
Manuscript accepted on :21-10-2019
Published online on: 12-12-2019
Plagiarism Check: Yes
Reviewed by: Francesca Gorini
Second Review by: Cherry Bansal
Final Approval by: Dr. Ian James Martin
Nandini N Manoli* and Bhavya Kotla
Department of Pathology, JSS Medical College and Hospital, a constituent of JSSAHER, India
Corresponding Author E-mail: nandinimanoli65@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1831
Abstract
Thyroid Fine needle aspiration cytology (FNAC) has gone through a paradigm shift in approach towards thyroid lesions. The 2017 Bethesda classification has helped to redefine the various conditions of the thyroid. An attempt has been made to utilize the classification with an example in each category. A total of 274 cases were studied over a period of one year (2018)( from January to December) at a tertiary referral hospital. The majority of cases were non neoplastic accounting to 246 cases with neoplastic cases accounting for 28 cases. The other ancillary techniques like use of Agnors, Morphometric, Pattern analysis, Cell block, ICC (immunocytochemistry) with LBC (Liquid based cytology) have been highlighted. Brief mentions of molecular techniques and recent advances, newer concepts like NIFTP have been discussed to highlight their utility in surgical management of Thyroid.
Keywords
FNAC; Thyroid; Bethesda system NIFTP
Download this article as:| Copy the following to cite this article: Manoli N. N, Kotla B. Recent Concepts in Thyroid Cytology with Emphasis on Ancillary Techniques. Biomed Pharmacol J 2019;12(4). |
| Copy the following to cite this URL: Manoli N. N, Kotla B. Recent Concepts in Thyroid Cytology with Emphasis on Ancillary Techniques. Biomed Pharmacol J 2019;12(4)..Available from: https://bit.ly/2YMkP63 |
Introduction
Fine Needle Aspiration Cytology (FNAC) of Thyroid is a useful, cost effective rapid painless outpatient accurate method for patient with thyroid conditions. Significant numbers of thyroid nodules, almost quarter of the cases are classified in the indeterminate category which includes Bethesda categories 3rd, 4th and 5th according to the 2017 Bethesda system of reporting thyroid cyto-pathology. This makes it difficult for management of the cases (1).
Many clinicians and pathologists have come up with various methods to improve and subcategorize the various cytological subgroups which have been possible by the latest Bethesda system 2017(2).
In South East Asian countries where thyroid lesions are common , many of the endocrinologist and pathologist have established their own system of clinical practice, reporting and their own methodology of management of thyroid cases which follow the American Thyroid Association (ATA) guidelines and the Bethesda system(3).
There are new concepts like UMP (Uncertain Malignant Potential) and NIFTP in the thyroid tumor classification. There are recent studies which put NIFTP (Non-Invasive Follicular Neoplasm with Papillary –like nuclear features) as a newly designated category for 10%-30% of thyroid carcinomas. (4)
The ancillary studies which can be done on thyroid FNA material and liquid –FNA helps in molecular testing of thyroid tumors with the introduction of Next Generation Sequence (NGS) for DNA and RNA. It helps in reducing ambiguity and sub categorizes the cases on cytology to improve the management of thyroid cases. (5)
The present article will deal with the latest Bethesda classification 2017, its use by presenting cases in each category and discuss the recent concepts of thyroid cytology:
The 2017 Bethesda System for Reporting Thyroid Cytopathology: includes
Category-1 Nondiagnostic Or Unsatisfactory,
Category-2 Benign,
category-3 Atypia Of Undetermined Significance Or Follicular Lesion Of
Undetermined Significance
category-4 follicular neoplasm or suspicious for a follicular neoplasm
category -5 Suspicious For Malignancy
category-6 Malignancy- (6).
Material and Methods
Total number of thyroid cases sent to the Department which underwent FNAC in the year 2018 was 274 in number of these 44 cases were under ultrasound guidance. The rest 230 cases were done by the conventional method. Non neoplastic cases made up for benign category totaling to 246 cases while 28 cases were neoplastic. (Table-1)
The non-neoplastic cases included Colloid Goiter, Nodular colloid Goiter, Hashimotos and lymphocytic thyroiditis. The neoplastic conditions of thyroid included cases belonging to various Bethesda categories. We have presented with example for each category
Table 1: Case Distribution Of Thyroid Lesions On Cytology
| Case | Conventional FNAC | USG Guided FNAC | Total |
| Colloid Goitre | 96 | 21 | 117 |
| Nodular Goitre | 10 | 2 | 12 |
| Autoimmune Thyroiditis | 1 | 1 | |
| Hashimoto’s | 47 | 6 | 53 |
| Lymphocytic | 58 | 5 | 63 |
| Follicular Neoplasm | 13 | 4 | 17 |
| Papillary Carcinoma | 5 | 5 | 10 |
| Medullary Carcinoma | 1 | 1 | |
| Total | 230 | 44 | 274 |
Approach to Thyroid FNAC
Approach to thyroid swelling includes a combination of clinical findings, radiological imaging with fine needle aspiration findings. The position of patient during the procedure of FNAC should be in supine position. Increased exposure of gland is done by keeping pillow under neck with instructions to patient, to keep still and refrain from swallowing. The numbers of passes required for an adequate thyroid aspirate are 2-4 passes. Depending on the size of the lesion, it can increase to 6-8 passes so as to represent the whole thyroid. The needle should have different angles or points of entry. (7)
The needle gauge used and technique of making smears are 24-27 gauge needle
For a hemorrhagic aspirate two step techniques should be used. If colloid material is aspirated, the aspirate should be subjected to centrifugation & deposit should be made into 1-2 smears and stained by Haematoxylin and Eosin (H&E), May-Grünwald Giemsa (MGG) and Papanicalaou (PAP) stain(7)
Procedure of FNAC
The procedure for FNAC thyroid is by two techniques, the routine technique is by aspiration using 10ml syringe and needle (24-27g). In cases with haemorrhage, a non-aspiration sampling technique using only needle can be done. Both the techniques can be done under ultrasound guidance for non-diagnostic or unsatisfactory cases (7).
The Stains Used are
PAP – for malignancy; MGG for background, colloid, fibroblasts: H&E for routine (7)
Category -1 Non diagnostic or unsatisfactory
Every thyroid FNA for diagnosis on cytology should be adequate or have a satisfactory smear. For an adequate or satisfactory smear for evaluation Bethesda criteria has been put forth. The criteria includes at least six groups of benign follicular cells with each group having at least 10thyroid follicular cells.
The 2017 Bethesda BSRTC reinforces that if there is an abundant colloid or a specific diagnosis can be rendered or whenever there is significant atypia, the specimen is by definition adequate for evaluation.
Conditions where a definite diagnosis cannot be rendered due to increase in blood in smear , improper cell preservation and decrease in thyroid follicular cells, the diagnosis of unsatisfactory (UNS) or non-diagnostic (ND) ND/UNS is given(8).
This can be reduced by advising sonographic guidance, which is diagnostic in most cases. Surgery is advised if clinical and sonographic suspicion of malignancy is present.
Category -2 Benign
A case of a 50year old Female with Clinical findings of neck swelling from midline to right side of neck. The swelling moves with deglutition. It is 3×3 cms in size with soft consistency. Clinical diagnosis is colloid goiter. Ultrasound finding shows a multi-nodular goiter with colloid degeneration. Biochemical findings areT3-1.62, T4- 12.11, TSH-0.005
Microscopy: Aspirate is satisfactory with smears which are moderately cellular. Benign thyroid follicular cellsare seen and arranged in sheets. Background shows thick and thin colloid, with cyst macrophages.(Fig-1)
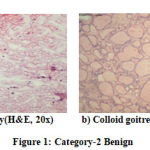 |
Figure 1: Category-2 Benign |
The diagnosis was confirmed by Histopathology as Nodular Colloid Goiter. The various differentials for multinodular goiter should be taken into consideration whenever the cellularity is more. The nuclear features mainly help to distinguish between nodular colloid goiter, follicular neoplasm with micro follicles and cystic papillary carcinoma thyroid. The presence of abundant colloid in the background also helps in making a more definitive diagnosis. (9, 10)
Category -3 AUS/FLUS
A 32year old female with midline swelling since one year which is 3x2cms in size ,oval, firm in consistencyis presented with Clinical diagnosis of Nodular colloid goiter. Ultra sound findings are: Nodular colloid goiter, showing heteroechoic lesion with hypo echoic halo, increased peripheral and internal vascularity.
Microscopy
Aspirate is satisfactory. Smears studied shows thyroid follicular cells arranged in micro follicles. Background shows blood.
The diagnosis observed was Follicular Neoplasm/Follicular lesion of undetermined significance (FLUS) /Atypia of undetermined significance (AUS)Advised-Histopathological Examination, Immune markers on cell block. Histopathology gave a diagnosis of Follicularadenoma. Conditions associated with AUS and their importance is3-6% of thyroid FNAC report, presence of architectural atypia and cellular atypia. The atypia is not sufficient to call follicular neoplasm or suspicious for malignancy, nor can be dismissed as benign/follicular lesion. Impression is it has a small but definite risk of malignancy which lies between that of benign and follicular neoplasm (5-10%).
The specific scenarios for AUS/FLUS (follicular lesions of undetermined significance) are,
nuclear features like ground glass appearance, nuclear grooving in an otherwise predominantly benign appearing sample.
Predominance of micro follicles in a sparsely cellular aspirate with scant colloid. Follicular cell atypia hindered by a sample preparation artifact (air- drying artifact or clotting artifact).
Presence of hurtle cells ina clinical setting suggesting chronic lymphocytic thyroiditis or multinodular goiter.(11,12)
Approach to cellular thyroid aspirates in follicular patterned lesions.
Whenever majority of the thyroid aspirate shows uniformly arranged follicles of thyroid cells with lumen filled with colloid on microscopic examination a diagnosis of follicular neoplasm is offered. The follicles can be based on their size either micro follicles or macro follicles; some lesions have both but a pattern dominates this follicular neoplasm on cytology can be further diagnosed as benign or malignant by the help of IHC markers or by BRAF molecular testing. (13)
Category -4 Follicular Neoplasm/ Suspicious of Follicular Neoplasm-FN/SFN
The history is of a 30years old, Female with swelling in front of the neck from 6months 2×3 cms solitary nodule. Clinical diagnosis Colloid goiter. Ultrasonography showed features of thyroid lobe which is bulky and shows an isoechoic solid lesion, few hypo echoic areas noted within it. It shows both internal and peripheral vascularity. TiradsIVa, T3-0.898 T4-7.18, TSH-1.84.
Microscopy
Aspirate shows moderately cellular smears which thyroid follicular cells arranged in micro follicles with mild nuclear atypia. Background shows blood. (Fig-2)
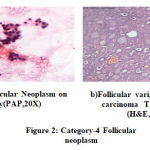 |
Figure 2: Category-4 Follicular neoplasm |
Diagnosis
Follicular Neoplasm or suspicious for a Follicular Neoplasm. Differential of (follicular variant of papillary carcinoma thyroid FVPTC).and NIFTP(noninvasive follicular thyroid neoplasm with papillary–like nuclear features).
Advised Molecular testing, Surgery after risk Assessments definitive distinction between FVPTC and NIFTP is not possible on cytology alone. The diagnosis given on histopathology was Follicular Variant of Papillary Carcinoma of Thyroid.
Follicular-patterned cases with mild nuclear changes (increased nuclear size, nuclear contour irregularity, and/or chromatin clearing) can be classified as FN/SFN.6There should not be even a single papillae or a pseudo inclusion favouring a papillary carcinoma. A note of caution regarding follicular variant of papillary carcinoma or NFTIP should be mentioned with advice for molecular testing or IHC.
Category -5 Suspicious of malignancy
The clinical history is of a case of a 58 years old female with swelling in front of neck, 4×3 cm, globular and firm. Clinical Diagnosis was Colloid goiter. Ultrasound findings: Colloid nodules in both lobes of thyroid, cervical level II and III lymph nodes noted reactive. Right lobe swelling 3.7×7.5mm and left lobe 5×3 mm.
Microscopy
Smears are cellular and show pleomorphic cells showing abundant cytoplasm with hyper chromatic nucleus. Single tumorcells seen in the background. Amorphous amyloidseen which stained with Congo red. Cell Block shows Calcitonin positive tumor cells. (Fig-3)
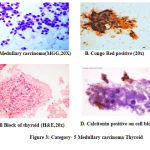 |
Figure 3: Category- 5 Medullary carcinoma Thyroid |
A diagnosis of malignant thyroid neoplasm was done on cytology with suspicion of medullary carcinoma. Confirmation was done by using special stain Congo Red on cytology slide and on histopathology section. IHC Calcitonin was done on cell block which showed positivity .Serum Calcitonin level assay showed raised levels. Diagnosis of Medullary carcinoma thyroid was confirmed both by histopathology and IHC on cell block.
Medullary thyroid carcinoma (MTC) is a rare, well differentiated neuroendocrine carcinoma that arises from parafollicular thyroid cell. It accounts for approximately 1-2% of thyroid malignancies (14).As medullary carcinoma presents with a wide variety of histologic patterns, it is important to perform immuno-histochemistry in any thyroid tumour that lacks definite colloid or is simply not typical of another type of thyroid carcinoma.
Amyloid is a characteristic histologic feature in Medullar thyroid carcinomas (MTC).and present in approximately 80% of the tumors and is composed of Calcitonin secreted by the tumour cells. Amyloid can be readily detected by histochemical stains such as Congo red(15).Calcitonin is the most useful marker for the diagnosis of MTC, with a good sensitivity ranging from 74% to 100% on cytology(16).
Calcitonin has been identified in the amyloid stroma by immuno- histochemistry and immunofluorescence. Congo red and Calcitonin were used on cytology & cell block respectively with confirmation of the case by histopathology.
Category-6 Malignancy
History of a 43year old female, with clinical features of neck swelling, measuring 3x3cms firm solitary nodule. Clinical diagnosis: was Colloid goiter, Ultrasound showed well defined solid hyper echoic nodule in right lobe of thyroid with peripheral and central vascularity and multiple calcifications TIRADS IVA, T3-1.37, T4-8.12, and TSH 4.42.
Microscopy
Aspirate is satisfactory. Smears are highly cellular. Smears studied show tumor cells arranged in papillary fronds, sheets and clusters. Individual tumor cells are arranged in pallisading pattern. Nuclear grooves and intranuclear inclusions seen. Background shows colloid and blood. The diagnosis offered is Papillary Carcinoma Thyroid which was confirmed on Histopathology. (Fig-4)
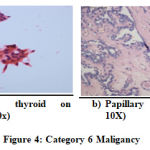 |
Figure 4: Category 6 Maliganc |
Cytologic Major & Minor criteria’s for diagnosis of Papillary Carcinoma
Major criteria
Enlarged oval and irregular nuclei, fine chromatin, multiple eccentric micronucleoli. Longitudinal chromatin ridge or nuclear groove, intranuclear cytoplasmic inclusions. All criterias are essentially nuclear. A constellation of features are necessary for diagnosis.
Minor criteria
The minor criteria are the following.Papillarycyto-architecture with syncytial monolayers, thick colloid ,psammoma bodies with calcific debris,occasional giant cells,andhistiocytoid cells(17).
Ancillary Techniques
Use of AgNORS in Thyroid Lesions
Nucleolar organizer regions (NORS) can be located by using silver nitrate on cytopreparations. It is a simple, easily manageable, reproducible and cost-effective method for differentiating benign from malignant lesions of thyroid. Colloid Goitre is taken as the control for studying any condition of thyroid(18).
Role of morphometry in diagnosis of Follicular Neoplasms
Four nuclear parameters are selected and compared with a standard the factors of the nucleus assessed are Mean nuclear area, Mean nuclear perimeter, largest to smallest diameter ratio of the nuclei, and coefficient of variation of the nuclear areait helps to differentiate between benign and malignant follicular neoplasm(19)
Uses of Liquid Based Cytology in Thyroid FNAC
Artifacts caused by conventional sample method account for significant proportion of inconclusive or AUS/FLUS results in thyroid FNA. Liquid based cytology helps to improve the diagnosis and reduce the number of AUS/FLUS.
It is done by improving the quality of cytomorphology with absence of obscuring elements and preservation of cells adequately. It helps in using the residual material obtained by LBC for ancillary studies. Eg. like molecular testing for BRAF/RAS in Papillary carcinomas.(20)
Role of Cell Block in Thyroid FNAC
Advantages are that the cell block section helps in meeting the architectural details especially to differentiate papillary carcinoma from papillary hyperplasia. It helps in diagnosing papillary carcinoma of thyroid at metastatic sites. Marker studies, special stains can be done on cell block preparations for better diagnostic accuracy of thyroid nodules. Confirmation of malignant thyroid conditions, can be done be IHC studies on cell block. (21)
Role of immunocytochemistry in Thyroid lesions.
Immunocytochemistry (ICC) and cytoenzymology (CE) are widely available nowadays in the market and be used to diagnose intermediate categories of thyroid conditions. They can be performed on smears (cell blocks, or liquid-based preparation).
Markers that are, most important for diagnosis on thyroid FNA are Hector Battiforamesothelial antigen-1 (HBME-1), thyroid peroxidase (TPO), and dipeptidylaminopeptidase IV (DPP4) can be used directly on smears. TTF-1, Thyroglobulin & Calcitonin are primary thyroid markers to identify and distinguish the cell type in less well differentiated neoplasms.(22)
Cytokeratin 19 and CD44 are helpful in distinguishing Papillary carcinoma from other thyroid neoplasms & metastatic papillary carcinoma to thyroid. Gelectin – 3 & CD44v6 are helpful in diagnosing follicular carcinoma. CD markers are helpful to confirm lymphoma in thyroid.Immunohistochemical markers including galectin-3, Hector Battiforamesothelial cell-1 (HBME-1), and cytokeratin-19 can be used to differentiate between benign and malignant thyroid lesions, the latter ,in which it can be diffusely expressed.(23)
Approach to cellular thyroid aspirates in follicular patterned lesions
There can be a method of pattern analysis in diagnosis of solitary nodule thyroid. Diagnostic accuracy by pattern analysis is very high, with specificity and sensitivity. It reduces the number of surgeries. It is reproducible. Various studies by different authors have found it to be an efficient and clinically reliable method(24)
Role of Radiology
Advantages of ultrasonography in FNAC of thyroid
Ultrasonography (US) has several advantages over palpation. in approaching thyroid FNAC, Real-time US permits visualization of the needle within the lesion,this helps to reach and aspirate small nonpalpable thyroid nodules which are suspicious of cancer . Even in palpable thyroid nodules, US guidance is superior to palpation as it helps to obtain the correct and adequate material for diagnosis of the lesions. it thus improves diagnostic accuracy of thyroid lesions .(25)
Recent Advances
FNAC of thyroid has under gone many changes with many advances in the diagnostic categories brought in by Bethesda classification 2017. There are many cases in the indeterminate category AUS/FLUS, (Low-risk) to Follicular neoplasm/ Suspicious for Follicular Neoplasm (FN/SFN) of intermediate risk or suspicious for malignancy [SFM].
They are high risk on cytology, which need to be confirmed by other methods. Also it is imperative for other ancillary methods to be added to decide the surgical and clinical management of thyroid nodules. The emphasis of the latest classification is not to over diagnose and over treat benign cases of thyroid which present as solitary nodule. (26,27)
The new classification of thyroid which comes under the Endocrine Tumour classification includes borderline tumours. The new terms included are UMP and NIFTP wherein. (UMP) means uncertain malignant potential, NIFTP (non-invasive follicular neoplasm with papillary –like nuclear features)which comes under the 2A2 category of the latest classification of endocrine tumor .(28)
NIFTP comes under category 3rd of Bethesda classification FN/SFN which accounts for (10% to 30%) of Follicular neoplasms and has an indolent course. Another aspect of follicular neoplasm FVPTC (follicular variant of papillary thyroid carcinoma) has also to be noted and diagnosed by ancillary techniques. (4)
There have been advances in techniques to differentiate the different low risk to high risk FN/SFN to AUS/FLUS from benign and malignant. These are molecular testing techniques to detect changes in DNA and RNA of thyroid follicular cells by using next generation sequencing (NGS). (5)
The material for extracting DNA or RNA material can be done by using directly the FNA material or liquid based fine needle aspiration LB-FNA to improve mutation profiling. It thus improves diagnostic accuracy and thus avoids unwanted thyroid ectomies. These help to decrease the number of indeterminate nodules in thyroid. (29)
Molecular methods used are
Affirm a gene expression classifier.
This uses micro RNA profiles for the diagnosis of indeterminate nodules where surgery is not desirable. Material collected from two needle passes are preserved in RNA preservative. Good number of gene profiles from the common 142 genes to the high risk 25 gene profiles are studied. Any of the important 6 gene profiles, if they show changes then the nodule are considered suspicious.(30)
BRAFV 600E
Gene mutation alone is an important marker to indicate malignancy, It is present in more than 99% of thyroid nodules and thus helps to differentiate the lesion from FN/SFN Bethesda 5th from malignancy Bethesda 6th which is important for surgical management.(31)
The seven gene test.
A panel of combination of BRAF V600E, PAX8/PPARG, RET/PTC, HRAS, KRAS and NRAS is the seven gene panel. Another test panel which can be suggested wherever possible as it has been shown to have greater sensitivity and specificity.(32)
Thyroseq v2 full ngs panel.
The ThyroSeq v2 panel uses NGS for simultaneous analysis of multiple genes. ThyroSeq v2 tests for point mutations and small insertions/deletions in 14 genes, 42 types of gene fusions, and expression levels of 16genes.it helps in detecting mutations or genetic changes in RET (medullary thyroid carcinoma) TERT promoter mutation, a mutation which is both a diagnostic and prognostic marker, and present at increased frequency in aggressive tumors such as poorly differentiated carcinoma and anaplastic thyroid carcinoma. It isalso associated with poor result like increased risk of distant metastasis, persistent disease, and cancer‐specific mortality. (33)This can be detected by use of thyroseq v2 (33)
NIFTP (Noninvasive follicular variant of papillary thyroid carcinoma).
The 2017 revised thyroid cytopathology (TBSRTC) has introduced a new category wherein it has reclassified noninvasive follicular variant of papillary thyroid carcinoma to a new term which is noninvasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) (6, 34)
the subset which is included in the Bethesda category 3 of FN/SFN represents a benign indolent well circumscribed thyroid tumour with follicular architecture , absence of any papillary structures but with nuclear features which overlap with those of papillary carcinoma.
The cytological diagnosis of this subgroup is difficult as capsular or vascular invasion cannot be commented about on FNA. Also as there is subtle overlap of nuclear features between benign NIFTP and follicular variant of papillary thyroid carcinoma (FvPTC) there is some limitation to categorize this indeteminate condition. (35)
Thus the factors which help to differentiate NIFTP from FVPTC rely on nuclear features which has an semiquantitative scoring system which are six parameters divided into three categories.
The three categories are,
Nuclear size, shape of nucleus whether overlapping or increased in size.
Nuclear membrane whether irregular contour or not.
Chromatin as to whether cleared or glassy appearance. A score of zero is given if each factor shows the features in less than 50% of the cells a score of one is given if more than 50% of the cells show the features. A total score ranges from zero to three. ( 36 )
If the score is (0/1) it is benign, score (1/2) NIFTP score (2/3) FVPTC, with slight overlapping of the nuclear features (37).
Molecular analysis of NIFTP
NIFTP has lineage towards RAS mutations rather than BRAF mutations. Thus, showing that they are less prone formetastasis. This leads to a more conservative approach to these neoplasms with thyroid lobotomy alone being enough and obviates the need for complete thyroidectomy and radiation.(38)
Conclusion
Thyroid FNAC has come a long way in diagnosis of thyroid conditions. The latest classification of thyroid. Bethesda 2017 helps to reduce the indeterminate cases of thyroid i.e. Bethesda 4th and 5th by the utility of IHC, Molecular testing and Liquid Based Cytology.
The new terms of NIFTP and FVPTC are given importance so as to reduce unwanted surgeries of indeterminate cases.
Acknowledgement
We acknowledge the help of our other colleagues, staff postgraduates and technicians who have participated in the process of diagnosis, processing and technical aspect of our work.
Conflict of interest
None
Funding
There was no funding from any agency for our work.
References
- American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, et al.
- Revised American thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-1214.
- Ali SZ, Cibas ES, eds. The Bethesda system for Reporting Thyroid Cytopathology. Definitions, Criteria and Explanatory Notes. New York, NY: Springer;2010.
- Kim M, Park HJ, Min HS, et al. The use of the Bethesda system for reporting thyroid cytopathology in Korea: a nationwide multicenter survey by Korean Society of Endocrine Pathology. J PatholTransl Med. 2017;51:410-417.
- Strickland KC, Howitt BE, Marqusee E, et al. The impact of noninvasive follicular variant of papillary thyroid carcinoma on rates of malignancy for fine needle aspiration diagnostic categories. Thyroid. 2015;25:987-992.\
- Goodwin S Mcpherson JD Coming of age: Ten years of next generation sequencing technologies . Nat Rev Genet. 2016;17:333-351.
- Cibas ES Ali SZ , The 2017 Bethesda system of Reporting Thyroid Cytopathology. Thyroid, 2017; 27:1341-1345.
- Jayaram G. Orell SR. SR Sterretts. GF Chap6, Thyroid Ed: Orell& Fine needle aspiration cytology 5th Edition, Churchill Livingstone, Pg 119-120.
- Renshaw A.A Histotogic follow-up of Non- diagnostic thyroid fine needle aspirations:Implications for adequacy criteria .Diagn cytopathol,2012,40;E13-15.
- Suen KC How does one separate cellular follicular lesions of the thyroid by fine needle aspiration biopsy? DiagnCytopathol 1988;4:78-81.
- Nassar A, Gupta P, LiVolsi VA etal. Histiocytic aggregates in benign nodular goiters mimicking cytologic features of papillary thyroid carcinoma (PTC). DiagnCytopathol 2003;29;243-5
- Harshan M, Corapanzano IP, Aslan DL etallPapillary thyroid carcinoma with atypical histiocytoid cells one fine needle aspiration Diagncytopathol 2009;37:244-250
- Song JY et all Reclassifying formerly Indeterminate thyroid FNAC using the bethesda system reduces the number of inconclusive cases ActaCytol 2012; 56 122-129
- Zubair W. Baloch, MD, PhD, and Virginia A. LiVolsi, MD, Follicular-Patterned Lesions of the Thyroid The Bane of the Pathologist American Society for Clinical Pathology, Am J ClinPathol 2002;117:143-150
- Nishino M, Pusztaszeri MP, Pitman MB. Medullary Thyroid Carcinoma. In: Ali S, CibasE. (Eds) TheBethesda System for Reporting Thyroid Cytopathology. Definitions Criteria and Explanatory notes 2nd Ed Springer, 2018;9:157-177.
- Erickson, LA, Vrana, JA, Theis, J.etal. Analysis of Amyloid in Medullary Thyroid Carcinoma by mass Spectrometry-Based Proteomic Analysis EndocrPathol2015; 26: 291-5.
- Pusztaszeri, MP. Md; Bongiovanni, M, Faquin, W.C.Updateonthecytologic and molecular features of medullary thyroidcarcinoma, Advances in Anatomic Pathology: 2014 ; 21: 26–35.
- Das DK Sharma PN Diagnosis of papillary thyroid carcinoma in fine needle aspiration smears. Factors that affect decision making ActaCytol,2009;53:497-506.
- AsotraSRole of Agnors in thyroid lesions on fine needle aspiration cytology smears.Journal of Cytology 2008;25-1: pg 18-22.
- ShanmugaP.SundaramS. Morphology to Morphometry in cytological evaluation of thyroid lesions 2011; journal of cytology, 2011;28,98-102.
- StamatakiM, Anninos D, Brountzosetall. The role of liquid based cytology in the investigation of thyroid lesions Cytopathology 2008;19:11-18.
- Fillie AC, Asa SL Geisirger KR etall Utilization of Ancillary studies in Thyroid Fine needle aspirates. A synopsis of the NationalCancer Institute Thyroid Fine needle AspiratonState of the Science conference, Diagnostic cytopathology, 2008; 36; 438-441.
- F,etalUniversal markers of thyroid malignancies: Galectin -3, HMBE-1, and Cytokeratin -19,Endo Pathol, 2010; 2:80-89.
- Maruta J, Hashimotoh H, Yamashita H etall. Immunostaining of Galectin -3 and CD 44v6 using fine needle aspiration for distinguishing follicular carcinoma from adenoma. DiagnCytopathol 2004;31:392-6.
- Lingegowda JB, Muddegowda PH, Rajesh Kumar N, Application of pattern analysis in fine needle aspiration of solitary nodule of thyroid 2010;27:1-7.
- Kim MJ, Kim EK, Park S. etall. US guided Fine needle aspiration of thyroid nodules Indications, Techniques and ResultsRadiographics 2008;28:1869-1886.
- Krauss EA, Mahon M, Fede JM etall Application of the Bethesda classification for thyroid fine needle aspiration. Arch Pathol Lab Med 2016;140:1211-1231.
- Kakudo .K, Kameyama. K, Miyauchi A, etall Introducing the reporting system for thyroid fine needle aspiration cytology according to the new guidelines of the Japan Thyroid association Endo cr.J 2014;61:539-552.
- RV, Osamura RY, Kloppel G, Rosai J Eds. WHO classification of tumour Endocrine organs, 4thEdn, Lyon, IAR,C, 2017.
- Petrucci MD, Descotes F, Depaepe L, Etall Molecular testing of BRAF, RAS and TERT on thyroid FNAC with indeterminate cytology improves diagnostic accuracy Cytopathology 2017;28:482-487.
- Santharam P, Khthir R, Gress. T. Gene Expression classifier for the diagnosis of indeterminate thyroid nodules with indetermine cytology N, Engle J Med 2012;367:705-715.
- Frais N, Soobiah. C,AbQahtaniK.etall, Diagnostic value of fine needle aspiration BRAF (V600E) Mutation analysis in papillary thyroid cancer: a systematic review and meta- analysis Human Pathol,2015:46:1443-1454.
- Eszlinger M, Bohme K, Ullmann M etallEvaluation of a two-year routine application of molecular testing of thyroid fine –needle aspirations using a seven-gene panel in a primary referral setting in Germany Thyroid 2017;27:402-411.
- Nikiforov YE, Carty SE, ChioseaSI,etalHighly accurate diagnosis of cancer in thyroid nodules with follicular neoplasm/suspicious for a follicular neoplasm cytologybyThyroseq v2next–generation sequencing assay. Cancer.2014; 120:3627-3634.
- K, Higuchi M, Hirokawa M, etallThyroid FNA cytology in Asian practice –Active surveillance for indeterminate thyroid nodules reduces over treatment of thyroid carcinomas. Cytopathlogy 2017; 28:455-466.
- Song SJ, LiVolsi VA, Montone K, Baloch Z. Pre‐operative features of non‐invasive follicular thyroid neoplasms with papillary‐like nuclear features: An analysis of their cytological, Gene Expression Classifier and sonographic findings. Cytopathology. 2017 Dec;28:488-94.
- Jaconi M, Manzoni M, Pincelli AI etall. The impact of the non-invasive follicular thyroid neoplasm with papillary like nuclear feature Terminology in routine diagnosis of thyroid tumour. Cytopathlogy 2017;28:495-502.
- Nikiforov YE, Seethala RR, Tallini G, Baloch ZW, Basolo F, Thompson LD, Barletta JA, Wenig BM, Al Ghuzlan A, Kakudo K, Giordano TJ. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA oncology. 2016 ,;2,:1023-9.
- Shrestha RT, Ruanpeng D, Hennessay JV cytomorphology of Non invasive Follicular thyroid Neoplasm with papillary like nuclear features and the impact of New nomenclature on molecular testing. Med.Sci 2019;7:2-9.

