
Manuscript accepted on :28-04-2020
Published online on: 22-05-2020
Plagiarism Check: Yes
Reviewed by: Flora Balieva
Second Review by: Georgekutty Kochuchakkalackal
Final Approval by: Prof. em. Hans-Joachim Freisleben
Elham Alshammari1*, Ahlam Alshammari2, Fatima Alsubaie1, Yasmeen Alanazi1, Lujain Alshawi1, Reema Bakhamis1, Nawal Alashgar1 and Waleed Alsowayan3
1Department of Pharmacy Practice, College of Pharmacy, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
2Medical Service Authority, Military Medical Complex, Kuwait.
3Internal Medicine Department, Security Force Hospital Program, Riyadh, Saudi Arabia.
Corresponding Author E-mail : ejalshammari@pnu.edu.sa
DOI : https://dx.doi.org/10.13005/bpj/1952
Abstract
In the Kingdom of Saudi Arabia, there are many patients who suffer from uncontrolled asthma. However, very few studies have been conducted to explore this issue. In this regard, the primary aim of the current study is to examine the level of asthma control among patients in a Saudi hospital. The authors used the GINA 2019 classification to classify the patients into three categories – controlled, partly controlled, or uncontrolled asthma. The secondary goal of the study was to examine the relationship between the level of control and the number of times that a patient visited the emergency department because of an asthma attack. Data was collected from asthmatic patients who attended a pulmonary clinic between October and December 2019. The results showed that close to 75% of the patients had controlled or partially controlled chronic asthma symptoms. Only 25% of the patients had uncontrolled symptoms of asthma. The results of the chi-square test were as follows (age = 0.509, p > 0.05, gender = 0.143, p > 0.05, education level = 2.07, p > 0.05 and level of physical activity = 8.55, p > 0.05). These findings mean that age, gender, education level, and the level of physical activity did not have any significant impact on the adherence to the treatment plan. An examination of the relationship between the treatment plan and emergency department visits resulted in: (r=0.317, p>0.05). These results meant that there was an equal number of emergency department visits for those who adhered and those who did not adhere to the treatment plan.
Keywords
Asthma; Disease Control; Evaluation Study; Hospital Care; Saudi Arabia
Download this article as:| Copy the following to cite this article: Alshammari E, Alshammari A, Alsubaie F, Alanazi Y, Alshawi L, Bakhamis R, Alashgar N, Alsowayan W. Evaluative Study of Asthma Control in a Saudi Hospital. Biomed Pharmacol J 2020;13(2). |
| Copy the following to cite this URL: Alshammari E, Alshammari A, Alsubaie F, Alanazi Y, Alshawi L, Bakhamis R, Alashgar N, Alsowayan W. Evaluative Study of Asthma Control in a Saudi Hospital. Biomed Pharmacol J 2020;13(2). Available from: https://bit.ly/3cTFmfi |
Introduction
Asthma Worldwide and Saudi Arabia Statistics
Asthma is a widespread condition affecting many people worldwide. Estimates show that asthma affects close to 5-10% of the population, translating to about 23.4 million individuals.1 Exercise-induced bronchospasm has a general rate of prevalence of 3-10% if individuals without asthma or a related allergy are excluded.1 However, the percentage increases to between 12 and 15 after the inclusion of patients with an underlying asthma condition.1 With all these conditions in mind, the World Health organization estimates that close to 235 million people are living with asthma worldwide. Besides, WHO also notes that over 80% of asthma-related deaths happen in countries with a low and lower-middle income.2 This is the case in Saudi Arabia, where asthma is a common condition. A report titled “Saudi Arabia’s adult prevalence of asthma” shows an 18.2% frequency of wheezing for patients who did not have a virus.3 The rate at which individuals take asthma medications in the country is 10.6%.3
Treatment Guidelines of Asthma
The management of asthma entails the treatment of acute episodes of the condition, as well as control of chronic symptoms.4 In other cases, treatment may also deal with night-time and symptoms induced because of exercise.4 GINA and SINA guidelines provided by an expert panel advocate that asthma treatment be based on distinct phases – initiation, adjustment, and maintenance of treatment.5 Figure 1 below illustrates the treatment steps that may be involved when following the GINA guidelines.
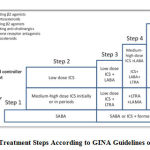 |
Figure 1: Treatment Steps According to GINA Guidelines on Asthma |
Uncontrolled Asthma Risk and Related Statistics
Asthma control illustrates the level of reducing the incidence and intensity of symptoms and functional limitations. As such, uncontrolled asthma is often marked by increased visits to the emergency department among other symptoms.6 The Centers for Disease Control and Prevention estimates that an average of 38.4% of children and 50.0% of adults with asthma experienced uncontrolled asthma between 2006 and 2010 worldwide.7 In the Kingdom of Saudi Arabia, there is a high percentage of patients who experienced cases of uncontrolled asthma. 64% of adults and 59.3% of children are believed to experience uncontrolled asthma.8
Uncontrolled asthma symptoms can be a critical risk factor for exacerbations. However, there are other risk factors that can contribute to exacerbations, even among patients that have very few symptoms of asthma. For instance, poor adherence to medications or the use of a wrong inhaler technique may lead to exacerbations. Comorbidities, such as obesity, gastro-esophageal reflux disease, chronic rhinosinusitis, anxiety, food allergies, and pregnancy may also serve as important risk factors. Additionally, individuals may experience exacerbations when exposed to smoking, air pollution, and allergens among other conditions. 9
There are numerous factors that affect the regulation of asthma. These factors may range from socio-demographic characteristics to psychosocial factors, observance to medication, severity of the condition, use of suitable inhalation technique, high use of SABA, exposure to agents that are infectious, and exposure to allergens or pollutants. Comorbidities, such as chronic sinusitis and hypertension can intensify the risk of asthma and lead to poor control mechanisms. Moreover, the use of some medications can cause the onset of asthma. Medications to avoid in this cause may include aspirin, non-steroid anti-inflammatory medications, and beta-blockers, among others. Even though asthma cannot be cured, the condition can be controlled effectively in many patients by evading the triggers and adhering to the recommended treatment plan. 9
Cost of Asthma Therapy and Uncontrolled or Untreated Asthma
Disease control and financial burden have been studied and measured in many different settings expressing the role of clinical pharmacy services. 10,11 Epidemiological statistics show an unquestionable increase in asthma, both locally and across the world. That means that the financial weight of the disease is also on the increase. The cost of the disease often results from the other diseases that may accompany the condition, such as hypersensitivity and obstructive rest apnea. Asthma may also cause extraordinary bleakness, an increase in visits to the emergency division, and a decline in productivity due to missed working days.12 The performance of students may also be affected due to missed school days. In the United States, the condition places a huge economic burden on the nation with the total estimated cost being $81.9 billion as of 2013. This figure includes the costs incurred due to absenteeism and mortality. Such an inflated cost can be reduced by ensuring improved access to human services, providing better education on asthma, and reducing the ethnic and racial gaps in the treatment of asthma. 13
Previous Studies
A past study examined repeated visits and admission in central Saudi. The purpose of the study was to discover the pediatric age group, the gender that was mostly affected by asthma, and some of the factors that predicted severity of this condition. The authors noted that most patients (71.9%) were male. Most of the patients (58.9%) were between 1 and 6 years.14 Most of the patients visited the emergency department due to asthma occurring more than once across half of the study period. Over two-thirds of the parents were able to explain the method of administering the meter dose inhaler properly. Additionally, infants were less affected by asthma, while those who were on medication had an exceedingly high incidence rate.13 From these findings, it is possible to assume that the right administration of medication can serve as an indicator of asthma severity.
Another study used EHR data to predict regular visits to the emergency department among asthmatic children.14 The study was motivated by the fact that ED visits are common and avoidable among children with asthma. From the data of 2691 children, the authors noted that demographics, the state of insurance, co-morbidities, use of healthcare resources, and the history of medication influenced the regular use of the emergency department. The final model developed by the authors found two primary variables – the status of insurance and the previous use of the emergency department. The odds of using the ED often were 3.1 times for patients who were publicly insured, compared to those who were privately insured. Patients with public insurance who had over four ED visits and those who were privately insured and with more than six visits to the ED had at least or more than 50% chance of visiting the ED the next year.15 These findings suggest that earlier visits to the ED and the status of insurance were strong predictors of future use of the ED among asthmatic children.
Earlier research also examined the usefulness of an action plan in enhance the outcome of asthma among children.16 The study was motivated by the fact that many asthma guidelines recommend the use of the written asthma action plan (WAAP) to improve the outcome of the disease. In the study, asthmatic children received WAAP and were followed up for a period of six months, where the outcome variables were measured. The primary outcome variables were asthma exacerbation that needed a visit to the emergency room, admission, impromptu OPD visit, and absence in school. The results of the study showed a reduction in the visits to the emergency room, impromptu OPD visits, number of admission days, and days absent in school.16 The findings of the study seem to suggest that the use of a well-designed WAAP can enhance self-care among patients and minimize asthma exacerbation.
Additionally, the implementation of asthma management guidelines has also been examined in the context of the emergency department.17 The authors compared the known strategies for managing severe bronchial asthma at the Emergency Room with the guidelines used in Saudi Arabia. The study entailed a retrospective examination of over 150 ER records, covering a diagnosis of asthma over a 1-year period between January and December 2000. Based on the findings of the study, less than 50% of the patients reported a history of asthma attack, its duration, frequency, and night-time symptoms. Also, less than 50% of the patients reported past visits to the ER and hospitalization, use of accessory muscle, and the peak flow rate. Only 46% of the patients who visited ED were given steroids, while only 64% of the patients were offered an opportunity for follow up appointment.17 From the study findings, it is possible to argue that unsatisfactory care of asthmatic patients often emanates from the failure to implement the recommended asthma guidelines.
Materials and Methods
Research Objectives
The primary objective of the study is to examine the degree of asthma control in patients in a Saudi hospital based on the GINA 2019 classification.
The secondary objective of the study is to investigate the relationship between the level of control and the number of visits to the emergency room due to asthma attacks.
Methodology
The authors carried out a prospective observation study implemented for 6 weeks. In essence, the study was conducted between October and December 2019 for five days each week. Data was obtained from patients visiting the pulmonary clinic. The patients were screened and followed-up for diagnosis. The following inclusion criteria was used. The patients were 18 years and above, had a documented diagnosis of bronchial asthma, and had visited the clinic between October and December 2019.
Results and Discussion
Demographic Characteristics of the Sample
62 patients met the inclusion criteria for the period between October and December 2019. Out of the 62 participants the majority 72.6% (n = 45) were females and 27.4% (n = 17) was males. The participants age ranged from 18 to 79 and the mean age was 51.15 (SD = 14.09). Table.1 below shows the education levels of the participants.
Table 1: Education Level
| Frequency | Percent | |
| Illiterate | 14 | 22.6 |
| Primary Education | 11 | 17.7 |
| Middle Education | 14 | 22.6 |
| Secondary Education | 19 | 30.6 |
| Tertiary Education | 4 | 6.5 |
| Total | 62 | 100.0 |
Descriptive Statistics
Asthma classification
According to the Asthma classification, 75% of the patients belonged to moderate persistent or to mild intermittent categories. However, 25% of the patients belonged to the severe persistent category. These findings are illustrated in Figure.2.
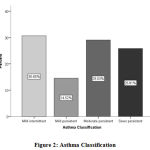 |
Figure 2: Asthma Classification |
Asthma Exacerbation Severity
64.52% (n = 40) of the patients had mild to moderate exacerbation. On the contrary, 35.48% (n = 22) had severe exacerbation to respiratory failure. The Fig.3 illustrates these findings.
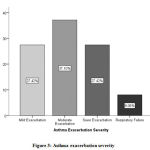 |
Figure 3: Asthma exacerbation severity |
Chronic Asthma Symptoms Control
Three-quarters of the patients had controlled or partially controlled chronic asthma symptoms. In the same manner, only one-quarter of the patients had uncontrolled asthma symptoms. These findings are illustrated in Fig. 4.
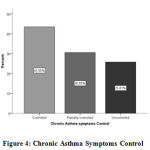 |
Figure 4: Chronic Asthma Symptoms Control |
Treatment Plan and the Adherence to Treatment Plan
All the patients (n = 62) had some sort of a treatment plan. However, only 85.5% (n = 53) followed the treatment plan. Nine patients (14.5%) did not follow the treatment plan.
Impact of Demographic Factors on Adherence to the Treatment Plan
The authors carried out a chi-square test to examine the relationship between demographic factors on adherence to treatment plan. Since, the age variable was scale in nature it was converted into a categorical variable with three levels (18 – 37, 38 – 57, 58 and above). According to the chi-square test results, age, = 0.509, p > .05, gender, = 0.143, p > 0.05, education level, = 2.07, p > 0.05 or level of physical activity, = 8.55, p > 0.05 had no significant impact on the adherence to the treatment plan. Which means irrespective of the gender, age, education level or level of physical activity, patients are quite similar in terms of the way they follow the treatment plan. The results of the chi-square test are as shown in Table 2.
Table 2: Chi-square Test Results
| Variable | Chi-Square value () | P value/Sig. |
| Age | 0.509 | 0.775 |
| Gender | 0.143 | 0.705 |
| Education Level | 2.07 | 0.724 |
| Level of Physical Activity | 8.55 | 0.056 |
Table 3: Chi-square Test Results
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | 0.317 | 1 | 0.573 | ||
| Continuity Correction | 0.008 | 1 | 0.927 | ||
| Likelihood Ratio | 0.350 | 1 | 0.554 | ||
| Fisher’s Exact Test | 1.000 | 0.495 | |||
| Linear-by-Linear Association | 0.312 | 1 | 0.576 | ||
| N of Valid Cases | 62 |
Table 4: Cross Tabulation (Adherence to Treatment Plan and ED Visits).
|
Variable |
ED visit | Total | ||
| No | Yes | |||
| Adherence to treatment plan | No | 8 | 1 | 9 |
| Yes | 43 | 10 | 53 | |
| Total | 51 | 11 | 62 | |
Drugs used for Treatment
Salbutamol was the most used drug. Drugs such as fluticasone / salbutamol, Budesonide / formoterol and montelukast sodium were also used highly to treat asthma. Ipratropium and budesonide were the least used drugs. A summary of these findings is shown in Table 5.
Table 5: Drugs
| Drug | Used or not | Frequency |
| Fluticasone / Salbutamol | No | 36 |
| Yes | 26 | |
| Budesonide / Formoterol | No | 33 |
| Yes | 29 | |
| Budesonide | No | 59 |
| Yes | 3 | |
| Montelukast sodium | No | 38 |
| Yes | 24 | |
| Salbutamol | No | 23 |
| Yes | 39 | |
| Ipratropium | No | 60 |
| Yes | 2 |
Monthly Cost for Treatment
Considering the monthly costs for treatments and available cost information from 55 patients, it ranged from 16 to 635 Saudi Riyals (1 United States Dollar equals 3.75 Saudi Riyal). The mean monthly cost was 303.16 SR (SD = 117.66). These findings are further demonstrated in the Fig. 5.
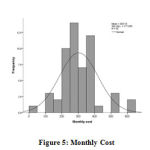 |
Figure 5: Monthly Cost |
Conclusion
The purpose of the study was to analyze the degree of asthma control among patients in a Saudi hospital. The findings showed that most of the patients had either controlled or partially controlled chronic asthma symptoms. The other aim of the study was to examine the relationship between the level of control and the number of visits to the emergency room due to asthma attacks. There was an equal number of emergency department visits for those who adhered and those who did not adhere to the treatment plan. While adherence to a treatment plan is significant in the control of asthma, this study concludes that this does not necessary dictate visits to the emergency room.
Ethics Approval
All researchers have read the law of ethics and granted the National Committee of bioethics certificate.
Research number in security forces hospital program: 19-369-67.
Institutional review board IRB registration number with KACST, KSA: H-01-R-069.
Acknowledgment
This research was funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program.
References
- Morris MJ, Pearson DJ. What is the worldwide prevalence of asthma? Medscape 2019; https://www.medscape.com/answers/296301-7945/what-is-the-worldwide-prevalence-of-asthma.
- Asthma. World Health Organization 2019; https://www.who.int/news-room/q-a-detail/asthma.
- Al Ghobain MO, Algazlan SS, Oreibi TM. Asthma prevalence among adults in Saudi Arabia. Saudi Medical Journal 2018; 39(2):179-184.
- Al-Moamary MS, Alhaider SA, Alangari AA, Al Ghobain MO, Zeitouni MO, Idrees MM, Alanazi AF, Al-Harbi AS, Yousef AA, Alorainy HS, Al-Hajjaj MS. The Saudi initiative for asthma – 2019 update: Guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med 2019; 14(1): 3-48.
- Global strategy for asthma management and prevention. Global Initiative for Asthma 2019; https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf.
- Uncontrolled asthma among persons with current asthma. Centers for Disease Control and Prevention 2014; https://www.cdc.gov/asthma/asthma_stats/uncontrolled_asthma.htm
- Al-Jahdali H, Ahmed A, Al-Harbi A, Khan M, Baharoon S, Bon Salih S, Halwani R, Al-Muhsen S. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin Immunol 2013; 9(1):8.
- BinSaeed A. Asthma control among adults in Saudi Arabia. Saudi Medical Journal 2015; 36(5): 599-604.
- Al-Jahdali H, Anwar A, Al-Harbi A, Baharoon S, Halwani R, Al Shimemeri A, Al-Muhsen S. Factors associated with patient visits to the emergency department for asthma therapy. BMC Pulmonary Medicine 2012; 12(80): 1-7.
- Alshammari, E., Role of clinical pharmacist in dose adjustment of renally eliminated drugs in cardiac patients with renal impairment. Int. Res. J. Pharm., 2019; 10(2): 70-74.
- Alshammari, E., Irrational Prescribing Habit of Omeprazole. International Journal of Pharmaceutical Quality Assurance, 2019; 10(3): 578-582.
- Loftus PA, Wise SK. Epidemiology and economic burden of asthma. Int Forum Allergy Rhinol 2015; Suppl 1: S7-10.
- Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008-2013. Ann Am Thorac Soc 2018; 15(3): 348-356.
- Al-Yami SM, Mohajer KA, Al-Jeraisy MI, Batarfi AM, Abolfotouh MA. Recurrent visits and admissions of children with asthma in central Saudi Arabia. Saudi Med J 2010; 31(8): 921-4.
- Das LT, Abramson EL, Stone AE, Kondrich JE, Kern LM, Grinspan ZM. Predicting frequent emergency department visits among children with asthma using HER data. Pediatr Pulmonol 2017; 52(7): 880-890.
- Lakupoch K, Manuyakorn W, Preutthipan A, Kamalaporn H. The effectiveness of newly developed written asthma action plan in improvement of asthma outcome in children. Asian Pac J Allergy Immunol 2018; 36(2): 88-92.
- Al-Jahdali HH, Al-Omar AM, Al-Moamary MS, Al-Duhaim AS, Al-Hodeib AS, Hassan IS, Al-Rabegi AM. Implementation of the national asthma management guidelines in the emergency department. Saudi Med J 2004; 25(9): 1208-11.

