ministry of Health established a special epidemiology committee. All direct flights from China were banned on Feb 9th, those from Italy and South Korea on Mar 5th. The first three patients positive for SARS-CoV-2 were diagnosed in the Czech Republic on 1st March 2020, which led to the activation of the National Security Board and subsequently to the issuance of a series of protective measures. Official rules for compulsory quarantine were issued (Mar 8th) and on Mar 12th, a state of emergency was declared with the closure of all borders, schools, services and stores (except for groceries). Wearing a face mask was declared obligatory.
As a part of the actions taken, our hospital (Saint Anne’s University Hospital from Brno; FNUSA) was declared a “COVID-19 dedicated” hospital during the second week of March, which meant that all SARS-CoV-2 positive patients requiring mechanical ventilation would be admitted from the entire region of Moravia. The doctors in our Intensive Care Unit (ICU) started to work in three separate teams on March 17th and we admitted our first critically ill SARS-CoV-2 positive patient on March 18th. At the time of FNUSA’s designation, the ICU had no special experience in taking care of patients with highly contagious diseases – except for common nosocomial infection prevention.
Experience gained from the current pandemic shows that the protection of healthcare professionals (HCP) against infection is one of the most important conditions for managing a pandemic 1,2. At the same time, we know that health care personnel are subject to a high risk of suffering from a severe course of Covid-19, probably because of their higher viral exposure 3. It is not just that HCPs may become ill and at that moment are unable to provide care, but also there is a serious risk that asymptomatic employees can pass the disease to susceptible patients. One aspect of protecting HCP is to set up effective anti-epidemic measures, including the consistent use of personal protective equipment (PPE). The second question is how and when to test HCP for the presence of the virus 4.
Therefore, we conducted an internal flat testing among all HCPs to evaluate the effectiveness of the staff protection and surveillance strategy. This article summarizes the local experiences with established protective measures, possibilities of HCPs testing and evaluates its effectiveness during the 1st COVID-19 wave.
Staff and Methods
Anti-epidemic measures: hospital organization
The ICU was transformed into a “first-line COVID ICU” with 18 beds available in isolated boxes. Surgical procedures were reduced to emergency cases only, with the intermediate care units then serving as backup for COVID patients. All visits to the hospital were prohibited. The main entrance was the only access to the hospital with all other entrances closed. At the main entrance, only hospital staff were allowed in upon presenting their hospital ID card and undergoing a thermocamera scan. Face masks were obligatory throughout the entire hospital area; the hospital cafeteria and café were closed. Where possible, elevators were locked and dedicated to COVID+ patients only, as was one operating theatre.
Anti-epidemic measures: ICU organisation
All COVID-positive patients were treated inside closed (single sliding door) single-bed isolation boxes. The air conditioning within the unit was reset so that slightly negative pressure was maintained inside the boxes. Access to the ICU was limited to a single two-step entrance.
The doctors in the ICU were divided into three separate teams working in a rota. The doctors from different teams did not meet face-to-face – not even for a handover, which instead was done by a written report sent by e-mail and a short telephone interview. At each team change, the previous team left the ICU shortly before the new team was to arrive. The new team then started the day by cleaning their workspaces (keyboards, cell phones) with antimicrobial wipes. Though no strict bans were issued, it was emphasized that the doctors from different teams should not also meet outside the hospital. We did not establish the same system for the nurses (i.e. complete separation of the teams during shift changes) as this would obviously interfere with the patients’ safety.
Anti-epidemic measures: personal protective equipment (PPE) use
The ICU staff were divided into a 1st line, which provided direct care inside the isolation boxes, and a 2nd line, which provided support throughout the rest of the unit. All personnel who came in direct contact with SARS-CoV-2 positive patients (“1st line”) were equipped with an FFP3 class face mask, goggles, surgical cap, gown and shoes; we used two layers of non-sterile gloves. The 2nd line staff wore scrubs and regular face masks; gloves were not obligatory for them as frequent hand disinfections were required.
In the week prior to admission, we performed repeated training in the use of PPE. We placed particular emphasis on the procedure of how to take off the PPE which we deemed the most dangerous. We also encouraged and practiced a “buddy-check“ procedure – learning to detect flaws in each other’s PPE. We did not outsource these training sessions.
Employees testing
We have established triple testing of all HCPs. First two tests were performed by nasopharyngeal swabs with subsequent PCR and were obligatory to all employees. Swabs of all personnel were taken by two specifically trained employees from deep within the nasopharynx. Finally, to assess whether any of the employees had experienced asymptomatic SARS-Cov2 infection, voluntary testing of specific circulating antibodies was performed (Figure 1).
PCR
The kits used were the Novel Coronavirus (2019-nCoV) Real Time multiplex RT-PCR Kit manufactured by Shanghai ZJ Bio-Tech Co., Ltd. (Liferiver), China. The kit simultaneously detects 3 target genes: the SARS-CoV-2 gene ORF1ab, gene N, and gene E. The thermocycler used was the MIC qPCR cycler manufactured by Bio Molecular Systems, Queensland, Australia.
Blood antibody analysis
Venous blood samples were collected in K3EDTA anticoagulant (S-Monovette, Sarstedt) and plasma was separated by centrifugation for 7 min., 1500 g. The evaluation of anti-SARS-CoV-2 antibodies was performed by the Elecsys Anti-SARS-CoV-2 electrochemiluminiscence assay (ECLIA), measured by a Cobas e411 analyser (both Roche Diagnostics, Germany). The assay uses a recombinant protein representing the nucleocapsid (N) antigen in a double-antigen sandwich assay format. The cut off value was 1 COI (cut-off index); results in the 0.201 – 0.999 range were defined as the grey zone and evaluated by a second test, which also provided typization of IgG/IgM antibodies. The second test was performed by the chemiluminescence immunoassay (CLIA) method by MAGLUMI™ 2019-nCov IgM and IgG assays, measured by a Maglumi 800 analyser (both Snibe Diagnostics, China). IgM immunoassay is a capture CLIA exploiting magnetic beads coated with an anti-human IgM antibody and a virus recombinant antigen with a luminescent label. IgG immunoassay is an indirect CLIA detecting antibody in a diluted specimen using magnetic beads coated with a virus recombinant antigen and an anti-human IgG antibody with a luminescent label. The structural characteristics of antigens (e.g. nucleocapsid, spike protein etc.) used in the Maglumi assays were the manufacturer’s trade secret. The interpretation of the result recommended from manufacturer was “non-reactive” for concentrations <1.00 AU/ml and “reactive” for concentrations ≥1.00 AU/ml for both IgM and IgG.
Results
During the first surge of the SARS-CoV-2 pandemic, we treated 16 patients in a life-threatening condition with a PaO2/FiO2 ratio of 111,0 ± 34,3 (mean ± SD). The age of the patients was 67,9 ± 9,7 years (mean ± SD), and 14 (87,5 %) patients were males. All patients required intubation and aggressive mechanical ventilation. Four patients required extracorporeal oxygenation (ECMO). The length of stay in our ICU was 12,4 ± 4,3 (mean ± SD) days and 8 patients died (i.e. 50% mortality). The highest number of patients we treated at the same time was 10 (Figure 1).
Only three patients became SARS-CoV-2 negative during their stay in our ICU (a negative PCR test and retest – see above); this happened after 15, 25 and 39 days after ICU admission. In one of these patients, a regular check-up PCR test was negative, but the confirmatory test within 48hrs came back as positive again. This patient had one more positive test 2 days later and finally became negative after 10 more days. The remaining 13 patients stayed SARS-CoV-2 positive throughout their entire stay.
The timeline of the healthcare personnel check-up is presented in Figure 1. During both PCR testing periods from nasopharyngeal swabs, all departmental employees without exception were tested, specifically: 41 doctors, 68 nurses, 9 orderlies, 5 volunteering medical students, 3 technicians and 3 cleaners from the ICU plus 4 pain management nurses and 33 anaesthesiologic nurses. None of these employees was tested positive in the either first or second phases.
In order to verify whether anyone had not acquired an asymptomatic coronaviral infection, we tested specific peripheral blood antibodies at the end of the first wave of the pandemic. Even though this was a voluntary testing (as opposed to swabs), 99 (out of 149; 66.4 %) employees got tested from 18th June to 29th June 2020. All samples were reported after the first test (see the methods section) as “non-reactive” (measured values < 0.2 COI); only one result was in the grey zone with subsequent non-reactive results in the second test for both IgG and IgM anti-SARS-CoV-2 antibodies.
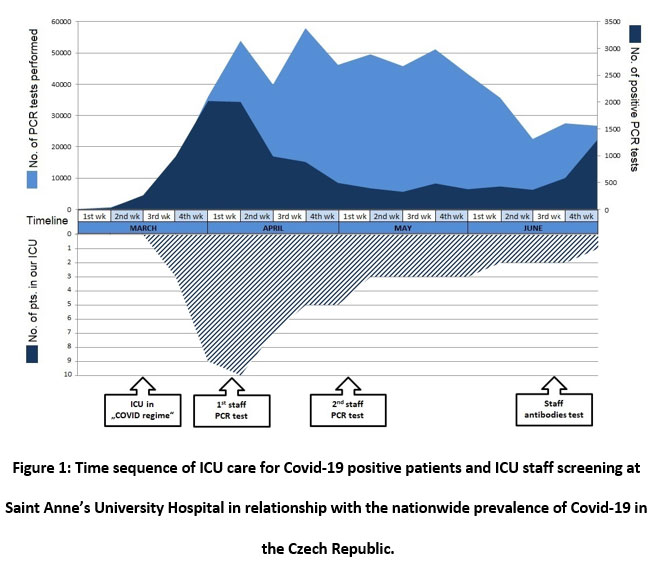 |
Figure 1: Time sequence of ICU care for Covid-19 positive patients and ICU staff screening at Saint Anne’s University Hospital in relationship with the nationwide prevalence of Covid-19 in the Czech Republic. |
Discussion
Protecting employees is undoubtedly one of the cornerstones of caring for patients during a pandemic (1,2). Based on our own experience from the first wave of the coronavirus pandemic, we can responsibly state that rapid adoption and strict adherence to anti-epidemic measures reduced the risk of infection of ICU personnel to a minimum. During a more than 3-month period of caring for Covid-positive critically ill patients, none of the staff became ill with the Covid-19 disease and in fact, no one was infected by the SARS-CoV2 virus. Therefore, we consider our anti-epidemic measures to be adequate and sufficient. Another finding is that self-education in the use of PPE is feasible. Here, it is appropriate to cooperate with a second colleague who observes the dressing process and evaluates the final state of the PPE just before entering the isolation box (“buddy-check”). Also, the manner of testing for infected individuals among our own employees using a combination of nasal swab PCR and detecting circulating antibodies proved to be successful. At the same time, it is clear that a responsible approach taken by every employee must be maintained not only in the work environment, but also outside the hospital. However, this is difficult to ensure by any systemic measure, so a general protective policy in society is necessary.
Another aspect of protecting employees during a pandemic is to support their mental health. Although the onset of the pandemic was psychologically demanding, we did not experience any such problems. One reason was certainly that the first wave lasted a relatively short time. Also, people were soon reassured that the situation could be managed and that no one had become infected. The division of the team into separate shifts and restrictions on normal hospital operations gave employees enough time to take a rest. Finally, public support and respect for healthcare professionals also had a positive effect.
It has remained a subject of debate why the pandemic developed into a health care disaster in Italy 5,6, while progressing in a much more manageable manner n other countries including the Czech Republic. For comparison, in Italy during the first wave 18 % of the tested HCPs came out positive 5. It is highly likely that multiple factors contributed to these differences. The strain of SARS-CoV-2 could have been slightly different as multiple strains are spreading 7,8. Some data also suggest a beneficial effect of the BCG vaccination, which had been widely used in the Czech Republic 9,10. The active social life of the senior population in Italy may have led to a greater proportion of elderly COVID-19 patients compared to other countries 11. It is also of great importance that warning had come earlier to the Czech Republic before the first cases occurred and more information was available at the time of the outbreak in our country.
We verified that strict adherence to anti-epidemic rules by the entire team is temporarily possible. Unfortunately, during later pandemic waves with gradually increasing number of infected individuals, it was no longer possible to establish measures on such a high level as in the first wave. For economic and organizational reasons, it was not possible to completely stop the admission of outpatients and planned surgical operations. It was necessary to set a compromise to what extent to limit normal hospital operations and to what extent to introduce anti-epidemic measures to ensure continuous care for patients, but at the same time not to put them at disproportionate risk during their hospital stay. This still presents a difficult challenge in the fight against the current pandemic.
Conclusion
Even healthcare professionals who come in daily contact with critically infected infectious patients can be effectively protected against Covid-19 infection by strictly adhering to well-established anti-epidemic measures. Organized testing of staff can provide valuable feedback on the effectiveness of such measures. We do believe that our experience with treating SARS-CoV-2 positive patients can provide both information and motivation to those teams who will have to face this challenge in the oncoming outbreaks.
Acknowledgment
We would like to acknowledge all the staff of the Department of Anesthesiology and Intensive Care of Saint Anne’s University Hospital for their outstanding commitment and dedication in managing the Covid-19 pandemic.
Conflict of Interest
None of the authors has a conflict of interest.
Funding Sources
This work was supported by the National Program of Sustainability II (The Ministry of Education, Youth and Sports of Czech Republic; LQ1605).
References
- Godderis L, Boone A, Bakusic J. COVID-19: a new work-related disease threatening healthcare workers. Occup Med (Lond). 2020;70(5):315-316. doi: 10.1093/occmed/kqaa056.
CrossRef - Chen W, Huang Y. To Protect Health Care Workers Better, To Save More Lives With COVID-19. Anesth Analg. 2020;131(1):97–101.
CrossRef - Gibson DM, Greene J. Risk for Severe COVID-19 Illness Among Health Care Workers Who Work Directly with Patients. J Gen Intern Med. 2020;1–3.
CrossRef - Rivett L, Sridhar S, Sparkes D, Routledge M, Jones NK, Forrest S, et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife. 11 2020;9.
- Felice C, Di Tanna GL, Zanus G, Grossi U. Impact of COVID-19 Outbreak on Healthcare Workers in Italy: Results from a National E-Survey. J Community Health. 2020;45(4):675-683. doi: 10.1007/s10900-020-00845-5.
CrossRef - Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet 2020;2:10–13.
CrossRef - Koyama T, Platt D, Parida L. Variant analysis of SARS-CoV-2 genomes. Bull World Health Organ. 2020;98(7):495–504.
CrossRef - Ludwig S, Zarbock A. Coronaviruses and SARS-CoV-2: A Brief Overview. Anesth Analg. 2020;131(1):93–6.
CrossRef - O’Neill LAJ, Netea MG. BCG-induced trained immunity: can it offer protection against COVID-19? Nat Rev Immunol. 2020;20(6):335–7.
CrossRef - Netea MG, Giamarellos-Bourboulis EJ, Domínguez-Andrés J, Curtis N, van Crevel R, van de Veerdonk FL, et al. Trained Immunity: a Tool for Reducing Susceptibility to and the Severity of SARS-CoV-2 Infection. Cell. 28 2020;181(5):969–77.
CrossRef - Di Lorenzo G, Di Trolio R. Coronavirus Disease (COVID-19) in Italy: Analysis of Risk Factors and Proposed Remedial Measures. Front Med. 2020;7:140.
CrossRef

