
Manuscript accepted on :27-06-2020
Published online on: 30-06-2020
Plagiarism Check: Yes
Reviewed by: Ankur Singh Bist
Second Review by: Ismail Ismail Abdullahi
Final Approval by: Dr. H Fai Poon
Shan Babu , Priya Susanand Pendem Saikiran*
, Priya Susanand Pendem Saikiran*
Department of Medical Imaging Technology, Manipal College of Health Professions, Manipal Academy of Higher Education, Manipal, Karnataka, India
Corresponding Author E-mail : saikiran.p@manipal.edu
DOI : https://dx.doi.org/10.13005/bpj/1971
Abstract
Chronic otitis media [COM] is a long-term infection of middle ear and mastoid cavity with frequent ear discharges through a tympanic perforation. Eustachian tube measurements done using High Resolution Computed Tomography [HRCT] would be helpful in determining the influence of it in the development of COM and cholesteatoma. The aim of study is to compare the ET measurements in patients having COM without Cholesteatoma, COM with Cholesteatoma and normal ears. This is a retrospective study. A total of 79 patients (47 males, 32 females, age range: 15-81 years) referred for temporal bone from June 2016 to June 2018 were included. Of 79 patients, Group A included 54 ears who had COM without cholesteatoma (26 Unilateral, 14 Bilateral) and Group B included 49 ears who had COM with cholesteatoma (29 unilateral and 10 Bilateral). Patients who underwent HRCT PNS with no pathologies related to middle ear were included as controls. Group C included 158 ears (79 patients) with normal ears. The ET angle with respect to Reid’s plane (ETA), Tubotympanic angle (TTA), Pretympanic diameter (PTD) was measured between the three groups. The mean ETA , TTA, PTD measured for groups A, and B was 24.30±1.6°, 146±3.2°, 5.5±2.2 mm, & 21.18±1.4°,148±4.2°, 4.1±2.1 mm respectively, where as in Group C it was 26.20±1.7°, 143±2.7°, 6.5±2.4 mm respectively. From our study we conclude that reduced ETA, increased TTA and reduced PTD may be predisposing factor in the development of COM and Cholesteatoma.
Keywords
COM; Cholesteatoma; HRCT Temporal Bone; Reid Plane ET Angle
Download this article as:| Copy the following to cite this article: Babu S, Susan P, Saikiran P. Evaluation of Eustachian Tube CT Measurements in Patients with COM and Cholesteatoma. Biomed Pharmacol J 2020;13(2). |
| Copy the following to cite this URL: Babu S, Susan P, Saikiran P. Evaluation of Eustachian Tube CT Measurements in Patients with COM and Cholesteatoma. Biomed Pharmacol J 2020;13(2). Available from: https://bit.ly/2NQXvzm |
Introduction
Chronic otitis media (COM) is a long term infection of middle ear and mastoid cavity with frequent ear discharges through a tympanic perforation. The prevalence of COM is 65 to 330 million persons in worldwide, of them 60% of individuals will have hearing impairment. Chronic otitis media is a complication of enduring Acute otitis media (AOM) . The point in time when AOM becomes COM is not known [Figure 1]. Environmental, genetic and craniofacial abnormalities are common risk factors for the development of AOM to COM 1-4. Despite these factors, the anatomical position of Eustachian tube (ET) has role in development of COM and cholesteatoma. ET has a vital part in managing the function of middle ear. ET is helpful in maintaining ventilation, clearing secretions, and protection of middle ear. Shorter and horizontal ET in adults might be responsible for recurrent AOM which leads to development of COM and Cholesteatoma5-9. Previously ET measurements were done on cadavers. Presently with the advent of High Resolution Imaging of Temporal bone and multiplanar reconstruction (MPR) techniques, measurements of ET were done using CT imaging10-14. There are less studies which measured the ET Measurements in patients having COM without cholesteatoma and patients with COM and cholesteatoma. Hence, we performed the above measurements in both the groups and compared with group of normal ears.
 |
Figure 1: Pathogenesis of Chronic Otitis Media |
Materials and Methods
The approval for study was obtained from Institutional Research Committee, School of Allied Health Sciences and Institutional Ethics Committee, Kasturba Hospital, Manipal. This is a retrospective study. A total of 79 patients (47 males, 32 females, age range: 15-81 years) indicated for temporal bone High resolution CT from June 2016 to June 2018 were included. Of 79 patients, Group A included 54 ears who had COM without cholesteatoma (26 Unilateral, 14 Bilateral) and Group B included 39 ears who had COM with cholesteatoma (19 unilateral and 10 Bilateral). Patients who underwent HRCT PNS with no pathologies related to middle ear were included as controls. Group C included 158 ears (79 patients) with normal ears. The diagnosis of COM and Cholesteatoma was made by clinical examination such as otomicroscopy & audiometry, mastoidectomy. All the patients of Group A and Group B had otorrhea recuurently with surgical confirmation of COM and cholesteatoma.
The HRCT temporal bone scanning was done on 64-slice scanner Brilliance CT (Philips Medical systems, Netherland). The axial slices were obtained with 0.9 mm thickness. For controls, the images of PNS were reconstructed retrospectively with slice thickness of 0.9 mm, matrix of 1024 x 1024 and evaluated.
The ET angle was defined as the plane going through the inferior border of orbit and the superior border of external auditory meatus [EAM] and the intersecting line between the pharyngeal and tympanic orifices [Figure 2]. The tubo-tympanic angle was measured on axial section by a line between tympanic orifice and longitudinal plane of EAM [Figure 3]. The pretympanic diameter was defined as funnel portion of the EAM nearer to the tympanic orifice on axial section [Figure 4].
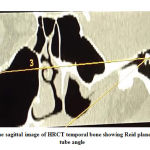 |
Figure 2: Oblique sagittal image of HRCT temporal bone showing Reid plane – Eustachian tube angle |
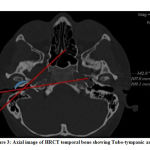 |
Figure 3: Axial image of HRCT temporal bone showing Tubo-tympanic angle |
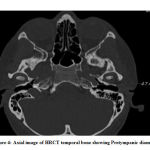 |
Figure 4: Axial image of HRCT temporal bone showing Pretympanic diameter |
The readers A and B were blinded to the diagnosis and performed measurements at different times to find the intra and interobserver variability
Statistical Analysis
The data analysis was done using statistical package for social sciences (SPSS) version 20.0. The Mann-Whitney U test was performed for the three measurements between three groups. The intra-observer variability was calculated using students -t- test. The inter observer variability was calculated using Intra-class correlation coefficient.
Results
In this study 40 patients who had COM without cholesteatoma and 39 patients who had COM with cholesteatoma and 79 patients with no pathologies in the ears were included.
The mean ET angle for the groups A, B and C was 24.30±1.6°, 21.18±1.4°, & 26.20±1.7° respectively [Figure 5]. There was statistically significant difference of Reid plane ET angle between the three groups (p<0.001) [Table 1]
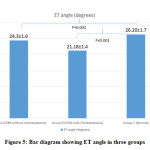 |
Figure 5: Bar diagram showing ET angle in three groups |
Table 1: Shows the Reid plane – Eustachian tube angles for three groups
| Study group | No. of cases | ET Angle (degrees) | p-value |
| Group A (COM without Cholesteatoma)
|
40 | 24.30±1.6 | p<0.001 |
| Group B (COM with Cholesteatoma)
|
39 | 21.18±1.4 | p<0.001 |
| Group C (Normal) | 79 | 26.20±1.7 |
The mean Tubo-tympanic angle for the groups A, B and C was 146±3.2°, 148±4.2° & 143±2.7° respectively [Figure 6]. There was statistically significant difference of tubotympanic angle between the three groups (p<0.001) [Table 2]
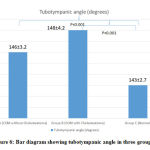 |
Figure 6: Bar diagram showing tubotympanic angle in three groups |
Table 2: Shows the Tubo-tympanic angles for three groups
| Study group | No. of cases | Tubo-tympanic Angle (degrees) | p-value |
| Group A (COM without Cholesteatoma)
|
40 | 146±3.2 | p<0.001 |
| Group B (COM with Cholesteatoma)
|
39 | 148±4.2 | p<0.001 |
| Group C (Normal) | 79 | 143±2.7 |
The mean Pretympanic diameter for the groups A, B and C was 5.5±2.2 mm, 4.1±2.1 mm & 6.5±2.4 mm respectively [Figure 7]. There was statistically significant difference of pretympanic diameter between the three groups (p<0.001) [Table 3]
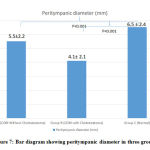 |
Figure 7: Bar diagram showing peritympanic diameter in three groups |
Table 3: Shows the pretympanic diameter for three groups
| Study group | No. of cases | Pretympanic diameter (mm) | p-value |
| Group A (COM without Cholesteatoma)
|
40 | 5.5 ± 2.2 | p<0.001 |
| Group B (COM with Cholesteatoma)
|
39 | 4.1 ± 2.1 | p<0.001 |
| Group C (Normal) | 79 | 6.5 ±2.4 |
There was no interobserver (p>0.01) and no intra observer (intra-class correlation coefficient = 0.89) variability was noted.
Discussion
Eustachian tube is complex and inaccessible structure to study. Several histological studies have measured the Eustachian tube angle and length. However, they are subjected to errors in tissue processing and sectioning errors. Presently with advances in imaging methods, the focus has been shifted from histology to using imaging techniques such as Computed Tomography with high resolution capabilities for examining Eustachian tube anatomy.10-14
The greater the horizontal positioning and shorter Eustachian tube leads to increase in bacterial backflow from to middle ear and it is main cause of transformation of acute to chronic otitis media. The increased horizontal position also leads to disturbance in passage of middle ear secretions 2,15
Takasaki et al. 10 studied the ET angle and length in children with COM and without COM as well as in normal adults. They found that the ET angle and length is similar on both right and left sides in children and adults. They also stated that the ET was more horizontal and shorter in children compared to adults which may be etiological factor for recurrent otitis media in children. In the present study the Reid plane-ET angle was 26.20±1.7, which is similar to Takasaki et al .10
Aksoy et al.11 studied the ET angle and Tubotympanic angle in patients with COM without Cholesteatoma, Patients with COM and Cholesteatoma and normal patients. They found reduced ET angle in patients with COM and cholesteatoma and almost similar angle between patients with COM and Normal ears. In the present study the ET angle for patients with COM and Patients with COM and cholesteatoma was 24.30±1.6, 21.18±1.4. In our study, The ET angle in patients with cholesteatoma were much reduced compared to Aksoy et al. 11. However, their study showed no significant difference in tubotympanic angle between the two groups where as our study showed significant difference in Tubo-tympanic angle between the patients with COM and Patients with COM and Cholesteatoma.
Dinc et al.12 also stated that ET angle was found to be smaller in patients with intratympanic tympanosclerosis (ITTS), tympanic membrane with retraction pockets (TMRP), cholesteatoma compared to normal. They also found ET angle to be more horizontal in males compared to females.
Sanjana Vijay Nemade et al. 13 studied the Eustachian tube angles and pretympanic diameters in patients with COM and normal ears. The ET angle, Tubo-tympanic angle and pretympanic diameter in patients with COM was 25.41 ± 2.57°, 148.12 ± 3.43° and 5.37 ± 2.10 mm where as in healthy patients it was 27.56 ± 3.62°, 145.14 ± 4.34° and 6.47 ± 2.40 mm respectively. They measured the pretympanic diameter to assess the patency of Eustachian tube and noticed reduction of diameter in blocked ET which is also evident from our study
Nasution et al. 14 found that ET angle was more horizontal in men compared to women and they also stated there is difference in ET angle between the patients with COM and in COM patients with Cholesteatoma.
In our study we found that the ET angle and pretympanic diameter was reduced in patients having COM without cholesteatoma and patients having COM with cholesteatoma, this would influence the pneumatization process of mastoid air cells because of inadequate ventilation of the middle ear and mastoid, thus predisposing factor for development of COM and cholesteatoma. In our study, we found tubotympanic angle obtuse in Group A & B compared to Group C. This would surge the possibilities of infections spreading to middle ear and influential factors for development of COM and cholesteatoma.
The ET angle measured in our study was similar to recent literature stated by Takasaki et al 10, Aksoy et al11, Sanjana Vijay Nemade et al 13and Naustion et al14. The tubotympanic angle measured in our study showed significant difference between the two groups contrary to the findings of Aksoy et al11. The peritympanic diameter measured in our study was similar to recent literature stated by Sanjana Vijay Nemade et al 13, they also noticed reduced peritympanic diameter which is evident in our study also.
We assume from the findings of our study that greater the horizontal position of ET anlge, and increase tubotympanic angle and reduced peritympantic diameter may be key etiological factors in the development of COM and cholesteatoma.
The pitfalls in our study are firstly, we did not analyze the association of gender for ET measurement and second is limited sample size Thirdly, we did not group the subjects as pediatrics and adults, we also did not assess the difference in measurements between pediatrics and adults.
Conclusion
High resolution imaging of temporal bone using CT with multiplanar reformation capabilities is a reliable method to evaluate the Eustachian tube anatomy. Although development of COM and cholesteatoma is multifactorial, we conclude that more horizontal position of Eustachian tube angle, increased Tubo-tympanic angle and reduced pretympanic diameter may be predisposing factor in the development of COM and Cholesteatoma. These measurements would be helpful in assessing the ET function.
Acknowledgments
Nil
Conflicts of Interests
There is no conflict of interest.
Funding source
This research did not receive any specific grant from funding agencies
References
- Verhoeff M, van der Veen EL, Rovers MM, Sanders EA, Schilder AG. Chronic suppurative otitis media: a review. Int J Pediatr Otorhinolaryngol.,70:1–12 (2006).
- Bluestone CD. Epidemiology and pathogenesis of chronic suppurative otitis media: implications for prevention and treatment. Int J Pediatr Otorhinolaryngol.,42:207 (1998).
- Rupa V, Jacob A, Joseph A. Chronic suppurative otitis media: prevalence and practices among rural South Indian children. Int J Pediatr Otorhinolaryngol., 48:217 (1999).
- Monasta L, Ronfani L, Marchetti F, et al. Burden of disease caused by otitis media: systematic review and global estimates. PLoS One.,7:e36226 (2012).
- Shim HJ, Choi AY, Yoon SW, Kwon KH, Yeo SG. The value of measuring eustachian tube aeration on temporal bone CT in patients with chronic otitis media. Clin Exp Otorhinolaryngol.,3:59-64 (2010).
- Smith ME, Scoffings DJ, Tysome JR. Imaging of the Eustachian tube and its function: a systematic review. , 58:543-556 (2016).
- Peter morris. Clinical evidence handbook. Am Fam Physician, 88(10):694-696 (2013).
- Tos M. Importance of eustachian tube function in middle ear surgery. Ear Nose Throat J., 77(9):744–747 (1988).
- Swarts JD, Alper CM, Luntz M, et al. Panel 2: eustachian tube, middle ear, and mastoid-anatomy, physiology, pathophysiology, and pathogenesis. Otolaryngology Head Neck Surgery.,148:26–36 (2013).
- Takasaki K, Takahashi H, Miyamoto I, Yoshida H, Yamamoto‑Fukuda T, Enatsu K, et al. Measurement of angle and length of the eustachian tube on computed tomography using the multiplanar reconstruction technique. ,117:1251‑4 (2007).
- Aksoy S, Sayin I, Yazici Z M, Kayhan F T, Karahasanoglu A, Hocaoglu E and Inci E.The evaluation of the angles of eustachian tubes in the patients with chronic otitis media on the temporal computerized tomography. J. Clin. Pract.,19 318-22 (2016).
- Dinc A E, Damar M, Ugur M B, Ilker I, Elicora S S, Biskin S and Tutar H. Do the angle and length of the eustachian tube influence the development of chronic otitis media? Laryngoscope J., 125: 2187-92 (2015).
- Sanjana Vijay Nemade , Kiran Jaywant Shinde, Varsha P. Rangankar, Priya Bhole. Evaluation and significance of Eustachian tube angles and pretympanic diameter in HRCT temporal bone of patients with chronic otitis media. World Journal of Otorhinolaryngology-Head and Neck Surgery., 4: 240-245 (2018).
- Rissa Ardika Nasution, Devira Zahara, Askaroellah Aboet.The Diffrentiation of the Angles of Eustachian Tubes in the Patient Chronic Suppurative Otitis Media With and without Cholesteatoma. Indonesian Journal of Medicine., 2(1): 73-78 (2017).
- Bluestone C D. Physiology, pathophysiology, and pathogenesis Otitis media in infant and children (BC Decker Hamilton) pp 41-72. (2007).

