
Manuscript accepted on :17-04-2021
Published online on: 18-05-2021
Plagiarism Check: Yes
Reviewed by: Dr. Sonali Tripathy
Second Review by: Dr. Adibah Hanim Ismail
Final Approval by: Dr Ayush Dogra
V.Chitra and Evelyn Sharon.S*
Department of Pharmacology, SRM College of Pharmacy, SRM IST. India
Corresponding Author E-mail: evelynsharonsukumar@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2159
Abstract
Osteoporosis is the multifactorial skeletal disease that leads to fracture risk in individuals. It is characterized by a decrease in bone mineral density leading to increased fracture risk. It is often silent and only known when fractures occur in the elderly leading to death. The reason is that the disease is always underdiagnosed and not treated properly. It affects men and women, but women are more susceptible to it due to estrogen deficiency. Osteoporosis is diagnosed based on the fragility fractures, low bone mineral density assessed by DEXA scan. Pharmacological (anti-resorptive and anabolic drugs) and lifestyle modifications (dietary intake, weight-bearing exercise, hip protectors, and fall prevention measures) are helpful in the prevention and treatment of Osteoporosis. Clinicians must take proper measures in finding out the patients who are at higher risk of Osteoporosis and providing treatment by either diagnosing or by screening the previous history of fracture risk in the patients. This article provides an overview of the diagnosis, screening, and treatment of Osteoporosis.
Keywords
Bone Mineral Density; Estrogen Deficiency; Fracture Risk; Lifestyle Modification; Osteoporosi; Pharmacological Treatment
Download this article as:| Copy the following to cite this article: Chitra V, Sharon S. E. Diagnosis, Screening and Treatment of Osteoporosis – A Review. Biomed Pharmacol J 2021;14(2). |
| Copy the following to cite this URL: Chitra V, Sharon S. E. Diagnosis, Screening and Treatment of Osteoporosis – A Review. Biomed Pharmacol J 2021;14(2). Available from: https://bit.ly/2SZVI0T |
Introduction
Osteoporosis means “POROUS BONES” which is characterized by loss of bone mass over time leading to fragility fractures. It is an age-related health problem which threatens the mobility and increases mortality in the elderly population. Both men and women are affected by this bone disorder. It makes their bone fragile and weak leading to fragility fractures with trivial trauma. These fractures might cause pain, discomfort and disability (Macnair, 2016). The occurrence of osteoporosis is more in women when compared to men. In women, it is due to estrogen deficiency which takes place during the menopause period. According to the ICMR reports it was said that 3% of the Indian men and 8% of the female population in India are Osteoporotic (Dalvi, Sathe and Chawan, 2007). Based on the census reports out of 163 million aged population 20 % are women and the remaining 10 -15% are men affected by Osteoporosis in India (Mithal and Malhotra, 2006). Further studies have revealed that Indians had a low bone mineral density when compared to their Western Counterparts due to hereditary factors, nutritional deficiencies, and smaller skeletal size. Results show that there is a great lack of knowledge about the awareness of Osteoporosis (Gopinathan, Sen, Behera, and Aggarwal, 2016). This is more among women in India where they are not aware of the condition and the means to prevent it. Clinicians need to be more interested in initiating primary prevention measures for the treatment and prevention of Osteoporosis among people who are at high risk. They must diagnose the disease either by screening or identifying the previous history of fractures. This article will provide an overview of the diagnosis, screening, and treatment options available for Osteoporosis.
Definition
Osteoporosis is a disease characterized by low bone mass, loss of the bone tissue, and destruction of the bone microarchitecture. In course of time, it leads to compressed bone strength leading to increased fracture risk (Sözen, Özışık and Başaran, 2017) (Sozen, Ozisik and Calik Basaran, 2017) (Srivastava, Mukerjee, Gupta and Srivastava, 2014). According to World Health Organization Osteoporosis is defined as “ When the value of the Bone mineral density is 2.5 Standard deviations or more below the mean of the young adult reference range(Mitlak and Nussbaum, 1993) (Sipos, Pietschmann, Rauner, Kerschan-schindl and Patsch, 2009). Osteoporosis is classified into two types namely Primary and Secondary( Fig1). Primary is further classified into two types namely Type 1 and Type 2 and Secondary osteoporosis is due to various chronic medical conditions, medications, and nutritional deficiencies(Sözen et al., 2017). Some common causes of secondary Osteoporosis associated with various conditions are outlined in table 1.
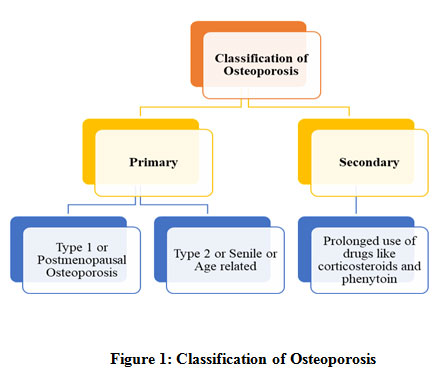 |
Figure 1: Classification of Osteoporosis. |
Table 1: Classification of Osteoporosis based on the scores.
| World Health Organization Classification of T Score for Osteoporosis | |
| Normal | BMD ≥ – 1.0 |
| Osteopenia (Low Bone Mass) | BMD ≥ – 2.5 and ≤ – 1.0 |
| Osteoporosis | BMD ≤ – 2.5 |
| Severe Osteoporosis | BMD ≤ – 2.5 with previous history of fragility fractures |
Diagnosis
Till 1993 there were no proper diagnosing methods for Osteoporosis. The incidence of fragility fractures was the only indication for the diagnosis of Osteoporosis. After the year 1994 WHO established definitions for Osteoporosis to help researchers and physicians to categorize the degree of bone loss among the patients mentioned in Table 2. The most common and the standard test for the evaluation of Osteoporosis are the measurement of:
Serum calcium
Renal function
Vitamin D3 levels
Alkaline phosphatase
Parathyroid Hormone levels
Thyroid function test
Table 2: Test for the diagnosis of Osteoporosis
| Tests | Men | Values | Women | Values |
| Serum Calcium Levels | ˃59 years – | 8.7 – 10.2 (mg/dL) | ˃59 years | 8.7 – 10.3 |
| Vitamin D3 Levels | ˃59 years | 600 (IU) | ˃59 years | 800 (IU) |
| Parathyroid Hormone Levels | ˃59 years | 76.8 pg/ml | ˃59 years | 77.6pg/ml |
| Alkaline Phosphatase Levels | ˃59 years | 80 – 302 (IU) | ˃59 years | 64 – 302 (IU) |
| Renal Function Test ( Creatinine) | ˃59 years | 8.4 – 25.9 (mg/day) | ˃59 years | 5.3 – 14.9 (mg/day) |
| Thyroid Function Test | ˃59 years | 0.5 – 5.49mIU/L | ˃59 years | 0.4 – 4.0 mIU/L |
Apart from the above test DEXA (Dual X-ray Absorptiometry) scan is used for the measurement of bone mineral density. DEXA scan has been the golden standard method for the diagnosis of osteoporosis (Juli, 2016). FRAX ( Fracture Risk Assessment Tool) is a computer-based algorithm developed by the WHO that calculates the probability of fracture risk in Osteoporosis candidates above the age of 50 years. The decision to treat is based on the risks, FRAX tool calculations, patient compliance, and health benefits. Patients with a previous history of the fracture risk must take the medication on the advice of the doctor and must not withdraw the medication on their own. Periodically they must be evaluated for their BMD especially women.
Screening for Osteoporosis
Older adults who are considered to be at higher risk of Osteoporosis must be screened periodically. They must be evaluated for fracture risk also. Patients who have been identified to be at higher risks must have a routine physical examination, BMD testing, and laboratory general testing to avoid further pain. The medical history obtained must completely focus on the risk of having low bone mineral density and the risk of falls. When the patients come on for the regular check-up his or her previous history of fractures due to falls, smoking, and alcohol intake details, menopausal status, and medication history must be taken and recorded.
The physical examination must include the height, weight, and body mass index so that any loss of height can be determined. BMI less than 21 kg/m² and loss of 5 cm or more are considered as a risk factor for Osteoporosis. The presence of gait disorder, weakness, and postural instability are considered as factors that increase the risk of fractures and falls. The presence or any signs of Thoracic kyphosis might lead to vertebral fractures.
Lifestyle Changes to Reduce Bone Loss
Patients with Osteoporosis must be advised on lifestyle changes to reduce the incidence of fractures and bone loss. Lifestyle modifications including eating a well-balanced diet with are rich in calcium and vitamin D, limiting the intake of tobacco and alcohol consumption having enough exposure to sunlight and maintaining regular physical activity should be followed.
Weight-bearing exercise
Exercise is considered an effective measure in maintaining the bone density in the lumbar spine but so far no evidence is available on it is proving to decrease the fracture risk. Few reports suggest that regular exercise can produce some benefit in Postmenopausal women in terms of their bone mineral density(Chow, Harrison, & Notarius, 1987), but the thing is that they are not able to prevent the normal Postmenopausal bone loss(Howe et al., 2011). Reports have also shown that the benefits obtained by regular exercise are lost rapidly when a sedentary lifestyle is resumed back (Dalsky et al., 1988). Exercise such as walking and aerobics can be done. Regular exercise has been found to increase muscle mass, strength in improving balance, coordination, and even reduced the risk of fractures and falls by about 25% in the elderly population (Taaffe, Duret, Wheeler, & Marcus, 1999).
Patients who are not Osteoporotic must be encouraged to take up weight-bearing exercise to gain fitness and prevent future risk of falls and fractures. Good examples of exercise such as walking, jogging, playing tennis can be done. In patients with Osteoporosis, the above jarring movements have to be avoided. Thus exercise is to be considered as an adjuvant rather than an alternative in the treatment of Osteoporosis.
Prevention of fall
Falls in the elderly population is more common due to their advancing age (Prudham D and Jg, 1981), especially more common in women. The risk factors that lead to fall fractures are chronic ill health, cognitive impairment, visual impairment, poor balance, multiple medications, wearing inappropriate footwear, hazardous environmental arrangements, and muscle weakness (Tinetti, Speechley andGinter, 1988). To avoid the risk factors physical therapy to improve the strength and balance can be given, avoiding medications that alter the mental health and in terms of environmental hazards shoes with non-skid soles can be given, placing non-slip mats and rugs, installing grab bars in the wash area, steps, showers and removing any non-essential things in the living area and in the other places where elders stay. Studies have reported that vitamin D supplementation was found to reduce the risk of falls by 20% in the elderly population (Ringe, 2012)(Dhaliwal and Aloia, 2017).
Hip protectors
This is an additional approach to the prevention of hip fractures. Hip protectors are rigid inserts that are used to prevent direct trauma to the hip. The hip protectors must be helpful in the bed-ridden elderly population. No evidence is effective in using hip protectors for pelvic fractures. Compliance on its long term use is very poor (Lauritzen, Petersen Lund, 1993)(Parker, Gillespie and Gillespie, 2005).
Calcium & Vitamin D
With aging, there is a drastic decline in calcium absorption in both men and women. This consequently leads to the loss of intestinal vitamin D receptors. The diet we take i.e the amount and consumption, the climatic condition, and race influences the calcium absorption. Vitamin D obtained in the form of diet and maximum sun exposure. The best indication for the vitamin D status is through serum 25-hydroxy vitamin D (25 OHD) levels. This serum 25 OHD levels are found to be lower in individuals who use sunscreens and in individuals with pigmented skin. Serum 25OHD levels eventually decline with aging due to many reasons. One among them is as the other people spend less time outdoors. The intestinal absorption of vitamin D does not get impaired with aging has been reported previously. Studies have shown that vitamin D supplementation may prevent bone loss and mildly increase the BMD in the elderly but does not reduce the vertebral and non-vertebral risk fracture in vitamin D deficient individuals (IJsselmuiden and Faden, 1992). Dietary intake of vitamin D of about 400 to 600 IU is recommended for individual’s age 50 years and above (Bischoff-Ferrari et al., 2005).
The best source of calcium is from dairy products such as milk, yogurt, and cheese. Few fruits and veggies also contain calcium in smaller amounts. The amount of calcium needed for women age 51 years and older is 1200 mg daily as per the guidelines (Aggarwal and Nityanand, 2013). Calcium supplements may prevent bone loss in women but no evidence is available on it saying that it decreases the fracture risk in patients with Osteoporosis (Peacock et al., 2000). It is very much evident that there is just a small increase in bone mineral density when calcium supplements are given. It is still controversial regarding the benefit of calcium intake toward bone health. When given in combinations with vitamin D it might have a beneficial role in the treatment of osteoporosis among the elderly population.
Pharmacological Treatment Of Osteoporosis
The drug treatment for Osteoporosis can be broadly classified into two types namely those that retard bone resorption (estrogens, calcitonin, and bisphosphonates) and those that stimulate bone formation ( teriparatide and strontium ranelate). The main goal of pharmacological therapy in Osteoporotic patients is not only to increase the bone density but to reduce the incidence of future fracture risk. The elderly with Osteoporosis are given pharmacological treatment based on 3 categories:
Patients with BMD “T” score below – 2.0 .
Patients with BMD below -1.5 with additional risk factors arising due to long term use of corticosteroid therapy, smoking and alcohol consumption, previous history of fractures during childhood .
Elderly osteoporotic patients with the previous history of vertebral or hip fractures.
Bisphosphonates
They are the first-line therapy given for Osteoporosis. Bisphosphonates are analogs of the pyrophosphate family that bind to the surface of the bones and inhibit the Osteoclastic activity. The FDA has approved only three bisphosphonates such as alendronate, risedronate, and ibandronate. The dosage for the use of the bisphosphonate drug is given in the below table 3. In case when a patient cannot tolerate the Oral intake of Bisphosphonates he/she is given Idronate and Zoledronic acid by Intravenous injections. These two drugs are not FDA approved they are used occasionally when the patient cannot tolerate the oral intake. Reports have shown that drugs like alendronate, risedronate, and ibandronate have shown to have reduced vertebral and hip fractures by 50 % – 60% in postmenopausal women(&NA; 1996)(Siris, Simon, Barton, McClung, and Grauer, 2008).
Patients who take oral bisphosphonates must be advised to take the tablet with 6 to 8 ounces of water in an empty stomach. The patient should not lie down for at least 30 minutes to avoid esophageal injury (Chesnut et al., 2004). If there is any difficulty in swallowing or discomfort like heartburn the drug can be withdrawn immediately and an alternate bisphosphonate can be prescribed. Oral bisphosphonates must be carefully prescribed in patients who have difficulty in swallowing, have previous complaints of esophageal reflux, patients who have undergone gastric surgery.
Table 3: Bisphosphonate drugs approved by FDA
| DRUGS | TREATMENT | PREVENTION |
| Alendronate | 10 mg/day | 5mg/day |
| Ibandronate | – | 2.5mg/day |
| Risedronate | 5mg/day | 5mg/day |
Raloxifene
The risk of breast cancer in the long term use of estrogen leads to the development of selective estrogen receptor modulators (SERMs). Raloxifene is a SERMs approved by the FDA for the prevention and treatment of Osteoporosis. It is a non- steroidal benzothiophene derivative that inhibits bone mineral density loss. It is given at a dose of 60 mg/day. It selectively interacts with the estrogen receptors showing the agonistic estrogen effects in bone tissues and as antagonistic estrogen in the breast and uterus tissues (Johnston et al., 2000). Reports show that there was a 50% reduction of the vertebral fractures and there was an increase in the bone mineral density in the lumbar spine, total hip, and femoral neck of the patients who received it (Ettinger et al., 1999).
Due to its selective actions against the estrogen receptors, they have shown to reduce the risk of breast cancer and prevent the chances of getting cardiovascular disease (Krul et al., 2015). The common side effect of Raloxifene is the increased risk of venous thromboembolism and increased vasomotor symptoms. It is not recommended in postmenopausal women who were previously given estrogen replacement therapy.
Calcitonin
It is given in the form of a nasal spray. An FDA approved drug for the treatment of Osteoporosis given at a dose of 200IU in alternating nostrils each day. It directly suppresses the activity of Osteoclasts thereby preventing bone loss and vertebral fractures (Gennari, 1989). Proper reports are not available on their use in the prevention of vertebral and hip fractures (Chesnut et al., 2000)(Overgaard, Hansen, Birk Jensen, & Christiansen, 1992). They are not contraindicated with any kind of hypersensitivity. The only side effect is the nasal rhinitis in 12% of the patients who used it. With the availability of the other drugs and better efficacy in Fracture risk reduction, Calcitonin is not generally the first-line treatment considered for Osteoporosis.
Hormonal replacement therapy/estrogen replacement therapy
It is used as a prophylactic measure and has shown to reduce the frequency of Osteoporotic fractures. But its role in the prevention and treatment of Osteoporosis remains unclear and controversial. Estrogens may reduce the risk of fractures by increasing mobility and dexterity. But their action is on bone density and bone turnover. Reports have shown that estrogen maintained vertebral disc height, showed shock-absorbing capacity which helped in reducing the vertebral fracture risk (Baron, Brincat, Galea, & Calleja, 2005). In few other studies, it was reported that estrogen when given alone (Anderson & Limacher, 2004) or in combination with progesterone showed a drastic decrease in bone loss and the fracture risk (Cauley et al., 2003). The revised FDA guidelines suggested that estrogen products can be given to Osteoporosis patients only for the prevention that too only for a shorter period. Combination estrogen therapy is associated with increased risk of Coronary heart disease, stroke, venous thromboembolism (Cauley et al., 2003), whereas estrogen therapy alone is associated with increased coronary heart disease and breast cancer.
Withdrawing estrogen therapy without proper care suddenly might lead to bone loss double the time it has been gained in Postmenopausal women (Kaye, n.d.)(Wasnich et al., 2004). Transdermal estrogen therapy has gained popularity in recent times. It was found that it produced similar effects to that of oral therapy. The transdermal patch increased the bone mineral density in the spine of the Postmenopausal women (Riis, Thomsen, Strøm, & Christianse, 1987). In a study to access the spine and hip bone density in Postmenopausal women with the transdermal patch, it was found that there was a reduction in bone turnover and an increase in the femoral and vertebral bone mineral density was observed (Hillard et al., 1994).
Using Hormonal Replacement Therapy in early Postmenopausal Women might result in decreased fracture risk in the later years of life. In randomized clinical study women who were given HRT had reduced fracture risk when compared with the patients who received placebo treatment (Bagger et al., 2004). Reports have suggested that there was a reduction of the hip fractures in women above the age of 75 years when estrogen treatment was given.
In summary, HRT is an effective treatment in the prevention and treatment of vertebral and non-vertebral fracture risk (Stevenson et al., 2006). Meta-analysis has reported that with the use of HRT there was a 33% reduction in the vertebral fractures and a 27% reduction in non-vertebral fractures (D. J. Torgerson & Bell-Syer, 2001)(David J. Torgerson & Bell-Syer, 2001). When HRT is being started in the early menopause stage it might help build up the bone mass and prevent future fracture risk (Bagger et al., 2004)(Ettinger et al., 2004).
Teriparatide
The first anabolic drug approved for the treatment of Osteoporosis by the FDA is Teriparatide. Teriparatide is the name given to recombinant parathyroid hormone therapy. PTH is an 84 amino acid peptide hormone analog that increases bone turnover. They are given to Postmenopausal patients with severe bone loss and patients who are at higher risk of fractures (Neer et al., 2001). It increases the serum calcium reducing the renal excretion thus mobilizing bone calcium by increasing the Osteoclastic resorption(Kalu, 1970).
Studies have shown that intermittent use of this drug by subcutaneous injection had a beneficial effect on the bone mineral density and fracture risk in Postmenopausal Osteoporotic women(Neer et al., 2001)(Lindsay et al., 1997). When compared to the other therapies Teriparatide has been found to increase and improve skeletal architecture including the trabecular.
Connectivity (Dempster et al., 2001). Daily subcutaneous administration of 20µg of Teriparatide is used for the treatment of Osteoporosis. Due to its high cost, it is mostly given in patients who are at a higher risk of fractures and who don’t respond to other therapies. It is a well-tolerated drug. The common side effects are headache, nausea, dizziness, mild hypercalcemia, and hypercalciuria are seen (Eriksen, Keaveny, Gallagher, & Krege, 2014).
Conclusion
Osteoporosis is becoming a life-threatening health issue in recent times due to its increase in fracture risk. The main problem is it is often under recognized and untreated which leads to an increase in fracture risk. Patients at a high risk of fractures don’t get enough evaluation for the disease or get proper treatment. The serious issue is that patients who are diagnosed with Osteoporosis and having low BMD levels are not evaluated or given proper treatment for the cure of the disease. With the recent reports, it is well known that women are at higher risk than men due to the estrogen deficiency after their menopause.
There is not much data on the proper screening techniques available for the treatment of Osteoporosis. The role of risk factor assessment, different bone density techniques, the frequency of screening, and the groups to whom the treatment can be made effective remains unclear. Estrogen therapy is available for the prevention and treatment of Osteoporosis. Calcium and vitamin D intake from fruits and vegetables is also recommended with extra supplementation to increase the bone mineral density. But still there exists a gap in treating and preventing Osteoporosis. And the biggest challenge is to educate the patients about Osteoporosis, assessing the risk factors, facilitating the screening methods, and administering the proper drug to the proper patients at the right time to prevent future and severity of the fracture risk.
Conflict of Interest
None
References
- Aggarwal, S., & Nityanand. (2013). Calcium and vitamin D in postmenopausal women. Indian Journal of Endocrinology and Metabolism, 17(9), 618. https://doi.org/10.4103/2230-8210.123549
CrossRef - &NA; (1996). Effect of Oral Alendronate on Bone Mineral Density and the Incidence of Fractures in Postmenopausal Osteoporosis. The Endocrinologist, 6(3), 271. https://doi.org/10.1097/00019616-199605000-00025
CrossRef - Anderson, G. L., & Limacher, M. (2004). Effects of Conjugated Equine Estrogen in Postmenopausal Women with Hysterectomy: The Women’s Health Initiative Randomized Controlled Trial. Journal of the American Medical Association, 291(14), 1701–1712. https://doi.org/10.1001/jama.291.14.1701
CrossRef - Bagger, Y. Z., Tankó, L. B., Alexandersen, P., Hansen, H. B., Møllgaard, A., Ravn, P., … Christiansen, C. (2004). Two to three years of hormone replacement treatment in healthy women have long-term preventive effects on bone mass and osteoporotic fractures: The PERF study. Bone, 34(4), 728–735. https://doi.org/10.1016/j.bone.2003.12.021
CrossRef - Baron, Y. M., Brincat, M. P., Galea, R., & Calleja, N. (2005). Intervertebral disc height in treated and untreated overweight post-menopausal women. Human Reproduction, 20(12), 3566– 3570. https://doi.org/10.1093/humrep/dei251
CrossRef - Bischoff-Ferrari, H. A., Willett, W. C., Wong, J. B., Giovannucci, E., Dietrich, T., & Dawson-Hughes, B. (2005). Fracture Prevention With Vitamin D Supplementation. Jama, 293(18), 2257. https://doi.org/10.1001/jama.293.18.2257
CrossRef - Cauley, J. A., Robbins, J., Chen, Z., Cummings, S. R., Jackson, R. D., LaCroix, A. Z., … Watts, N. B. (2003). Effects of Estrogen Plus Progestin on Risk of Fracture and Bone Mineral Density: The Women’s Health Initiative Randomized Trial. Journal of the American Medical Association, 290(13), 1729–1738. https://doi.org/10.1001/jama.290.13.1729
CrossRef - Chesnut, C. H., Silverman, S., Andriano, K., Genant, H., Gimona, A., Harris, S., … Baylink, D. (2000). A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The prevent recurrence of osteoporotic fractures study. American Journal of Medicine, 109(4), 267–276. https://doi.org/10.1016/S0002-9343(00)00490-3
CrossRef - Chesnut, C. H., Skag, A., Christiansen, C., Recker, R., Stakkestad, J. A., Hoiseth, A., … Delmas, P. D. (2004). Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. Journal of Bone and Mineral Research, 19(8), 1241–1249. https://doi.org/10.1359/JBMR.040325
CrossRef - Chow, R., Harrison, J. E., & Notarius, C. (1987). Effect of two randomized exercise programs on bone mass of healthy postmenopausal women. British Medical Journal (Clinical Research Ed.), 295(6611), 1441–1444. https://doi.org/10.1136/bmj.295.6611.1441
CrossRef - Dalsky, G. P., Stocke, K. S., Ehsani, A. A., Slatopolsky, E., Lee, W. C., & Birge, S. J. (1988). Weight-bearing exercise training and lumbar bone mineral content in postmenopausal women. Annals of Internal Medicine, 108(6), 824–828. https://doi.org/10.7326/0003-4819-108-6-824
CrossRef - Dalvi, H., Sathe, R., & Chawan, S. (2007). Assessment of Prevalence of Osteoporosis in Adult Population in. Icmr, 167–177.
- Dempster, D. W., Cosman, F., Kurland, E. S., Zhou, H., Nieves, J., Woelfert, L., … Lindsay, R. (2001). Effects of daily treatment with parathyroid hormone on bone microarchitecture and turnover in patients with osteoporosis: A paired biopsy study. Journal of Bone and Mineral Research, 16(10), 1846–1853. https://doi.org/10.1359/jbmr.2001.16.10.1846
CrossRef - Dhaliwal, R., & Aloia, J. F. (2017). Effect of Vitamin D on Falls and Physical Performance. Endocrinology and Metabolism Clinics of North America, 46(4), 919–933. https://doi.org/10.1016/j.ecl.2017.07.004
CrossRef - Eriksen, E. F., Keaveny, T. M., Gallagher, E. R., & Krege, J. H. (2014). Literature review: The effects of teriparatide therapy at the hip in patients with osteoporosis. Bone, 67, 246–256. https://doi.org/10.1016/j.bone.2014.07.014
CrossRef - Ettinger, B., Ensrud, K. E., Wallace, R., Johnson, K. C., Cummings, S. R., Yankov, V., … Grady, D. (2004). Effects of ultralow-dose transdermal estradiol on bone mineral density: A randomized clinical trial. Obstetrics and Gynecology, 104(3), 443–451. https://doi.org/10.1097/01.AOG.0000137833.43248.79
CrossRef - Ettinger, B., Mitlalc, B. H., Nickelsen, T., Genant, H. K., Christiansen, C., Zanchetta, J. R., & Stakkestad, J. (1999). Reduction of Vertebral Fracture Risk in Postmenopausal Women With Osteoporosis Treated With Raloxifene. Jama, 282(7), 637–645.
CrossRef - Gennari, C. (1989). Salmon calcitonin (Miacalcic) nasal spray in prevention and treatment of osteoporosis. Clinical Rheumatology, 8(2 Supplement), 61–65. https://doi.org/10.1007/BF02207236
CrossRef - Gopinathan, N. R., Sen, R. K., Behera, P., & Aggarwal, S. (2016). Awareness of osteoporosis in postmenopausal Indian women : An evaluation of Osteoporosis Health Belief Scale, 180– 184. https://doi.org/10.4103/0976-7800.195697
CrossRef - Hillard, T. C., Whitcroft, S. J., Marsh, M. S., Ellerington, M. C., Lees, B., Whitehead, M. I., & Stevenson, J. C. (1994). Long-term effects of transdermal and oral hormone replacement therapy on postmenopausal bone loss. Osteoporosis International, 4(6), 341–348. https://doi.org/10.1007/BF01622195
CrossRef - Howe, T. E., Shea, B., Dawson, L. J., Downie, F., Murray, A., Ross, C., … Creed, G. (2011). Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database of Systematic Reviews, 2011(7), 1–167. https://doi.org/10.1002/14651858.CD000333.pub2.
CrossRef - IJsselmuiden, C. B., & Faden, R. R. (1992). The New England Journal of Medicine Downloaded from nejm.org on January 31, 2011. For personal use only. No other uses without permission. Copyright © 1992 Massachusetts Medical Society. All rights reserved., 326.
- Johnston, C. C., Bjarnason, N. H., Cohen, F. J., Shah, A., Lindsay, R., Mitlak, B. H., … Delmas, P. D. (2000). Long-term effects of raloxifene on bone mineral density, bone turnover, and serum lipid levels in early postmenopausal women: Three-year data from 2 double-blind, randomized, placebo-controlled trials. Archives of Internal Medicine, 160(22), 3444–3450. https://doi.org/10.1001/archinte.160.22.3444
CrossRef - Juli. (2016). Osteoporosis: A review. Research Journal of Pharmaceutical, Biological and Chemical Sciences, 7(4), 2853–2856. https://doi.org/10.3329/birdem.v5i1.28371
CrossRef - Kalu, D. N. (1970). PTH und Osteosklerose. The Journal of Infectious Diseases, 202(11), 1659– 1666. https://doi.org/10.1086/657158
CrossRef - Kaye, J. (n.d.). Tachycardia Throughout. Group, 1325–1327.
- Krul, I. M., Sc, M., Lugtenburg, P. J., Ph, D., Leeuwen, F. E. Van, & Ph, D. (2015).new England Journal, 1609–1619. https://doi.org/10.1056/NEJMoa1505949
CrossRef - Lauritzen, J. B., Petersen, M. M., & Lund, B. (1993). Effect of external hip protectors on hip fractures. The Lancet, 341, 11–13. https://doi.org/http://dx.doi.org/10.1016/0140-6736(93)92480-H
CrossRef
Abbreviations
| BMD | Bone mineral density |
| HRT | Hormonal replacement therapy |
| PTH | Parathyroid hormone |
| IU | International units |
| FDA | Food and drug administration |
| 25OHD | 25 Hydroxy vitamin D |
| WHO | World health organization |
| DEXA | Dual-energy Xray absorptiometry |
| FRAX | Fracture risk assessment tool |

