
Manuscript accepted on :3-Dec-2020
Published online on: --
Plagiarism Check: Yes
Reviewed by: Christos Tsagkaris
Second Review by: Abhishek Raj
Final Approval by: Ayush Dogra
K. A. Arul Senghor* , Meera Shivasekar and V. M Vinodhini
, Meera Shivasekar and V. M Vinodhini
Department of Biochemistry SRM Medical College Hospital and Research Centre, SRM IST Kattankulathur 603203.
Corresponding Author E-mail: arulsenk@srmist.edu.in
DOI : https://dx.doi.org//10.13005/bpj/2071
Abstract
Introduction:Thyroid hormones and leptin is a perfect pair that maintains homeostasis of metabolic profile and abnormality in thyroid hormone levels potentiates insulin resistant state.The intriguing relationship between obesity and hypothyroidism is related by the key element leptin leading to consequent clinical implications. The severity of insulin resistance in hypothyroid and adipocytokine levels relate to the chance of pregnancy in infertile women. Aim:To assess the Leptin, insulin resistance and HOMA-adiponectin in Hypothyroid infertile women. Settings and Design:It is an Observational Cross-sectional work conducted in women with 20 to 40 years of age. About 180 infertile females were screened at the Obstetric& Gynecology OPD. 86 married women were categorized as groups: Euthyroid (A) –included fertile women who had TSH and FT4 within normal reference range. Subclinical Hypothyroidism (B) - infertile women with raised TSH ranging from 4.6 – 20 mIU/ml and normal FT4 Overt hypothyroid (C)- includedinfertile women with elevated TSH greater than 20 mIU/ml and decreased free T4 level. Methods and Material:Measurement of adiposity indices that includes calculated parameters such as BMI, WHR, waist circumference / height ratio and body roundness index. Fasting serum sample was collected and analysed for FT3, FT4, TSH, prolactin, insulin. Using Biovendor and DRG Human kit based on ELISA; Adiponectin and Leptin levels was estimated respectively. HOMA-IR and HOMA-adiponectin were calculated. Results:Mean Leptin concentrations and HOMA-adiponectin were significantly increased (p < 0.01) in Overt hypothyroid infertile women as compared to euthyroid and subclinical hypothyroid infertile women. Leptin had significantly positive correlation with TSH, FT3/FT4 ratio whereas negatively correlated with FT4. Significant positive correlation was observed with HOMA-IR and HOMA- adiponectin in hypothyroid infertile women. Conclusions:The study concludes that in hypothyroid infertile women having high leptin levels with reduced insulin sensitivity as related with increased HOMA-adiponectin. Analysis of thyroid profile, insulin sensitivity state along with leptin is mandatory to regulate ovulatory process in infertile women.
Keywords
FT3/FT4 Ratio; HOMA-adiponectin; Hypothyroidism; Leptin
Download this article as:| Copy the following to cite this article: Senghor K. A. A, Shivasekar M, Vinodhini V. M. Evaluation of Leptin and HOMA-Adiponectin in Hypothyroid Infertile Females. Biomed Pharmacol J 2020;13(4). |
| Copy the following to cite this URL: Senghor K. A. A, Shivasekar M, Vinodhini V. M. Evaluation of Leptin and HOMA-Adiponectin in Hypothyroid Infertile Females. Biomed Pharmacol J 2020;13(4). Available from: https://bit.ly/379tK7A |
Introduction
The estimate of overall prevalence of primary infertility in India is between 3.9 to 16.8% as per World Health Organization (WHO)1. According to the Indian Society of Assisted Reproduction, about 10 to 14 % of the Indian populations have infertility. Thyroid dysfunction is quite common in females and contributes to ovulatory dysfunction and aberrant function of Hypothalamic-pituitary-Ovarian axis. Hypothyroidism and hyperprolactinemia have profound effects on menstrual cycle, ovulatory process, fecundity and pregnancy 2, 3
The routine evaluation of thyroid profile in infertile women is mandatory since satisfactory levels of the circulating thyroid hormones are crucial for energy consumption, various metabolic pathways and continuation of normal reproductive function. Thyroid dysfunction has greater impact on the reproductive process affecting the fertility of the women. It is possible to identify the clinical condition of Hypothyroidism or Hyperthyroidism by early evaluation of thyroid profile in infertile women thereby can reverse the impact. It has been reported that individuals with excess of truncal adipose tissue are associated with abnormal thyroid hormone levels 4.There exists an intriguing link between thyroid hormones and obesity, which is supported by the explanation of decreased tissue responsiveness to thyroid hormones in obese individuals and also leptin is said to play a potential mechanism in this regard5.
Adipocytokines is said to have a putative role linking the balance of energy homeostasis and reproductive function. Leptin is a 28 KDaob gene product which regulates TRH gene expression and directs normal functioning of the thyroid axis Leptin is regulated by a wide range of inflammatory mediators such as TNF-α, IL-6 and IL-1β. Accumulation of excess adipose tissue mediates an inflammatory environment and leptin production is induced 6. Adiponectin is a 30 KDa protein encoded by ADIPOQ gene. Adiponectin is interrelated in energy metabolism as a molecule of insulin sensitizer, anti-atherogenic and anti-inflammatory properties. Reduced adiponectin concentration is very much implicated in insulin resistant state. Obesity is associated with decreased expression of AdipoR1 and AdipoR2 and impaired adiponectin signaling in adipose tissue is the possible mechanism responsible for reduced insulin sensitivity 7.
Thyroid hormones and leptin is perfect pair that maintains weight and energy expenditure. Moreover Leptin is an appetite regulator that controls metabolic efficiency and body weight regulation through its strong influence on HPA-T axis8. Abnormality in thyroid hormones levels affects the metabolic spectra which potentiates the alteration in metabolism contributing to the pathogenesis of insulin resistant state 9.
There exists obscure finding about the exact pathology between thyroid dysfunction and insulin resistance but adaptive response exhibits a key role 10. The conflicting data’s suggest that thyroid hormone levels are associated with energy expenditure and adiposity has its consequences ending to insulin resistance. Adipose tissue is considered as an endocrine organ that secretes biologically important molecules called Adipocytokines with multiple metabolic functions. The intricate interaction between thyroid hormones and adipocytokines has to be elucidated that potentiates the link to reproductive process.
Materials and Methods
Current work is an observational study conducted in theInfertility clinic, Department of Obstetrics and Gynecology. Hundred and thirteen female participants between the age group of 20 to 40 yrs were selected for the study after getting the approval from the Institutional Ethical Committee. The study was conducted after giving the full explanation of the study to the selected women who then signed the informed written consent.
The participants were selected as per the inclusion criteria with (i) history of atleast 1 year of infertility (ii) Male partner with normal semen analysis. The participants were examined by the gynecologist and diagnosed as primary infertility. Thyroid profile was done for all the participants and according to National Health and Nutrition examination survey III, were categorized into 3 groups:
Group A: (n = 30) Euthyroid – Fertile women with normal TSH levels (0.39 – 4.6 mIU/ml). Group B: (n = 36) Subclinical Hypothyroidism – Infertile women with TSH levels (4.6 – 20 mIU/ml) & normal FT4 levels. Group C: (n = 20) Overt Hypothyroidism – Infertile women with TSH levels (> 20 mIU/ml) and low FT4 levels.
According to WHO guidelines prolactin levels > 25 µg/ L is categorized as hyperprolactinemia. Infertile with anatomical defects, tubular blockage, endometriosis, genital TB, renal disease, liver disease or cardiac disease and hyperthyroid disorder were excluded from the study.
After overnight fasting with all aseptic precautions venous blood sample was drawn for evaluation of Free T3, Free T4, TSH, Prolactin using dedicated standard reagent kits in the instrument Vitros based on enhanced CLIA assay. Serum Leptin levels were assayed with DRG Human Leptin 96 well ELISA kit.. The expected normal serum leptin levels in lean women is 3.7 – 11.1 ng/ml. Biovendor Human Adiponectin 96 well ELISA kit was utilized to measure Adiponectin. Normal Adiponectin levels in females: BMI < 23: 8.2 – 19 μg/ml.
Calculated parameters
Calculation of Insulin Resistance = (Fasting Insulin μU/ ml x Fasting glucose mg/dL ) / 405
HOMA-IR = Fasting Insulin(μIU/ ml) multiplied with fasting glucose (mg/dl) divided by numerical 405. HOMA- Adiponectin11 = HOMA-IR divided by adiponectin. HOMA-Adiponectinis used for screening insulin resistance and cut-off value for reference is 0.95
Anthropometric measurements
Body mass index: Body weight was measured to the nearest kilogram using a standard weighing scale. Height was measured in meters.
WHR – Waist circumference and hip circumference were measured to the nearest 0.5 cm with a non-stretchable measuring tape.
WC – was measured in the midway section between the lower margin of the ribs and iliac crest.
HC – was measured at the cut-off levels of the greater trochanter.
WC/Ht ratio: is calculated as waist circumference in cm / height in cm.
Body roundness index12 was calculated as:
Body roundness Index serves as improved indicator of obesity that combines height and waist circumference and predicts the body fat percentage and visceral adiposity 13
Statistics
All the statistical data analysis was done with SPSS version 16.0 (SPSS inc). The values were documented as mean and standard deviation; and compared by ANOVA. p value of 0.05 was considered as statistically significant. Correlation analysis was performed to assess the correlation between variables.
Results
In the present study about 180 infertile women attending the infertility clinic were screened and 56 were found to have hypothyroidism. They were further categorized as subclinical hypothyroid and overt hypothyroid based on FT4 and TSH levels; and compared with 30 healthy fertile females.
The average duration of infertility was 3.76 years in subclinical hypothyroid and 5.27 years in overt hypothyroid infertile females. As presented in Table (1) anthropometric indicators were compared between subclinical hypothyroid, overt hypothyroid and fertile females. Statistical significant difference was observed with adiposity indicators such as WC, WC/Ht ratio and body roundness index in hypothyroid infertile females.
Table 1: Comparison of Anthropometric indicators between subclinical, overt hypothyroid infertile and euthyroid individuals.
| Parameters | Euthyroid (n = 30) | Subclinical hypothyroidism (n = 36) | Overt hypothyroidism (n = 20) | P value |
| Age | 30.52 ± 5.75 | 26.62 ± 3.83 | 29.15 ± 4.46 | 0.0109 |
| Weight (kg) | 58.94 ± 8.51 | 59.36 ± 7.79 | 66 ± 5.93 | 0.003 |
| Height (m) | 1.55 ± 0.036 | 1.54 ± 0.036 | 1.54 ± 0.03 | NS |
| BMI | 24.78 ± 3.63 | 24.73 ± 3.26 | 27.81 ± 2.642 | 0.002** |
| WC (cm) | 83.48 ± 3.79 | 86.15 ± 3.28 | 88.35 ±4.055 | 0.0001* |
| HC (cm) | 102.06 ± 6.47 | 102.46 ± 4.72 | 106.15 ± 5.38 | 0.02 |
| WHR | 0.838 ± 0.044 | 0.84 ± 0.03 | 0.83 ± 0.032 | 0.04 |
| Wc/Ht | 0.422 ± 0.178 | 0.556 ± 0.033 | 0.57 ± 0.035 | 0.0001*** |
| Body roundness Index | 3.274 ± 0.05 | 3.48 ± 0.048 | 4.91 ± 0.041 | 0.0001*** |
ValuesareexpressedinMean ± StandardDeviation. *Pvalue< 0.05isconsideredsignificant. NS-Notsignificant. ***VeryHighlysignificant**HighlySignificant.
Table (2) summarizes the comparison of thyroid hormones, prolactin, leptin and adiponectin between the groups. Among the infertile females 64.3% had subclinical hypothyroidism with TSH levels between 4.6 to 20 µIU/ml with normal FT4 levels; and 35.7% were overt hypothyroid with TSH levels > 20 µIU/ml and low FT4 levels. Likely prolactin levels were elevated in overt hypothyroid infertile females.
Table 2: Comparison of Biochemical parameters between subclinical, overt hypothyroid infertile and euthyroid individuals.
| Parameters | Euthyroid (n = 30) | Subclinical hypothyroidism (n = 36) | Overt hypothyroidism (n = 20) | P value |
| FT3 (pg/ml) | 3.12 ± 0.485 | 2.84 ± 0.78 | 1.719 ± 0.89 | 0.0001*** |
| FT4 (ng/dl) | 1.074 ± 0.15 | 1.102 ± 0.417 | 0.565 ± 0.295 | 0.0001*** |
| FT3/FT4 ratio | 2.80 ± 0.57 | 2.798 ± 0.97 | 5.025 ± 3.83 | 0.0001*** |
| TSH (µIU/ml) | 2.79 ± 0.904 | 8.857 ± 4.07 | 53.949 ± 34.67 | 0.0001*** |
| Prolactin (ng/dl) | 10.31 ± 2.68 | 22.759 ± 12.3 | 34.939 ± 23.07 | 0.0001*** |
| Leptin(ng/ml) | 19.15 ± 1.99 | 31.87 ± 15.984 | 42.54 ± 10.275 | 0.0001*** |
| Adiponectin (μg/ml) | 12.8 ± 2.77 | 7.6 ± 2.71 | 6.47 ± 1.88 | 0.0001*** |
| HOMA-IR | 1.89 ± 0.44 | 2.56 ± 0.9 | 2.81 ± 1.11 | 0.0004** |
| HOMA-adiponectin | 0.09 ± 0.03 | 0.44 ± 0.4 | 0.52 ± 0.38 | 0.0001*** |
ValuesareexpressedinMean ± StandardDeviation. *Pvalue< 0.05isconsideredsignificant. NS-Notsignificant. ***VeryHighlysignificant**HighlySignificant
The mean leptin levels were 42.54 ± 10.27 ng/ml and adiponectin levels were 6.47 ± 1.88 μg/ml in overt hypothyroid and statistical significant difference was observed in comparison with subclinical hypothyroid infertile and healthy fertile females respectively. As in Table (3) Pearson correlation analysis applied to these parameters, correlation of leptin revealed positive correlation with BMI, TSH and prolactin levels in subclinical and overt hypothyroid infertile females. As summarized in the table, leptin had negative correlation with FT4 and positive correlation with TSH and FT3/FT4 ratio. Further leptin revealed statistically significant correlation with HOMA-IR and HOMA-adiponectin as measure of insulin resistance (fig 1).
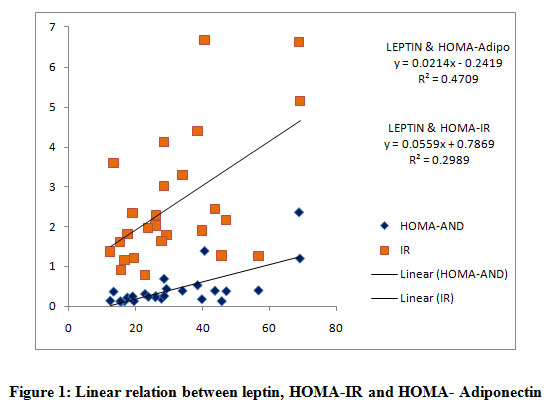 |
Figure 1: Linear relation between leptin, HOMA-IR and HOMA- Adiponectin |
Table 3: Correlation analysis of Leptin with Variables in infertile subclinical and overt hypothyroid women
| Parameters | Subclinical hypothyroidism (n = 36) | Overt hypothyroidism (n = 20) | ||
| LEPTIN | r value | P value | r value | P value |
| FT3 (pg/ml) | – 0.09 a | NS | – 0.23a | < 0.05 |
| FT4 (ng/dl) | – 0.11 a | 0.017 | – 0.31 b | 0.01 |
| FT3/FT4 ratio | + 0.42 | 0.005 | + 0.54 | 0.002 |
| TSH µIU/ml | + 0.45 b | 0.0078 | + 0.57 c | 0.002 |
| Prolactin (ng/dl) | + 0.34 b | 0.019 | + 0.46 b | 0.01 |
| HOMA-IR | + 0.54 c | 0.001 | + 0.76c | 0.0001 |
| HOMA-Adipo | + 0.68 c | 0.001 | + 0.67 c | 0.001 |
Correlation Small (0.1–0.3) Medium (0.3–0.5) Strong (0.5–1.0). a shows less correlation b Shows strongest correlation. c Indicates highly significant.
Discussion
Female infertility accounts to 37% of infertile couples and hypothyroidism is one of the most common thyroid diseases that cause abnormality of the regulatory processes in the female reproductive cycle. Adipocytokines serve as an important link that is involved in ovulatory menstrual cycle, embryo implantation and continuum of pregnancy. The fact that there exists vicious cycle around hypothalamus, leptin and adiposity that has its impact on the normal reproductive process 14. Leptin may be considered as a reliable marker to assess the severity of thyroid dysfunction and disturbed ovulatory process. Present study therefore is focused on the objective of evaluating the association between serum leptin levels with adiposity indicators and markers of insulin resistance in hypothyroid infertile females.
thyroid dysfunction and disturbed ovulatory process. Present study therefore is focused on the objective of evaluating the association between serum leptin levels with adiposity indicators and markers of insulin resistance in hypothyroid infertile females.
As suggested by other review authors, satisfactory level of leptinsignalling is required to maintain TRH expression in Hypothalamic – Paraventricular nucleus which is essential for normal TSH and Thyroid hormone production by Thyroid gland 17. Moreover TSH receptors are expressed in the adipose tissue indicating its role in the regulation of adipocytokines18. In our study positive correlation was observed between leptin and TSH which indicates the effect of TSH on leptin secretion by the adipose tissue. Our study uniquely evaluated the Leptin to FT3/FT4 ratio highlights the putative role of leptin in peripheral conversion of T4 to T3 by influencing the enzyme deiodinase19. Actually risk factors like obesity leads to leptin resistance which decreases the peripheral conversion of T4 to T3 but increases reverse T3 this in turn blocks further peripheral conversion to T3 and aggravates hypothyroid state 20.
Normally thyroid hormones are involved in glucose metabolism. Also expression and activation insulin and insulin like growth factor receptors in thyroid cells are promoted by TSH 20. Present study revealed the positive correlation of leptin with insulin resistance indices in hypothyroid females that emphasizes the synergistic effect over impaired ovulatory function. This is supported by the study in PCOS women in which there exists association between TSH concentration and insulin resistance 21.
As per the correlational analysis, we observed significant correlation of leptin with HOMA- adiponectin, which is one of the insulin resistance indices that take account of the beneficial adipocytokineadiponectin. Obesity is associated with reduced expression of adiponectin receptors that leads to impaired adiponectinsignalling in the adipose tissue which is implicated to reduced insulin sensitivity 22. This study forms the platform for the researchers to study the adipocytokine profile before and after life style modification; thereby assess the occurrence of ovulation. Also the Clinicians are directed the right pathway to advice life style modifications primarily and followed by therapeutic implications.
This study concludes that individuals with excess adipose tissue have elevated leptin levels contributing to leptin resistance. This in turn influences and aggravates insulin resistant state as noted by HOMA-IR and HOMA-adiponectin and further leads to disturbed ovulatory process affecting the normal reproductive physiology.
Conclusion
High Leptin level is evident in hypothyroid infertile women. Leptin relates with insulin resistant state and increased HOMA-adiponectin in hypothyroid women elucidates the importance of adiponectin in reproductive process. Thyroid profile work out is mandatory for all infertile women and subsequent treatment withlife style modification to be inculcated in women thereby insulin sensitivity is promoted and the chance of conception and normal reproductive process is maintained.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- National Health Portal. India. Gateway of authentic Health information. nhp.gov.in/disease/reproductive-system/infertility published date. Aug 5 (2016).
- MohanaPriya, NishatAkhtar, and Jamal Ahmad. Prevalence of hypothyroidism in infertile women and evaluation of response of treatment for hypothyroidism on infertility. Indian Journal of Endocrinology and Metabolism. Jul-Aug; 19(4): 504–506 (2015). doi: 10.4103/2230-8210.159058.
CrossRef - Keerthanaa SR et al. Analytical study of thyroid and prolactin hormone levels in infertile women with menstrual irregularities. Int J ReprodContraceptObstet Gynecol. Apr;9 (4): 1 – 7 (2020).
CrossRef - Knudsen, P. Laurberg, L. B. Rasmussen et al. Small differences in thyroid function may be important for BMI and the occurrence of obesity in the population. Journal of Clinical Endocrinology and Metabolism. 90(7): 4019 – 4024 (2005).
CrossRef - Sanyal D, Raychaudhuri M. Hypothyroidism and obesity: An intriguing link. Indian J EndocrinolMetab. 2016;20(4):554-557. doi:10.4103/2230-8210.183454.
CrossRef - Al-HindawiSahar H. The Influence of Thyroid Hormones on Leptin and Resistin Levels in Hyperthyroid Female Patients. International Journal of Medical Research & Health Sciences, 7(1): 40-47 (2018).
- Toulis K.A., Goulis D.G., Farmakiotis D., Georgopoulos N.A., Katsikis I., Tarlatzis B.C., Papadimas I., Panidis D. Adiponectin levels in women with polycystic ovary syndrome: A systematic review and a meta-analysis. Reprod. Update. 15:297–307(2009).doi: 10.1093/humupd/dmp006.
CrossRef - Nakamura A, Miyoshi H, Ukawa S, Nakamura K, Nakagawa T, Terauchi Y, et al. Serum adiponectin and insulin secretion: a direct or inverse association? J Diabetes Investig.9(5):1106-9 (2018).
CrossRef - Roef, B. Lapauw, S. Goemaere et al., “Body composition and metabolic parameters are associated with variation in thyroid hormone levels among euthyroid young men. European Journal of Endocrinology. vol 167(5): 719–726 (2012).
CrossRef - Kaushikkar, Satwikasinha. Variations of Adipokines and Insulin Resistance in Primary Hypothyroidism. Journal of Clinical and Diagnostic Research. Aug, Vol-11(8): BC07-BC09 (2017).
- BrunnaSullaraVilela, Ana Carolina JunqueiraVasques, Roberta Soares, Lara Cassani, Adriana Costae Forti, José Carlos Pareja, Marcos Antonio Tambascia, BRAMS Investigators, Bruno Geloneze.The HOMA-Adiponectin (HOMA-AD) closely Mirrors the HOMA-IR Index in the screening of Insulin Resistance in the Brazilian Metabolic Syndrome Study (BRAMS). PLoS One. 11(8): e0158751 (2016).
CrossRef - Nikhil Mathur, SrinidhiRai, NevedithaSujith, OrruGayatri. Newer v/s Classical Anthropometric Indices as a Screening Tool for Dyslipidemia in Healthy Young Adults. Journal of Clinical and Diagnostic Research. Apr, Vol-13(4): BC04-BC07 (2019).
CrossRef - Thomas DM, Bredlau C, Bosy-Westphal A, Mueller M, Shen W, Gallagher D, et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity (Silver Spring). 21:2264- 71(2013).
CrossRef - Olga Gruzdeva, DariaBorodkina, EvgenyaUchasova, YuliaDylevaand Olga Barbarash. Leptin resistance: underlying mechanisms and diagnosis. Diabetes MetabSyndrObes 12: 191–198 (2019). doi: 2147/DMSO.S182406.
CrossRef - Farr OM, Gavrieli A, Mantzoros CS. Leptin applications in 2015: what have we learned about leptin and obesity? CurrOpinEndocrinol Diabetes Obes. Oct; 22(5):353-9 (2015).
CrossRef - Ahmed Alahmar, SulagnaDutta, PallavSengupta. Thyroid hormones in male reproduction and infertility Asian Pacific Journal of Reproduction.8(5): 203-210 (2019)
CrossRef - Jeffrey S. Flier, Mark Harris, and Anthony N. Hollenberg. Leptin, nutrition, and the thyroid: the why, the wherefore, and the wiring. J Clin Invest. Apr 1; 105(7): 859–861(2000). doi: 1172/JCI9725.
CrossRef - BernaEmgeAydogan and Mustafa Sahin. Adipocytokines in Thyroid Dysfunction. Hindawi Publishing Corporation ISRN Inflammation Volume Article ID 646271, 1 – 7 2013)http://dx.doi.org/10.1155/2013/646271.
CrossRef - Cettour-Rose P, Burger AG, Meier CA, Visser TJ, et al. Central stimulatory effect of leptin on T3 production is mediated by brown adipose tissue type II deiodinase. Am J PhysiolEndocrinolMetab. 283(5):E980–7 (2002).
CrossRef - Holtorf, Kent. Peripheral Thyroid Hormone Conversion and Its Impact on TSH and Metabolic Activity. Journal of Restorative Medicine, Volume 3, Number 1, April, pp. 30-52 (2014).
CrossRef - RashmiMullur, Yan-Yun Liu, and Gregory A. Brent. Thyroid Hormone Regulation of Metabolism. Physiology Reviews. Apr; 94(2): 355–382 (2014). doi: 1152/physrev.00030.2013.
CrossRef - Kaushikkar, Satwikasinha. Variations of Adipokines and Insulin Resistance in Primary Hypothyroidism. Journal of Clinical and Diagnostic Research. 2017 Aug, Vol-11(8): BC07-BC09(2017).

