
Manuscript accepted on :12 June 2018
Published online on: 28-06-2018
Plagiarism Check: Yes
Mirhakim Zh. Azizov1, Aziz P. Alimov1, Umida M. Rustamova2, Khurshid Kh. Shakirov1 and Nadezhda V. Stupina1
1Department of Adults Orthopedics Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics Mahtumkuli Str., Tashkent, Uzbekistan.
2Department of Rentgenology Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics Mahtumkuli Str., Tashkent, Uzbekistan.
Corresponding Author E-mail: niito-tashkent@yandex.ru
DOI : https://dx.doi.org/10.13005/bpj/1463
Abstract
Clinical and densitometric researches in patients with the terminal stage of gonarthrosis and decrease in bone mineral density allow determining the condition of knee joint endoprosthesis. In the process of research women took part; their average age made up 57 years (max. 84 years old, min. 52 years old – menopausal age). X-ray densitometry (dual energy absorptiometry) before and after surgery (in 12 months). Patients were divided into two (main and control) groups depending on further treatment schedule. Studying the treatment results was carried out using the method of criteria calculation – f* (Fisher) by the method of mathematical treatment. Densitometric data analysis before and after operation showed after operation in the main group of women, who took osteotropic drugs as compared to the indicators of control group, significant bone density increase. The growth in bone mineral density of the main group by the year end made up on the average 60%, in control group – 18,75%.
Keywords
Anti-inflammatory Agents; Bone Tissue; Degenerative Dystrophic Diseases; Gonarthrosis; X ray Destometry
Download this article as:| Copy the following to cite this article: Azizov M. Z, Alimov A. P, Rustamova U. M, Shakirov K. K, Stupina N. V. Analysis of Densitometric Indices of Osteotropic Therapy by the Method of f* (Fisher) in Case of Knee Arthroplasty. Biomed Pharmacol J 2018;11(2). |
| Copy the following to cite this URL: Azizov M. Z, Alimov A. P, Rustamova U. M, Shakirov K. K, Stupina N. V. Analysis of Densitometric Indices of Osteotropic Therapy by the Method of f* (Fisher) in Case of Knee Arthroplasty. Biomed Pharmacol J 2018;11(2). Available from: http://biomedpharmajournal.org/?p=21117 |
Introduction
Resorptive processes, taking place in near-prosthetic bone tissue, are considered most frequent causes of endoprosthesis instability component. Among the causes of check-up operations from 60% to 73,8% fall at the aseptic loosening of implant.1,2 The causes of such an early osteolysis after joint replacement to an artificial one, authors relate to insufficient physiological load on disease knee joint as a result of present flexion contractures of knee joint and taking non-steroid anti-inflammatory agents, which have a slowing down impact on the osteogenetic cells’ function.3,4,5 Remodeling of bone tissue is conjugated in time processes: full cycle of remodeling comprises of resorption activation, which is followed by bone formation activation. Osteolysis takes place when balanced relation between bone formation and resorption is upset. The mechanism of the increase in bone resorption and the decrease in its formation can be related to quantitative preponderance of functional osteoclasts compared with osteogenetic cells.6,7,8 Researches based on the X ray densitometry method demonstrate preponderance of osteolysis in early periods after endoprosthesis replacement of knee joint as compared to initial indices [5]. Under conditions of initial defect of bone tissue, given assident osteoporosis, the problem of instability becomes particularly exacerbated due to possible development of peroprosthetic microfractures.9,10 Therefore, pre-surgical medicated supporting of well-balanced flowing of the processes of osteolysis and remodelling in bone bed appears an important component of early and long-term prophylaxis of aseptic loosening of knee joint endoprosthesis components.11 Therefore, revealing early symptoms of osteolysis based on the X ray densitometry method and optimal medicated impact will allow preventing reabsorption after carried out knee arthroplasty. The purpose of our research was to study effectiveness of the impact of medicated correction on the processes of remodeling of bones forming knee joint before and after endoprosthesis replacement in a comparative aspect.
Materials and Methods
In the unit of adult orthopaedics of the R&D clinic of traumatology and orthopaedics from 2011 to 2014 66 patients were under indoor treatment with regard to degenerative dystrophic diseases, they were implanted endoprosthesis of knee joint De Puy pfs SIGMA with saving posterior cruciate ligament (24 endoprostheses) and without saving with posterior stabilizer (42 endoprostheses) according to standard technology. All patients were women, average age was 57 years (max. 84 years old, min. 52 years old). 38 patients suffered initial osteoarthrosis of the knee, 21 patients suffered rheumatoid arthritis, 7 patients – posttraumatic arthrosis of the knee joint. Terminal stage of gonarthrosis with limited joint movement was detected in all patients at the stage of pre-surgical examination.
31 patients undertook X ray densitometry (dual energy absorptiometry) before and after операции (in 12 months). Researches were carried out using the densitometric device Stratos (France) under standard programme: proximal section of the hip. Patients were divided into two groups depending on the schedule of further treatment. In the first (control) group general medicated treatment provided tasks of bone tissue normalization after surgical treatment from the 8th day within 12 months. Patients of the second group (main one) took osteotropic drugs (bisphosphonates, calcium drugs) within 6 months before surgical intervention and following 12 months after the implantation of knee joint endoprosthesis. The study of treatment results were carried out using the method of criteria calculation – f* (Fisher) by the method of mathematical treatment.12 An analysis of T-criterion was carried out by the data of dual energy X ray densitometry.
Results and Discussion
Densitometric researches of patients before surgery showed different values of T-criterion in the patients of control group from -1,0 to – 2,3; main group – from -0,8 to -2,9:
Basing on WHO recommendations, osteoporosis and osteopenia are diagnosed mainly by densitometric indices of T-criterion – the value of standard variations of T-criterion to -0,1 – N, from -1,0 – – 2,5 – osteopenia, – 2,5 and lower – osteoporosis (WHO, 1994). We considered the value T-score -1,0 a critical one and considered that if T-score is higher or equal to -1,0, than “there is an effect”, and if lower – 1,0, than “there’s no effect”. All preliminary figures are comparatively matched with data gotten after12 months. In the main group, the effect was observed in 9 out of 15, i.e. in 60% cases, and in the control group – in 3 out of 16, i.e. in 18,75% cases. These percentages can be compared by the f* method to determine authenticity of distinctions between them.
Н0: proportion of persons, whose T-score ≤1,0, in the main group is not higher than in the control group.
Н1: proportion of persons, whose T-score >1,0, in the main group is higher, than in the control group.
Let’s determine values of f*, corresponding to percentages of “effect” in each group based on the mathematical treatment method[12]:
ϕ* (60%)=1,775
ϕ* (18,75%)=0,897
Let’s calculate the empiric value of f* according to the formula:

where f1 – indicator corresponding to highest % rate;
f2 – indicator corresponding to lowest % rate;
n1 – number of observations in group 1;
n2 – number of observations in group 2.
In the given case:

According to Table XIII annex 1 E.V. we determine what level f*emp=2,434 corresponds to
Ρ=0,006
Now it’s possible to determine critical values of f*, corresponding to statistical significance levels:
f*cr= (2)
f*emp=2,434
f*emp˃f*cr
Let’s build “significance axis” (Fig. 1):
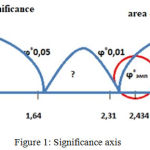 |
Figure 1: Significance axis
|
The f* empirical value obtained is the area of significance. As a result Н0 is rejected, Н1 is taken.
Conclusion
Densitometric analysis before surgery demonstrates a decrease in bone mineral density both in the main group and in the control group. After surgery in the main group of patients who took osteotropic preparations as compared to control group indicators, bone density significantly increased. During the analysis of treatment effectiveness of patients after endoprosthesis replacement of knee joint, statistically significant distinctions in 1 year were revealed in the process of remodeling in the main group. The growth of bone mineral density of the main group by the year end made on the average 60%, in the control group – 18,75%. In 40% of patients of main group, the results (Т-criterion is lower – 1,0) partially relate to concurrent conditions (rheumatoid arthritis, etc.).
References
- Kornilov N.V, Voytovitch A.V. et al., Surgical treatment of degenerative-dystrophic damage of large joints. Saint Petersburg. Lito Syntez. 1997;174–175.
- Small R, Ritter M.A, Merchun J.G, Davis K.E, Rogge R.D. Changes in tibial bone density measured from standard radiographs in cemented and uncemented total knee replacements after ten years’ follow-up. Bone Joint .J. 2013;95-B(7):911-916.
CrossRef - Rodionova S.S, Esykin N.A, Matveeva N.Y, Morozova N.S. Rational choice of treatment of initial phases of gonarthrosis in patients suffering systemic osteoporosis. Priorov Herald of traumatology and orthopaedics. 2014;2:52-56.
- Gilchrist N, Hooper G, Frampton C, Maguire P, Heard A, March R.L, Maxwell R, Penny I. Measurement of bone density around the Oxford medial compartment knee replacement using iDXA. A precision study. J. Clin Densitom. 2013;16(2):178-82.
CrossRef - Soininvaara T.A, Harju K.A, Miettinen H.J, Kröger H.P. Periprosthetic bone mineral density changes after unicondylar knee arthroplasty. Knee. 2013;20(2):120-7.
CrossRef - Berglezova M.A, Andreeva T.M. Aseptic loosening of pelvis joint endoprosthesis: mechanisms of osteolysis and potential therapy. Herald of traumatology and orthopaedics. 2010;3:82-88.
- Stilling M, Soballe K, Larsen K, Andersen N.T, Rahbek O. Knee flexion influences periprosthetic BMD measurement in the tibia. Suggestions for a reproducible clinical scan protocol. Acta Orthop. 2010;81(4):463-70.
CrossRef - Tjоrnild M, Sоballe K, Bender T, Stilling M. Reproducibility of BMD measurements in the prosthetic knee comparing knee-specific software to traditional DXA software: a clinical validation. J Clin Densitom. 2011;14(2):138-48.
CrossRef - Jensen C.L, Petersen M.M, Schrøder H.M, Lund B. Bone mineral density changes of the proximal tibia after revision total knee arthroplasty. A randomised study with the use of porous tantalum metaphyseal cones. Int Orthop. 2012;36(9):1857-1863.
CrossRef - Hooper G.J, Gilchrist N, Maxwell R, March R, Heard A, Frampton C. The effect of the Oxford uncemented medial compartment arthroplasty on the bone mineral density and content of the proximal tibia. Bone Joint J. 2013;95-B(11):1480-3
CrossRef - Jensen C.L, Petersen M.M, Schrоder H.M, Lund B. Changes in bone mineral density of the distal femur after revision total knee arthroplasty with metaphyseal press-fit stem. J Orthop Traumatol. 2010;11(3):143-8.
CrossRef - Sidirenko E.V. Methods of mathematical treatment in psychology, Saint Petersburg: Rech. 2003;349.

