
Manuscript accepted on :30-10-2019
Published online on: 21-11-2019
Plagiarism Check: Yes
Reviewed by: Lisa Scherer
Second Review by: Helena Felgueiras
Final Approval by: Dr. Francesca Gorini
Shanmugapriya V1 and Karthikeyan D2
and Karthikeyan D2
1Department of Biochemistry Vinayaka Mission’s Medical College, Karaikal, Puducherry UT – 609609, India
2Department of Microbiology Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamilnadu – 636308, India
Corresponding Author E-mail: priyasri_1011@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1827
Abstract
Alcoholism is now an emerging social and national health problem among adolescents and middle aged population. Alcohol consumption has doubled in the recent years and has increasing its complications. To analyze the metabolic variations in chronic alcoholics which include their BMI, liver function test, lipid profile, inflammatory markers, antioxidants level, insulin level and atherogenic index. The chronic alcoholics had increased BMI with grade 1 obesity with mean value of 30.8±2.4. The mean total cholesterol level (mg/dl) in cases was 232 ± 22.4. The mean HDL level (mg/dl) showed a significant variation among the study group as 38.8±7.8. The mean LDL and NHDL in cases were 148.6 ±15 and 170±17.8 respectively. The mean serum insulin level in study population was 22.36±5.8. The GGT level was increased as expected with mean value 112±13.9. Lipid peroxidation marker MDA was markedly increased in alcoholics with mean value of 14.6± 1.7. All the biochemical parameters in chronic alcoholics were significantly altered when compared to normal non-alcoholic individuals. Alcoholic patients were found to be dyslipidemic, grade I obese, oxidative stress with low levels of anti-oxidants, insulin resistant and prone to cardiac risks by developing atherogenesis.
Keywords
Alcoholism; antioxidants; cardiac risks; inflammatory markers
Download this article as:| Copy the following to cite this article: Shanmugapriya V, Karthikeyan D. A Study on Analysis of Cardio Vascular Risk Factors in Chronic Alcoholics. Biomed Pharmacol J 2019;12(4). |
| Copy the following to cite this URL: Shanmugapriya V, Karthikeyan D. A Study on Analysis of Cardio Vascular Risk Factors in Chronic Alcoholics. Biomed Pharmacol J 2019;12(4). Available from: https://bit.ly/338aYbp |
Introduction
As per the recent report by World Health Organization (WHO), alcohol consumption has increased to two folds in the last ten years in India .The highest increase is in South East Asia especially in India. Alcohol consumption is 2.4 liters in 2005, increased to 4.3 liters in 2010 and further increased to 5.7 liters in 2016. In 2016, more than 3 million people died due to various harmful effects of chronic alcoholism. In this, 28% of death is due to road traffic accidents, 21% due to gastro intestinal and digestive disorders and 19% of deaths due to cardiovascular diseases and remaining due to cancers, infectious diseases, mental disorders etc., [1]. Cardiac deaths due to alcoholism become preventable; when the rate and amount of alcohol intake has been decreased. In addition to this, alcoholism has become a national health problem decreasing the man power and national productivity. The toxic effect of alcohol results in multi organ failure including its effect on central nervous system.
As the metabolic capital of our body, liver is the major organ involved in metabolizing alcohol. In general alcohol means ethanol which is oxidized to aldehyde and then to acetic acid. The enzymes involved in alcohol metabolism are alcohol dehydrogenase and aldehyde dehydrogenase respectively. The intermediate product formed during this metabolism is aldehyde in the form of either acetaldehyde or formaldehyde, which accumulates in our body and produces toxic effects. This is due to the fact that the first enzyme alcohol dehydrogenase which converts alcohol to aldehyde is metabolically more active than the second enzyme aldehyde dehydrogenase which converts aldehyde to acid. The toxic effect continues resulting in free radicular damage that cause cell death and in due course leading to organ failure. The metabolism of all biomolecules has been altered. Lipid metabolism derangements results in triglycerides accumulation in liver which is called us fatty liver disease. Further triglycerides become the substrate for peroxidation reaction leading to cell damage. Because of high oxygen consumption, paucity of antioxidant mechanisms and abundant lipid content central nervous system is more prone to free radicular damage and neuronal death [2]. With this background knowledge, this study aims to analyze the metabolic variations in chronic alcoholics including the levels of inflammatory markers, antioxidant level, insulin resistance, atherogenic index, liver enzymes with lipid profile against a control group of apparently normal subjects from the general population.
Materials and Method
A total of 45 (Forty five) chronic alcoholics under the age of 50 years and 20 (Twenty) controls subjects were studied for their fasting blood sugar , lipid profile , liver function tests , inflammatory markers like hsCRP , MDA , Antioxidants like uric acid and vitamin C , insulin resistance, atherogenic index for assessing cardiac risk. Samples were collected from the patients and control subjects after getting the informed consent. Diabetic, hypertensive patients, smokers, patients on treatment for any other diseases, jaundiced patients were excluded from the study. Clinical parameters like blood pressure, pulse rate, height and weight were recorded for all the study subjects. Biochemical parameters like fasting glucose, total cholesterol, triglycerides, HDLc, liver function tests (LFT) which includes SGOT, SGPT, ALP, total protein and albumin , uric acid and hsCRP were done by their respective standardized kit methods. Calculated parameters include BMI, LDLc, VLDLc, NHDL, atherogenic index and HOMA -IR. LDLc and VLDLc were calculated by Friedwald’s formula [3]. Serum insulin and Vitamin C level were estimated by ELISA kit method after standardization. Plasma MDA level was estimated by Esterbauer and Steinberg’s method 1989 which is based on lipid peroxide condensed with 1 methyl-2 phenyl indole, under acidic condition. The level of lipid peroxides was measured in terms of MDA in spectrophotometer at the wavelength maximum of 586 nm .The normal level is taken as less than 4 µmol/L [4].
Results and Discussion
Study Parameters in Total Cases and Controls
Table 1: Table shows increased level of TC, TGL, ALP, GGT, hsCRP, MDA and atherogenic index in chronic alcoholism cases when compared with the control group. Whereas the level of HDL, VIT C and albumin were decreased in chronic alcoholics with the reference of control group.
| PARAMETERS | CASES | CONTROLS | |||
| FBS(mg/dl) | 88.6 ±16 | 82.7± 8.5 | |||
| PPBS(mg/dl) | 134± 12.6 | 122.4±9.5 | |||
| TC(mg/dl) | 232± 22.4 | 168±15.6 | |||
| TGL(mg/dl) | 156.9±12.8 | 98.7±9.7 | |||
| HDL(mg/dl) | 38.8±7.8 | 55.7±8.6 | |||
| LDL(mg/dl) | 148.6±15 | 100.4±14.5 | |||
| TC:HDLc | 5.4±0.8 | 3.1±0.4 | |||
| LDLc:HDLc | 3 .6±0.4 | 1.9±0.3 | |||
| NHDL(mg/dl) | 170±17.8 | 130±15.4 | |||
| ALP (IU/L) | 165±18.7 | 88 ±10.4 | |||
| ALBUMIN(g/dl) | 3.6 ±0.8 | 4.9±0.9 | |||
| GGT (IU/L) | 112±13.9 | 27.9±9.6 | |||
| INSULIN | 22.36±5.8 | 16±4.76 | |||
| URIC ACID(mg/dl) | 7.2±0.71 | 6.4±0.56 | |||
| hsCRP | 2. 7±0.42 | 0.8 ±0.03 | |||
| VITAMIN C | 0.7±0.25 | 1.8 ±0.82 | |||
| MDA(µmol/L) | 14.6±1.7 | 2.5 ±0.7 | |||
| ATHEROGENIC INDEX | 0.55±0.07 | 0.2±0.01 | |||
| HOMA- IR | 5.2±1.7 | 2.3±0.08 | |||
| BMI(kg/m2) | 30.8±2.4 | 23.9± 1.2 | |||
Serum GGT vs duration of alcohol intake
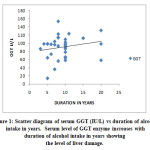 |
Figure 1: Scatter diagram of serum GGT (IU/L) vs duration of alcohol intake in years. Serum level of GGT enzyme increases with duration of alcohol intake in years showing the level of liver damage. |
Serum ALP (IU/L) vs TGL (mg/dl)
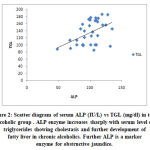 |
Figure 2: Scatter diagram of serum ALP (IU/L) vs TGL (mg/dl) in total alcoholic group . ALP enzyme increases sharply with serum level of triglycerides showing cholestasis and further development of fatty liver in chronic alcoholics. Further ALP is a marker enzyme for obstructive jaundice. |
Serum VIT C vs hsCRP
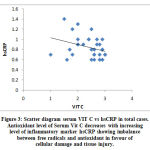 |
Figure 3: Scatter diagram serum VIT C vs hsCRP in total cases. Antioxidant level of Serum Vit C decreases with increasing level of inflammatory marker hsCRP showing imbalance between free radicals and antioxidant in favour of cellular damage and tissue injury. |
This study was conducted in a group of chronic alcoholics consuming alcohol for more than 10 years against a group of apparently normal healthy non alcoholic individuals. The mean age of cases and controls are 42.3 ± 4 and 39.5 ± 3.2 years and the mean duration of alcohol intake is 11.2 ± 2.8 years. Lipid profile in the study group has showed a much variations between the cases and control. The mean total cholesterol level (mg/dl) in cases was 232 ± 22.4 and in controls it was 168± 15.6. The mean HDL level (mg/dl) showed a significant variation among the study group as 38.8±7.8 and 55.7±8.6. The mean LDL and NHDL in cases were 148.6 ±15 and 170±17.8 respectively. The cardiac risk ratios TC:HDLc and LDLc:HDLc were also elevated in study populations when compared to controls with significant p value (<0.005). Calculated parameter of atherogenic index which is log10 (TGL/HD) showed that alcoholics have higher risk of developing atherogenesis leading to cardiac effect including the coronary artery disease when compared to the control group. (i.e. 0.55 ± 0.07 vs 0.2 ± 0.01). Normal level was being < 0.11 for low risk; < 0.24 for intermediate risk and > 0.24 for high risk [5].
The mean serum insulin level in study population was 22.36±5.8 and in controls was 16 ±4.76, showing increased risk of insulin resistance along with HOMA- IR 5.2 ±1.7 calculated by the formula: serum fasting glucose X serum insulin/405. Acute and chronic ethanol exposure leads to functional insulin resistance, measured as the inability of systemic insulin to suppress lipolysis and insulin-stimulated glucose uptake. Yet, paradoxically, ethanol also enhances hepatic insulin receptor phosphorylation and downstream protein kinase B signaling [6].
The Chronic alcoholic cases had increased BMI with grade 1 obesity with mean value of 30.8±2.4 whereas, the control group had mean value 23.9± 1.2.
Liver function tests were done for all the study populations. SGOT and SGPT enzymes were slightly elevated. Alkaline phosphatase enzyme was markedly elevated and there was significant correlation with increasing levels of triglycerides. Gamma Glutamyl Transferase (GGT) enzyme is from hepatocytic plasma membrame and it is widely accepted as biomarker for alcoholic liver disease. The GGT level was increased as expected with mean value 112±13.9. Serum albumin was decreased with mean value of 3.6±0.8 in cases and 4.9±0.9 in controls respectively indicating decreased synthetic function of liver cells.
The inflammatory markers and antioxidant status were studied in all the subjects and their results were as follows. Uric acid level was elevated than the normal level with mean value of 7.2± 0.71. Alcohol intake may also influence CHD risk through modulation of inflammatory parameters. Moderate alcohol intake is associated with decreased C-reactive protein (CRP) and leukocyte count, but there is an inverse association with heavy drinking .The principal source of CRP has been assumed to be the liver, but it has also been shown that arterial tissue itself produces CRP [7]. High sensitive C reactive Protein (hsCRP) inflammatory protein was significantly elevated with mean value 2.7±0.42 against control group with mean value of 0.8± 0.03. Results shows that alcohol misuse has a pro-inflammatory effect reflected by an increase in serum CRP level. We propose that through this effect, excessive ethanol consumption may result in increased oxidative stress leading to oxidation of LDL. Oxidised LDL (oLDL) results in the formation of atherosclerotic plaques by forming oxalyl radicals along with collagen, calcium debris making it insoluble fibrin [8]. The oLDL contains highly cytotoxic products such as aldehydes , hydroxyl radicles which are considered as diffusible toxins. MDA, 4 HNE and other lipid peroxidation products generated within LDL are believed to be responsible for free radicular damage of blood vessels and other cellular pathology. In normal cells there is appropriate balance between prooxidants and anti oxidants. But, dyslipidemia and lipid peroxidation may alter the balance in favour of atherogenesis. Lipid per oxidation marker MDA was markedly increased in alcoholics with mean value of 14.6± 1.7 while, controls had 2.5±0.7 with very significant p value 0.0024. Aqueous phase antioxidant vitamin C level was decreased in alcoholic patients when compared to control group with mean value of 0.7 ±0.25 and 1.8±0.82 with significant p value.
Conclusion
This study clearly proves the metabolic derangements in chronic alcoholics including dyslipidemia, increased oxidative stress and lipid per oxidation, atherogenesis, obesity and progressing hepatic damage. Though, every individual knows about the adverse effects of alcohol, the percentage of social drinking and in due course to binge drinking increases day by day among adolescents and middle aged population. Increased alcohol consumption at an early age may leads to the consequences earlier which results in decreasing the man power, working hours and in turn national productivity and its development. The oxidative stress factors, antioxidants level, BMI, lipid profile with cardiac risk ratio factors assessment should be done as a routine in assessing and managing alcoholics and during follow ups in order to prevent earlier complication.
Conflict of Interests
Declared None
Acknowledgement
We are thankful to the patients who had participated in this study.
Funding Source
This was conducted as a self funded project. Not received any fund or grant from others.
References
- Alcohol consumption – Indian statistics WHO report: google.com/amp/s/www.livermint.com/industry/Alcohol consumption in India has doubled in 11 years html% 3ffacet-amp.
- Neelesh Deshpande and Sabitha kandi. Effect of alcohol consumption on oxidative stress markers and its role in the pathogenesis and progression of liver cirrhosis. American journal of medical and biological research, 2013;1(4): 99-102 .
- Friedewald WT, Levy RI and Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem, 1972; 18(6):499-502.
- H Esterbauer ,G Wag and Puhl H. Lipid peroxidation and its role in atherosclerosis. British Medical bulletin, 1993; 49(3):566-576.
- Onat A, Can G, Kaya H and Hergenç G. Atherogenic index of plasma (log10 triglyceride/high-density lipoprotein- cholesterol) predicts high blood pressure, diabetes, and vascular events. J Clin Lipidol, 2010; 4(2):89-98.
- Claudia Lindtner, Thomas Scherer and Elizabeth Zielinski. Binge drinking induces whole-body insulin resistance by impairing hypothalamic insulin Action. Sci Transl Med, 2013 Jan 30; 5(170): 170-174.
- Hannu alho, Pekka silanaukee and Anne kalela. Alcohol misuse increases serum antibodies to oxidized LDL and C- reactive protein. Alcohol and Alcoholism, 2004; 39(4): 312–315 https://doi.org/10.1093/alcalc/agh059
- Vasudevan Sreekumari D M and Kannan Vaidyanathan S. Textbook of Biochemistry Seventh edition, Page No: 140-141.
- Stefano Volpato, Marco Pahor and Luigi Ferrucci. Relationship of Alcohol Intake with Inflammatory Markers and Plasminogen Activator Inhibitior-1 in Well-Functioning Older Adults- Tehe Health, Aging, and Body Composition Study. Aha Journals, 2004: http://circulation:ahajournals.org.
- Shanmugapriya V and Mohanty P K. Association between body mass index, lipid peroxidation and coronary lipid risk factors in hypothyroid subjects. International journal of medical science and public health, 2013; 2 (4): 1063-1067.

