A Comparative study on Efficacy of Lutein and Atorvastatin on Lipid Profile and Lipoprotein(A) in Hypercholesterolemic male Wistar Rats.
 , ,
, , 1Department of Pharmacology, Shri Sathya Sai Medical College and Research Institute, Kancheepurum district, Tamil Nadu, India.
2Department of Anaesthesia, Shri Sathya Sai Medical College and Research Institute, Kancheepurum district, Tamil Nadu, India.
Corresponding Author E-mail : sowmimbbs13@gmail.com
DOI : http://dx.doi.org/10.13005/bpj/2151
Download this article as:
![]()
Background Hypercholesterolemia is the predominantfactor in developing atherosclerosis and myocardial diseases.A major contributor for the progression of atherosclerosis is abnormalities in lipid and lipoprotein metabolism.Hence the objectives of the study was to estimatethe comparative efficacy of Lutein with atorvastatin on lipid profile and lipoprotein(a) and to estimate the histopahthological changes in hypercholesterolemic male wistar rats.
Materials and Methods Experimental Wistar rats (male) were grouped into six. Each group contains 6 rats. Group I is control. Group II received cholesterol rich diet. Group III received cholesterol rich diet and the drug Atorvastatin 5mg/kg. Group IV received cholesterol rich diet and the drugLutein 25mg/kg. Group V received cholesterol rich diet and the drugLutein 50mg/kg. Group VI received cholesterol rich diet and the drug Lutein100mg/kg. At the end of 16 weeks, Blood samples from each rats was taken through retro-orbital puncture to evaluate serum lipoproteinsand lipoprotein(a) and thenwistar rats were sacrificed underinjection I.M Ketamine,Aortaand Liverwere dissected out and sent for histopathological studies.
Results The plasma LDL, VLDL, Triglycerides, total cholesterol, lipoprotein(a) levels were reduced in all lutein treated groups and atorvastatin treated group compared to high cholesterol diet group. A significant rise in HDL levels was noted in all Lutein treated groups and atorvastatin treated group. No statistically significant difference was seen between Atorvastatin 5mg/kg body weight and Lutein 100mg/kg body weight on reduction of total cholesterol.The efficacy of the drug Lutein in progression of atherosclerosis and its cytoprotective action in liver was proved in this study.
Conclusion This study indicates that Lutein has effect onreducing plasma lipoproteins&the study had shown significant antiatherogenic effect.
KEYWORDS:Atherosclerosis; Hypercholesterolemia; Lutein; Lp(a); Liver
Introduction
Myocardial disease is one of the leading cause of mortality in world-wide.The formation of atherosclerosis is due to endothelial dysfunction, deposition of lipid in the vessel wall which leads to inflammation of the vessel wall, cell proliferation & calcification. The risk factors such as abnormal cholesterol levels, hypertension, hyperglycemia & obesity further increases the incidence of stroke & myocardial disease.
Even though, several factors have been attributed to the causes of atherosclerosis. The main contributor for progression of this disease is abnormalities in lipoprotein metabolism. The importance of plasma lipoprotein and lipid metabolism abnormalities characterized by hyperlipidemia or hypercholesterolemia as the cause of coronary heart diseases (CHD).1
Hyperlipidemia is that the presence of excess fatty substances called lipids, mainly triglycerides and cholesterol, within the blood. Hyperlipidemia is otherwise called as hypolipoproteinemia because these fatty substances remain circulating within the blood attached to proteins.This can be the sole way that these fatty substances can remain dissolved while in circulation.2
Lipoproteins consists of macromolecular complexes that carries lipids molecules mainly cholesterol andtriglycerides via plasma &lymph. Lipoproteins plays a vital role in the transportation of cholesterol and triglycerides from liver to peripheral tissues and vice versa.3
The structure of Lipoprotein (a) ishighly complex, consists of a low density lipo protein (LDL) with the presence of apo B-100 bound to another protein, apolipoprotein (a)by disulphide bond. Many studies have proved that Lp(a)contributes to the formation atherosclerotic lesionsin arteries by inhibiting TGF (transforming growth factor) activation, and also by promoting vascular smooth muscle cellsproliferation. Lp (a) decreases the activity of fibrin-dependent plasminogen activator byinhibiting the binding of plasminogen to the endothelial cells. It acts as a pro-inflammatory mediator and augments the atherosclerotic lesion formation in plaques.
The high concentration of Lp(a) in association with raised LDL concentrations may potentiates the endothelial dysfunction. Specifically Lp(a), increases the permeability between endothelial cells, which facilitates deposition of LDL in arterial wall.4
Use of drug therapy depends on the level of cardiovascular risk. Patients with congestive heart disease or other risk factors and having average Low density lipoprotein cholesterol levels are benefited from treatment. Patients with congestive heart diseases should start a hypolipidemic drug therapy. According to NCEP ATP III guidelines, The hypolipidemic drug therapy is to reduce LDL level to <100mg/dlin patients with established congestive heart diseases, diabetes mellitus and to reduce LDL level to <70 mg/dl in congestive heart disease patients. Based on these guidelines, all Congestive heart disease patients and congestive heart diseases risk associated patients require lipid lowering drug therapy.3
Lutein is one of the hundreds of known naturally oxygenated carotenoids and has potential antioxidant properties. Some epidemiological studies found that serum HDL-C was positively associated, and oxidized LDL was negatively associated with serum Lutein levels.5 Hence the present study has been done to prove the comparative effects of Lutein with atorvastatin in rats fed with high cholesterol diet.
Materials and Methods
Chemicals and Reagents
Lutein was bought from MP Biomedicals, Mumbai, India. Pure Cholesterol &Cholic acid sodium salt were purchased from Himedia, India.
Preparation of Drug
Lutein 50mg/ml. Atorvastatin powder were dissolved in dimethyl sulfoxide (DMSO) and prepared the solution of 10mg/ml.
Animals
Adult Wistar rats (male) weighing 150-200 gms was used in this study. It was bought from Sastra University, Trichy, India. Wistar rats were kept in 6 different polypropylene cages, bedded with husk and maintained under proper environmental conditions at Animal House, RMMC&H.
Study Centre
Study was conducted in accordance with CPCSEA guidelinesat RMMC&H, Chidambaram. It was approved by the Animal Ethical Committee of RMMC&H, Chidambaram.
Experimental Induction of hypercholesterolemia
Hypercholesterolemia was induced in all groups except control group by feeding cholesterol diet. High cholesterol diet contains 1% of pure cholesterol, 0.5% of cholic acid sodium salt &1% of coconut oil was mixed inthe rat chow.6
Study design
Experimental wistar rats (male) were divided into 6 groups. Each group contains 6 rats (n=36).
Group I (n=6) = Control.
Group II (n=6) = High cholesterol diet.
Group III (n=6) = Atorvastatin 5mg/kg p.o daily with high cholesterol diet.
Group IV (n=6) = Lutein 25mg/kg p.o daily with high cholesterol diet.
Group V (n=6) = Lutein 50mg/kg p.o daily with high cholesterol diet.
Group VI (n=6) = Lutein 100mg/kg p.o daily with high cholesterol diet.7
The drug was administered through intra-gastric tube,every day in the morning for a period of 16 weeks.
Blood and Tissue sampling
After 16 weeks, Blood samples from each animal of all groups were collected via retro-orbital puncture in separate test tubesand named accordinglyto evaluate serum lipoproteinsand lipoprotein(a) and then wistar rats were sacrificed under injection I.M Ketamine,Aortaand Liver were dissected out and sent for histopathological studies
Biochemical Analysis
Blood samples from each wistar rats of all groups was collected in a different labelled test tubes& it was allowed to clot for 15-30 minutes. Test tubes were transferred to centrifuge and then the clot was taken out by centrifuging the test tubes for 10 minutes. The supernatant serum was obtained. Serum obtained was processed for the estimation of triglycerides, LDL, HDL, VLDL and total cholesterolusing calorimetry. The data obtained were analyzed by Duncan’s Multiple Range Test (DMRT), by SPSS software 16 version.
Results
Efficacy of Lutein in serum Lipid Profile & LP(a)
From Table 1, it was observed that significant statistical difference(p ≤ 0.05) seen in all Lutein treated groups& Atorvastatin group compared to high cholesterol diet group in the reduction of triglycerides,total cholesterol, VLDL, LDL & Lp(a) levels. A statistical significant raise in HDL levels in all Lutein treated groups. No statistically significant difference was seen between Atorvastatin 5mg/kg body weight and Lutein 100mg/kg body weight on reduction of total cholesterol, LDL, VLDL, HDL & LP(a). Table 1 shows efficacy of Lutein on serum lipid profile in hypercholesterolemic wistarrats.
Table 1: Efficacy of Lutein on Serum Lipid profile in Hypercholesterolemic Wistar Rats.
|
Groups |
Total cholesterol
mg/dl |
Triglycerides
mg/dl |
HDL
mg/dl |
LDL
mg/dl |
VLDL
mg/dl |
LP (a)
mg/dl |
| Group I | 72.93 ± 8.50a | 68.01±5.87a | 27.51 ± 0.29a | 18.08±1.89a | 11.63±1.74a | 6.83 ± 0.01a |
| Group II | 132.85±12.56 | 115.68±8.23b | 21.13 ± 0.28b | 48.08±8.94b | 29.40±4.80b | 12.64 ± 0.03b |
| Group III | 76.75 ±7.38c | 93.43±4.68c | 26.86 ±0.03c | 29.50±4.06c | 19.01±4.19c | 7.84 ± 0.03c |
| Group IV | 122.05±7.88d | 109.18±8.37d | 23.06 ± 0.15e | 45.98±4.64d | 23.46±4.22d | 11.63 ± 0.02e |
| Group V | 99.15±7.4e | 97.70±3.53e | 25.93 ± 0.13d | 37.68±3.96e | 21.75±2.23e | 8.73 ± 0.01d |
| Group VI | 78.86±9.92c | 89.08±4.59f | 26.71 ± 0.07c | 36.60±3.57e | 21.25±3.18e | 7.93 ± 0.01c |
Values are expressed as Means ± SD
Values not sharing a common superscript differ significantly at p ≤ 0.05. (DMRT).
Histopathological Evaluation
Detailed Histopathological examination of liver and aorta were carried out using light Trinocular microscope. The liver lesions such as micro and macro vesicular steatosis, degeneration and necrosis of hepatocytes, sinusoidal hemorrhages and infiltration of inflammatory cells and aorta lesions such as clumps of lipid droplets attached to tunica intima and irregular nuclei of smooth muscle fibers in tunica media were observed in high cholesterol fed (group II) animals. Similar lesions were also noted in group IV and V animals however the severity was lesser when compared with group II animals.
Microscopic examination of liver sections (Figure 1) of Group I animals showed normal radiating cords of hepatocytes with central round nucleus and homogenous cytoplasm around the central vein. Whereas the Group II animals showed severe steatosis (micro and macro vesicular) degeneration and necrosis of hepatocytes, infiltration of mono nuclear cells in the hepatic sinusoids. Group III animals showed the similar lesions but with less severity. Group IV and V animals showed moderate to mild steatosis (Micro and macro vesicular lipid droplets), chronic venous congestion, hepatocyte degeneration and mild inflammation. Group VI animals showed very less fatty change and normal hepatic architecture.
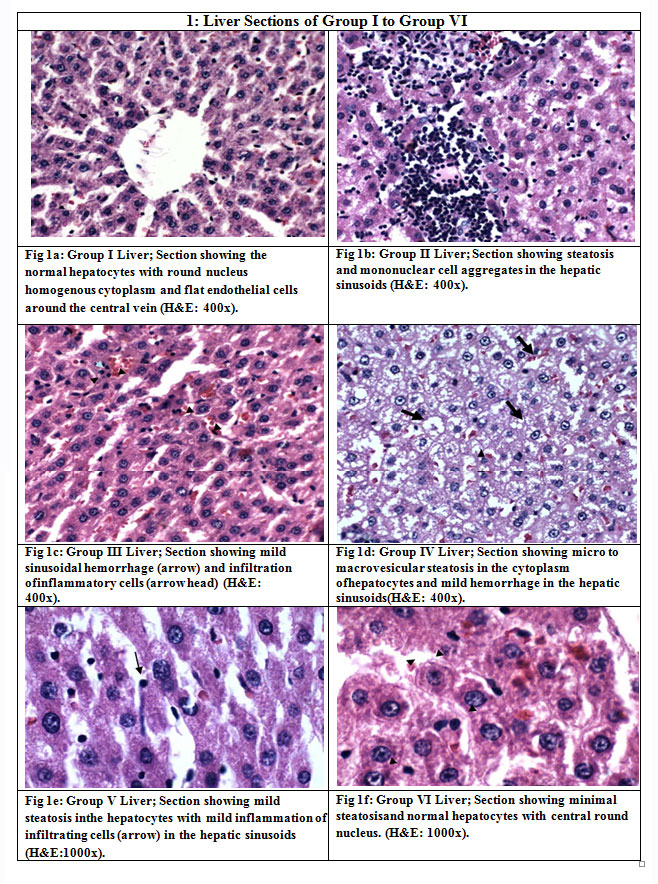 |
Figure 1: Liver Sections of Group I to Group VI. |
Microscopic examination of aorta sections (Figure 2) of Group I animals showed normal Tunica intima and Tunica media with normal smooth muscle fibres, wavy elastic fibers and loose Tunica adventitia. Group II animals showed clumps of lipid dropletsin the Tunica intima and irregular nuclei of smooth muscle fibers in Tunica media. In Group III animals, normal Tunica intima and mild thickening of Tunica media were observed. Irregular Tunica intima and sub endothelial lipid deposition in Tunica media were noticed in Group IV animals. Whereas Group V and VI animals showed normal Tunica intima and media with normal wavy elastic fibers.
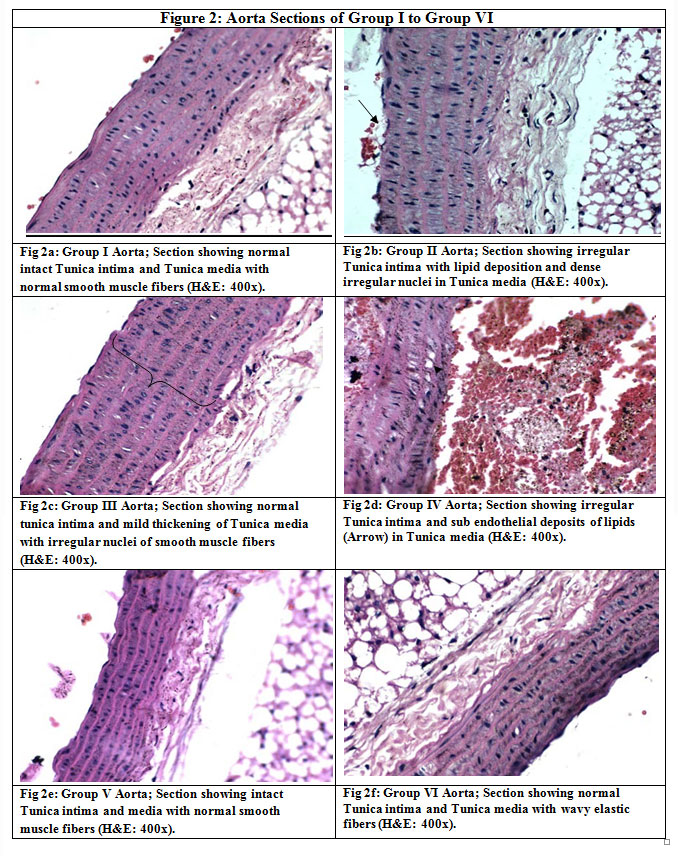 |
Figure 2: Aorta Sections of Group I to Group VI |
The findings showed that cellular damage in liver and aorta was raised in high cholesterol fed (group II) animals and the severity of lesions were more when compared with other group animals. Among the other groups’ animals, severity of lesion was lesser in group III, V and VI animals.
Discussion
Hyperlipidemia is that the main factor for diseases like myocardial infarction. The major causes of the disease in worldwide is increased cholesterol level leading to Ischemic cardiomyopathy and stroke.
Dyslipidemia and lowHDL levels also increases the risk of atherogenesis. Management of hyperlipidemia mainly focusses on reducing LDL levels. Incidence of coronary heart disease and strokes were found to be reduced by 30-40% when LDL-C level were reduced by drugs to 30-40% in clinical trials.8Although severe hypertriglyceridemia necessitates treatment to pancreatitis, it is unclear if hypertriglyceridemia ‘per se’ can lead to CAD.9 Insulin resistance can result in moderately elevated levels of TG with or without elevation of total cholesterol.
Lutein is one of the most widely available carotenoids and needs to be supplemented in diet as ‘de novo’ synthesis of lutein not possible in human being. Spinach, beef, lettuce, broccoli, eggs, orange & green leafy vegetables are rich sources of lutein.10 Although benefical effect of lutein in lung cancer has been reported11 inconclusive results for cancers of prostate12breast13 colon14 bladder15& stomach16 are reported. The preventive effect of lutein in ‘after cataract’ was reported by Yizhen HV et al in 2008.17
Lutein is a non-provitamin A carotenoids but a biologically active phytochemical.18 Being a flavonoid, it is devoid of side effects and hence is selected for our study. Oral route of administration is most convenient and improves patient compliance and hence in this preclinical study, oral dosage regimen was preferred.In animals fed on diet rich in cholesterol, LDL particles accumulate in subendothelial region of intima, undergo oxidation and in the presence of IL1, TNFα and angiotensin, trigger the expression of adhesion molecule ‘Foam cells’ an early atherosclerotic lesion occurs due to accumulation of modified lipoprotein.
Cholesterol rich diet is used to elevate serum cholesterol levels in animal models. Since cholesterol rich diet alone does not increase serum triglyceride levels, saturated fat is also needed along with cholesterol for a proper hyperlipidemic rat models. Diet containing both cholesterol & saturated fatty acid elevate the serum lipid levels by stimulating the activity of HMG CoA reductase along with down regulation of LDL receptors, increased activity of CETP & decreased level of LCAT enzyme. Cholic acid increases the cholesterol absorption. By suppressing cholesterol 7α hydroxylase activity, Cholic acid reduces the excretion of cholesterol.
The standard drug Atorvastatin used in our study resulted in reduced serum LDL, VLDL TC levels & HDLlevel wasincreased. Lutein also resulted in similar effects on lipid profile. However the effect of lutein on triglyceride levels at 100mg/kg dose (group VI) was found to be far more superior to the effect of atorvastatin.
The percentage inhibition of total cholesterol in atorvastatin group (group III) was 42% and that of lutein 100mg/kg dose (group VI) was 41% as compared to high cholesterol diet group (group II). Similarly the percentage inhibition of LDL & VLDL levels by atorvastatin was 39% & 34% respectively and that of lutein 100mg/kg was 25% in VLDL when compared with high cholesterol diet group (group II) The effect of atorvastatin and Lutein 100mg/kg in HDL levels were similar with a percentage elevation of 97%.
The rats received the standard drug Atorvastatin 5mg/kg (group III)and Lutein 100mg/kg (group 6) showed greater percentage inhibition of TC, LDL & VLDL compared to rats receiving high cholesterol diet. But the percentage inhibition of triglyceride levels of rats in lutein 100mg/kg is 21% when compared to cholesterol rich diet group (group II) and was found to be higher than the percentage inhibition of atorvastatin group (group III) which showed only 15% reduction of triglycerides. According to our study Lutein at 100mg/kg dose showed greater effect in reducing triglycerides than in reducing plasma lipoproteins when compared to Atorvastatin.
Statins act by competitively inhibiting HMG CoA reductase enzyme, and thus decreases the cholesterol synthesis. Hence their primary action is reducing of LDL-C although they cause reduction of VLDL & increase in HDL levels. Even though high doses of statins can reduce triglyceride levels, fibric acid derivatives are preferred in the therapy of hypertriglyceridemia.
Fibrates primarily lower TG levels by 20-50% while reducing LDL-C level by 10-15% and increasing HDL-C by 10-15%. Fibrates exert their action mainly through activation of peroxisome proliferator activated receptor α (PPARα). Probably lutein also acts through a similar mechanism.
Lp(a) prevents binding of plasminogen to cell thereby inhibiting generation of plasmin leading to clotting.19 Overexpression of LDL receptor gene increases the clearance of Lp(a)20and rabbits deficiency of LDL receptor gene show elevated Lp(a) levels.21 Cell culture studies show that Lp(a) has low affinity for LDL receptor.22 Statins increases LDL receptor expression but do not lower Lp(a).23
Asialoglycoprotein receptor (ASGPR) expressed in liver binds and internalises Lp(a) ASPGR knockout mice studies suggesting that this receptor constitute the major pathway for liver uptake of Lp(a).24Meta-analysis of 5436 CHD subjects from 27 prospective studies indicate that there was 70% more risk for CHD in patients with higher levels of Lp(a).25
According to the results of our study, Lutein at all three doses resulted in reduction of Lp(a) levels. Lutein 100mg/kg (group VI) showed the maximum response. Atorvastatin also reduced the Lp(a) level on par with lutein in our study. The Histopathology findings showed that cellular damage in liver and aorta was higher in High cholesterol diet group (group II) animals and the severity of lesions were more when compared with other group animals. Among the other groups’ animals, severity of lesion was lesser in Atorvastatin 5mg/kg group, Lutein 50mg/kg and Lutein 100mg/kg group animals.
In this study, Lutein reducedLDL, Total cholesterol, Lp(a), VLDL and triglycerideslevels, while increasing the level of HDL. Histopathological reports showed that lutein reduced the cellular damage in liver & aorta on par with the protective actions of atorvastatin.
Any drug that can reduce TG level in addition to its action on lipoproteins is a welcome addition to the list of current hypolipidemic drugs. The hypolipidemic potential of lutein can be exploited therapeutically to prevent atherosclerosis. Besides, being a flavonoid it is safe & devoid of side effects and its additional antioxidant property makes it more suitable for patients with high risk for CHD.
Conclusion
Flavonoids are found abundantly in nature. These are potent antioxidants. The carotenoid lutein was selected for this study not only because it is an antioxidant but also claimed to have hypolipidemic potential. In this preclinical study, the prophylactic effect of lutein in hyperlipidemia, was evaluated and compared with Atorvastatin. Lutein decreased the TC, LDL, VLDL, TG &Lp(a) levels and increased HDL levels. No side effects of lutein during the study period was noted. Our study reveals that lutein is an effective hypolipidemic agent that can reduce not only the lipoprotein level but also the triglyceride level and further extensive clinical studies are needed to prove this claim.
Acknowledgement
I thank my family members, Faculties of Department of Pharmacology, SSSMCRI, Professors of Department of Pharmacology R.M.M.C.H, Chidambaram and Micro Therapeutic Research Labs Private Limited, Chennai for providing laboratory assistance in analyzing the samples used in this study.
Conflict of Interest
There are no conflict of interest.
Funding Sourse
none
References
- Ali Al-Mamari. Atherosclerosis and Physical Activity Oman Med J. 2009 Jul;24(3):173–178.
CrossRef - Harikumar K, Ramesh P, Chandra Obul Reddy B, et al; Hypolipidemic activity of Ethanolic and Methanolic extracts of Echinochloa Crus-Galli in Triton Induced Hyperlipidemic Mice. International Journal of Biological & Pharmaceutical Research. 2013; 4(7):495-501.
- Rader DJ, Hobbs HH. Disorders of Lipoprotein Metabolism. In Harrisons Principles of Internal Medicine. Eds Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, 18th McGraw-Hill Book Co. New York, 2012; 356:3145-3161.
- Koschinsky ML, Marcovina SM; Lipoprotein (a). In Ballantyne Clinical Lipidology: A companion to Braunwald’s Heart Disease. Saunders Elsevier Inc. Pennsylvania, 2009; 11:130-140.
CrossRef - Mahley RW, Bersot TP. Drug therapy for hypercholesterolemia and dyslipidemia. Goodman & Gilman’s the pharmacological basis of therapeutics. 10th Ed. New York: McGraw Hill; 2001:971-1002.
- Asokan B.R, Jaikumar S, Nirmala P et al., Anti-hyperlipidemic activity of a poly herbal formulation in experimental models. 2010;433-442.
- Hao Han, Wei Cui, Danhong Gao, et al; Oxygenated carotenoid Lutein supplementation against early atherosclerosis in apo-deficient mice through alleviation the dyslipidemia and attenuation the oxidative stress. J Clin Pharmacol2000;35:345-51.
- Grundy SM, Vega GL, McGovern ME et al. Efficacy, safety and tolerability by once daily. Niacin for treatment of dyslipidemia associated with type 2 Diabetes; Results of the assessment of diabetes control and evaluation of the efficacy of Niaspan trial. Arch Intern Med, 2002,162:1568-1576.
CrossRef - Sarwar N, Danesh J, Eiriksdottir G et al. Triglycerides and the risk of coronary heart disease 10,158 incident cases among 262,525 participants in 29 western prospective studies. Circulation. 2007;115(4):450-458.
CrossRef - Heinonen M, Ollilainen V, Linkola E.K, et al. Carotenoids in finnish foods. Vegetables, fruits & berries. J.Agric. Food chem 1989; 37,655-659.
CrossRef - Michand DS, Feskanich D, Rimm EE et al. Intake of specific carotenoids and risk of lung cancer in 2 prospective US cohorts. Am J Clin Nutr 2000;72,990-997.
CrossRef - Giovannucci E, Ascherio A, Rimm EB et al. Intake of carotenoids and retinol in relation to risk of prostate cancer. J.Nath cancer inst 1995;1767-1776.
CrossRef - Dorgan JF, Sowell A, Swanson CA, et al. Relationships of serum carotenoids, retinol, alpha-tocopherol, and selenium with breast cancer risk: results from a prospective study in Columbia, Missouri. Cancer Causes Control. 1998;9(1):89-97.
CrossRef - Slattery ML, Benson J, Curtin K, et al. Carotenoids and colon cancer. Am.J.Clin.Nutri. 2000;71, 575-582.
CrossRef - Garcia R,Gonzalez CA, Agudo A, Riboli E. High intake of specific carotenoidsand flavonoids does not reduce the risk of bladder cancer. Nutr Cancer 1999; 35, 212-214.
CrossRef - Botterweck AAM, Van den Brandt PA &Goldbohm RA. Vitamins, carotenoids, dietary fiber and the risk of gastric carcinoma. Cancer 2000;737-748.
CrossRef - Yizhen HV &Zhirong XU. Effects of lutein on the growth & migration of bovine lens and epithelial cells In vitro; J Huazhong Univ.Sci.Technol (Med sci) 2008; 28(3) 360-363.
CrossRef - Fernando Granado, BegonaOlmedilla and Inmaculada Blanco; Nutritional and clinical relevance of lutein in human health. British Journal of Nutrition 200390;487–502.
CrossRef - Caplice NM, Panetta C, Peterson TE, et al. Lipoprotein (a) binds and inactivates tissue factor pathway inhibitor, a novel link between lipoproteins and thrombosis; Blood 98(10) 2980-2987.
CrossRef - Hofmann SL, Eaton DL, Brown MS, et al; Overexpression of human low density lipoprotein receptors leads to accelerated catabolism of Lp(a) lipoprotein in transgenic mice; J.Clin. Invest 1990; 85; 1542-1547.
CrossRef - Fan J, Challah M, Shimoyamada H, et al., Defects of the LDL receptor in WHHL transgenic rabbits lead to a marked accumulation of plasma lipoprotein[a].J Lipid Res.2000;41:1004-12.
CrossRef - Snyder ML, Polacek D, Scanu AM, et al., Comparative binding and degradation of lipoprotein(a) and low density lipoprotein by human monocyte-derived macrophages: Biol Chem 1992;267:339-346.
CrossRef - Kostner GM, Gavish D, Leopold B, et al.,HMG CoA reductase inhibitors lower LDL cholesterol without reducing Lp(a) levels;1989;80:1313-1319.
CrossRef - Hrzenjak A, Frank S, Wo X, et al.,Galactose-specific asialoglycoprotein receptor is involved in lipoprotein (a) catabolism; Biochem J:2003; 376:765-771.
CrossRef - Danesh J, Collins R, Peto R : Lipoprotein(a) and coronary heart disease. Meta-analysis of prospective studies: Circulation2000;102:1082-1085.
CrossRef




