
Nurul Syamimi Binti, Mohd Azlan Sunil and Ashish R. Jain
Department of Prosthodontics, Saveetha Dental College and Hospital, Saveetha University, Chennai, India.
Corresponding Author E-mail: dr.ashishjain_r@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1405
Abstract
The posterior palatal seal (PPS) is an important structure aiding in retention of maxillary complete denture. Failure to properly record it may lead to seal failure, decrease retention and physiological violation of palate. Proper methods and materials to record PPS should be used to achieve good retention of denture and patient’s comfort. To find out the most common methods and materials used for recording PPS among dental practitioners and dental students. 13 question questionnaire on knowledge, methods and materials to record PPS was prepared. 100 participants (50 dental practitioners, 50 dental students) from Saveetha Dental College, Saveetha University in Chennai was involved. The questionnaires were directly distributed and collected data was tabulated and analysed using Microsoft Excel 2013. 63% of participants correctly indicated pterygomaxillary seal and postpalatal seal as regions of PPS. 57% knew how to locate vibrating lines. 73% knew anterior vibrating line is cupids bow shape. 42% prefer arbitrary scraping, however, 64% indicated that it is the least accurate method. 49% and 44%, respectively, prefer IOWA wax and Korecta wax to record PPS. In a conventional technique, 73% prefer using ball-end of T-burnisher. 28% indicated butterfly shaped with notching of hamular notch as common form of PPS. 35% agreed that class 1 variation of PPS is the most common. 26% indicated the anterior vibrating line is 1.31mm distal to fovea palatine. 31% agreed lateral part of cupids bow has the highest compressibility. 45% indicated 5-12mm as anteroposterior width of PPS. The most preferred technique was arbitrary scraping. Most participants prefer IOWA wax and Korecta wax in case of fluid wax technique and flat-end part of T-burnisher is preferred in conventional technique. Results on knowledge of anatomical landmarks and parameter of PPS indicate that there is a need to emphasize on the importance of PPS with proper learning.
Keywords
Denture Retention; Knowledge on PPS; Materials to Record PPS; Methods of Recording PPS; PPS Survey
Download this article as:| Copy the following to cite this article: Binti N. S, Sunil M. A, Jain A. R. Knowledge, Attitude and Perception of Materials and Methods Used for Recording Posterior Palatal Seal Among Dental Practitioners and Dental Students. Biomed Pharmacol J 2018;11(1). |
| Copy the following to cite this URL: Binti N. S, Sunil M. A, Jain A. R. Knowledge, Knowledge, Attitude and Perception of Materials and Methods Used for Recording Posterior Palatal Seal Among Dental Practitioners and Dental Students. Biomed Pharmacol J 2018;11(1). Available from: http://biomedpharmajournal.org/?p=19507 |
Introduction
According to Glossary of Prosthodontics Terms, posterior palatal seal is the seal at the posterior border of a maxillary prosthesis. Posterior palatal seal area is the soft tissue area at or beyond the junction of the hard and soft palates on which pressure, within physiological limits, can be applied by a denture to aid in retention.1 The retention of the denture is a matter of great satisfaction to a dentist and more importantly, an utmost interest to the patient. A successful retention is achievable if the correct techniques and materials are put to use during treatment to fulfil the needs and expectations of the patient.
Patients expect a good prosthesis which can work efficiently during speech and mastication and be well-retained in the mouth for a long duration. Therefore, the importance of extension of complete dentures has been well-established for various reasons. The posterior palatal seal functions to provide retention and stability of a well-adapted denture through forces of adhesion, cohesion and interfacial surface tension by providing a proper seal, prevents food accumulation between posterior border of denture and soft palate, to reduce the tendency of gag, to make the sunken distal border of the denture less noticeable to the tongue, to supply a thickened area that provides added strength across the denture and to compensate for polymerization.2-4 Additional functions of posterior palatal seal which have been described by Weintraub 5 are increase in confidence and comfort to the patient by enhancing retention, provides a positive posterior contact and thus prevents the final impression material from sliding down into the pharynx. Although forces such as adhesion and cohesion, interfacial surface tension, capillary attraction and viscosity of the saliva may have been recognized to aid in retention of a denture, these forces are capable to resist only those forces that act perpendicular to the denture base. However, atmospheric pressure helps to counteract those tipping thrusts and lateral torque which tend to dislodge the denture. The displacement of the denture is prevented by a partial vacuum that is formed between the supporting tissues and the denture base that will resist lateral torque. Zurasky and Duke6 emphasized the fact that retention and stability obtained by adhesion and cohesion resist the forces, which are directed in vertical direction. A well-fitting and retentive complete denture requires a well-fitting tissue surface, a peripheral border compatible with the muscles and tissues which make up the mucobuccal and mucolabial spaces so that a peripheral seal is created by the soft tissue draping over them. It is usually obtained by labial and buccal seal. In the posterior region, it is mainly by the posterior palatal seal.7 At the posterior extension of the maxillary denture, where the tissues are less compliant, special attention is required to make the seal effective. This is the postdam region, where the denture is designed to affect a posterior palatal seal [8]. Skinner demonstrated experimentally the importance of posterior palatal seal and stated: “The most effective addition to increase retention is the post dam”.9 Despite the literature based recommendation regarding the relevance of posterior palatal seal in fabricating dentures, the location and preparation of it is frequently neglected by clinicians and dental students.10 Many dentures have failed due to improper establishment of distal limit and improper recording of posterior palatal seal. Recording posterior palatal seal without reference to the anatomical landmarks of the mouth may result is error of location and preparation on the master cast.
Various methods and materials to record posterior palatal seal and reproducing it in the maxillary denture have been introduced, such as the conventional technique, fluid wax technique, arbitrary technique, and extended palate technique.11 Classification of techniques of recording posterior palatal seal by Hardy and Kapoor 2 is divided in to three, which are functional, semi-functional and empirical technique. In the functional technique, the final impression is border molded in posterior palatal seal area with soft stick modelling compound or wax by sucking movements performed by the patient. As for semi-functional technique, border molding is done by the dentist itself and the cast is grooved to the desired depth in empirical technique. Each technique has its own advantages and disadvantages. Recording the posterior palatal seal is commonly performed by locating the posterior vibrating line in the patient’s mouth and transferring in to the master cast, followed by arbitrarily scribing the cast before fabricating the denture.12-16 Based on a previous study, 87.5% of dental schools in the Canada and United states implement arbitrary scribing to record posterior palatal seal on the cast,17 although arbitrary scribing of the master cast is considered to be the least reliable method.18 For the establishment of posterior palatal seal at final impression stage, the fluid wax technique is the technique of choice. Nevertheless, fluid wax technique19 comes with a few disadvantages such as more time is required for impression appointment, handling the materials may be difficult, a heating unit is needed for the purpose of wax conditioning, and boxing procedure of cast formation requires proper care to prevent ant distortion of the carefully added posterior palatal seal wax.
Choices of method to be used and timing depends on one’s preference and experience. Hence, this study aims to find out the most common methods and materials used for recording posterior palatal seal among dental practitioners and dental students.
Materials and Methods
An original pretested questionnaire on knowledge, attitude and perception of methods and materials to record posterior palatal seal was prepared. The questionnaire includes age of participants, gender and the year of study in case of student participants. The questionnaire consist of 13 questions regarding knowledge on anatomical landmarks and surrounding structures of posterior palatal seal, and perception and knowledge on methods and materials available to record posterior palatal seal. As seen in Figure 1, the sample size of this questionnaire-based study is 109 population. This study was conducted with 100 participants, thus, it is sufficient for the required sample size.
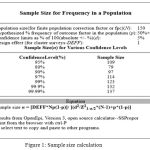 |
Figure 1: Sample size calculation
|
50 dental practitioners and 50 dental students were involved in the survey. Dental students were of third years, fourth years and interns and as for dental practitioners, the questionnaires were given at random to all faculties. Anatomical landmarks and surrounding structures of posterior palatal seal is of great importance when locating and recording the posterior palatal seal. Thus, questions regarding it were included in the survey to assess the participants’ knowledge on the structures and their priority towards it. The questionnaires were directly distributed to the participants and filled up questionnaires were immediately collected on site. The collected data was analysed and tabulated in Microsoft Excel 2013. All 100 participants responded to the survey, yielding a response rate of 100%. The subjects are between the ages of 20 to 46 years.
Table 1: Questionnaire on Knowledge, Attitude and Perception on Methods and Materials used for Recording Posterior Palatal Seal among Dental Practitioners and Dental Students.
| No. of Questions |
| 1. Based on anatomical landmark, which two regions make up the posterior palatal seal? |
| a) Hamular notch and postpalatal seal |
| b) Pterygomaxillary seal and postpalatal seal |
| c) Maxillary tuberosity and postpalatal seal |
| d) Pterygomaxillary seal and maxillary tuberosity |
| 2. Are you aware of how to locate the anterior and posterior vibrating line? |
| a) Yes |
| b) No |
| 3. What is the shape of anterior vibrating line? |
| a) Butterfly-shaped c) Cupid’s bow shaped |
| b) Oval-shaped d) Triangular-shaped |
| 4. While recording posterior palatal seal, should PPS extend in to mid palatine fissure if it is present? |
| a) Yes |
| b) No |
| 5. Which techniques do you prefer to use when recording the PPS? |
| a) Conventional technique d) Extended palate technique (Silverman) |
| b) Fluid wax technique e) Adding PPS to extending denture |
| c) Arbitrary scraping of master cast f) Others: |
| 6. Among the four techniques stated below, which is the least accurate method to mark the posterior palatal seal? |
| a) Conventional technique c) Arbitrary scraping |
| b) Fluid wax technique d) Extended palate technique (Silverman) |
| 7. Which material do you prefer to use when recording PPS with fluid wax technique? |
| a) Iowa wax c) Adaptol |
| b) Korecta wac d) H-L physiologic paste |
| 8. Which part of the T-burnisher do you prefer to use when recording PPS with conventional technique? |
| a) Ball-end c) Handle end |
| b) Flat-end |
| 9. Out of various forms of posterior palatal seal which is more common? |
| a) Single bead scribed on the posterior vibrating line |
| b) Double line scribed in the anterior and posterior vibrating line |
| c) Butterfly shaped posterior palatal seal |
| d) Butterfly shaped posterior palatal seal with notching of posterior vibrating line |
| e) Butterfly shaped posterior palatal seal with notching of hamular notch. |
| 10. Most common Variations used with different shaped soft palate based on the classification. |
| a) Class 1: A butterfly shaped posterior palatal seal with 3-4 mm wide |
| b) Class 2: Posterior palatal seal is narrow with 2-3 mm of width |
| c) Class 3: A single beading made on the posterior vibrating line |
| 11. Location of posterior palatal seal is not consistent and show lot of variation but on an average anterior vibrating line is ——-mm distal to fovea palatine. |
| a) 1.31mm c) 1.57mm |
| b) 1.39mm d) 2.1mm |
| 12. Which part of posterior palatal seal has highest compressibility? |
| a) Midpalatine raphe c) Lateral part of cupids bow |
| b) Hamular notch d) All of the above |
| 13. Anteroposterior width of posterior palatal seal is |
| a) 5-12mm c) 10-12mm |
| b) 8-10mm d) less than 5mm |
Results
A total of 100 dental practitioners and dental students from Saveetha Dental College participated in this study. The response rate of participants was 100%. Among 100 participants, 58 of them were female (27-practitioners, 31-students) and 42 were male (23-practitioners, 19-students) participants, aged between 20 to 46 years. Out of 50 dental students, 21 (42%) of them are interns, 18 (36%) are in their fourth year and the remaining 11 (22%) are third year students. The results were gathered through the questionnaires and they are as followed.
As seen in Figure 2, 63% of the participants correctly indicated that the pterygomaxillary seal and postpalatal seal are two regions which make up the posterior palatal seal, whereas 24% answered ‘hamular notch and postpalatal seal’, 9% chose ‘maxillary tuberosity and postpalatal seal’ and remaining 4% went with ‘pterygomaxillary seal and maxillary tuberosity’.
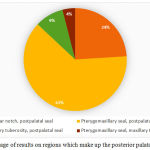 |
Figure 2: Percentage of results on regions which make up the posterior palatal seal
|
The participants were asked if they were are on how to locate the anterior and posterior vibrating line. As seen in Figure 3, over half of the participants surveyed (57%) were aware on how to locate the anterior and posterior vibrating line while 43% reported not being aware of it.
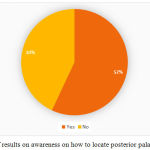 |
Figure 3: Percentage of results on awareness on how to locate posterior palatal seal
|
When asked about the shape of anterior vibrating line, as seen in Figure 4, nearly four fifth of the participants (73%) were aware of the shape of anterior vibrating line and correctly indicated cupid’s bow shape, however, 21% went with butterfly shape and 6% went with oval shape. None of the participants chose triangular shape as their answer.
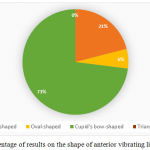 |
Figure 4: Percentage of results on the shape of anterior vibrating line
|
The participants were asked whether or not the posterior palatal seal should extend in to the mid palatine fissure while recording the posterior palatal seal if it is present. Figure 5 shows that 81% agreed that the posterior palatal seal should be extended in to the mid palatine fissure if it is present and the remaining 19% decided the opposite.
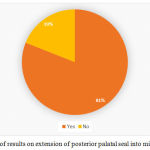 |
Figure 5: Percentage of results on extension of posterior palatal seal into mid palatine fissure
|
As shown in Figure 6, almost half of the participants surveyed (42%) reported arbitrary scraping technique as preferred technique, 25% prefer fluid wax technique to record posterior palatal seal, 21% would use conventional technique, and only 7% and 5%, respectively, would prefer to use extended palate technique (Silverman technique) and adding posterior palatal seal to extending denture.
 |
Figure 6: Percentage of results preferred techniques to record posterior palatal seal
|
As shown in Figure 7, among the four techniques – conventional technique, fluid wax technique, arbitrary scraping technique and extended palate technique (Silverman technique), arbitrary scraping technique was indicated as the least accurate method to mark posterior palatal seal by a majority of the participants (64%) while 19% and 12% went with fluid wax technique and conventional technique respectively as least accurate method and the remaining 5% reported extended palate technique.
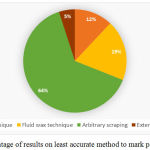 |
Figure 7 : Percentage of results on least accurate method to mark posterior palatal seal
|
When asked on which materials they prefer to use when using fluid wax technique, as seen in Figure 8, 44% of participants prefer to use Korecta wax when recording posterior palatal seal by fluid wax technique. IOWA wax is preferred by 49% of participants, 7% selected adaptol and none prefer to use H-L physiologic paste.
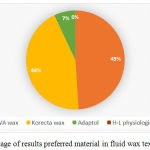 |
Figure 8: Percentage of results preferred material in fluid wax texhnique
|
The participants were asked on which part of the T-burnisher to they prefer to use when recording posterior palatal seal with conventional technique. As seen in Figure 9, most of the participants (73%) prefer to use the flat-end of t-burnisher and only 27% prefer the ball-end.
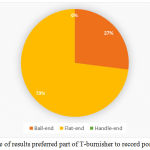 |
Figure 9: Percentage of results preferred part of T-burnisher to record posterior palatal seal
|
Participants were asked on the most common form posterior palatal seal, in which as seen in Figure 10, 32% of participants reported ‘butterfly shape’ as most common form of posterior palatal seal, whereas 18% and 14%, respectively, answered ‘double line scribed in the anterior and posterior vibrating line’ and ‘butterfly shape with notching of posterior vibrating line’. 8% answered ‘single bead scribed on the posterior vibrating line’. However, only 28% of the participants correctly indicated that the butterfly shaped posterior palatal seal with notching of hamular notch is the most common form of posterior palatal seal.
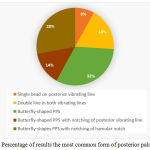 |
Figure 10: Percentage of results the most common form of posterior palatal seal
|
Figure 11 shows over half of the participants (52%) answered ‘Class 2: Posterior palatal seal is narrow with 2-3mm of width’ as the common variation used with different shaped soft palate based on the classification. Only 35% responded with ‘Class 1: A butterfly shaped posterior palatal seal with 3-4mm wide’ and the rest of the participants (13%) went with ‘Class 3: A single beading made on the posterior vibrating line’.
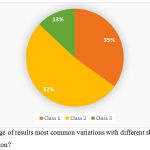 |
Figure 11: Percentage of results most common variations with different shaped soft palate based on classification?
|
The participants were asked on the average distance of anterior vibrating line to fovea palatine. Figure 12 shows option (b) and (c) (1.39mm and 1.57mm respectively) had an equal response of 31% of the participants, 26% responded ‘1.31mm’ and 12% answered ’2.1mm’ distal to fovea palatine.
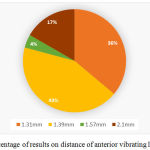 |
Figure 12: Percentage of results on distance of anterior vibrating line to fovea palatine
|
As seen in Figure 13, 36% indicated that hamular notch is the part of posterior palatal seal with highest compressibility, 20% responded with option (a)-mid palatine raphe, 31% of the participants correctly answered ‘lateral part of cupids bow’ and few of them (13%) went with option (d)-all of the above.
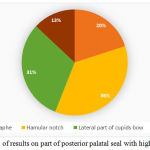 |
Figure 13: Percentage of results on part of posterior palatal seal with highest compressibility
|
Figure 14 shows less than half the participants surveyed (45%) agreed on 5-12mm as the anteroposterior width of posterior palatal seal, around two fifth of the participants (31%) responded ‘8-10mm’, 6% answered ’10-12mm’ and 18% responded with ‘less than 5mm’.
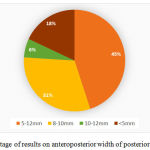 |
Figure 14: Percentage of results on anteroposterior width of posterior palatal seal
|
Discussion
The results of this survey of show that most of the participants do possess knowledge on the anatomical landmarks and surrounding structures of posterior palatal seal. However, most of them do not possess knowledge on parameters of posterior palatal seal such as size, shape, location and compressibility. The materials and methods used to record posterior palatal seal vary among them. Most of the participants had knowledge on the regions which make up the posterior palatal seal, which is the pterygomaxillary seal and post palatal seal. Pterygomaxillary seal extends through pterygomaxillary notch continuing 3-4 mm anterolaterally, approximating the mucogingival junction. 1 Hardy and Kapur 2 mentioned that it occupies the entire width of hamular notch which is covered by pterygomaxillary fold. The postpalatal seal is the area between the anterior and posterior vibrating line found medially from one tuberosity to other and appears as a cupids bow, which in correctly indicated by 73% of the participants. Over half of the participants (5%) were aware on how to locate the anterior and posterior vibrating line, although it has been thought in second year and in depth during the fourth year of study. According to Sear, the anterior vibrating line is not the junction of hard and soft palate. However, according to Gerald S. Wintraub, it is usually located in the junction of soft and hard palate. 5 Based on a previous study by Rashedi, B., & Petropoulos, V. C. (2003),20 most dental schools in the US (80%) teach a combination of phonation of the “ah” sound with other method such as blowing the nose and using fovea palatine as a guide, in locating posterior vibrating line. In order to achieve obtain acceptable stability and retention of denture, the denture should be perfectly adapted and proper seal should be established.2 A satisfying majority of participants (81%) do know while recording posterior palatal seal, it should extend into the mid palatine fissure if it is present. This is to provide a good peripheral seal. 3
Less than half of the participants (42%) prefer to use arbitrary scraping technique to record posterior palatal seal, although it is the least accurate technique as it has high potential of over postdamming and it is not physiologic.21 64% of the participants were aware of the inaccuracy of arbitrary scraping technique. Similarly, a previous study by Chen et al., reported most dental schools in the United States and Canada (87.5%) teach arbitrary scribing of master cast although they are aware arbitrary scribing of mater cast is considered by some to be the least accurate method and leaves a chance at insertion appoint since it relies of dentist’s recollection of palatal configuration and tissue compressibility.22 21% of participants prefer conventional, and 25% prefer to use fluid wax technique. Based on a literature review, conventional technique provides a highly retentive trial base, gives psychological security to patient that retention will not be a problem, dentist is able to understand the retentive qualities of final denture, and the posterior extension of the denture can be understood by the patient, but, it has more potential for over compression of tissue and not a physiological technique.10 However, fluid wax technique avoids over compression of tissue and it is a physiological technique besides increasing retention at an early stage by incorporating posterior palatal seal into trial denture base.10 Others would prefer extended palate technique (7%) and another technique which is adding posterior palatal seal to extending denture (5%). Fluid wax technique uses waxes that have low melting point for ease of use intraorally without discomfort or trauma to the patient, low distortion and rigidity at room temperature, high flow rate at mouth temperature (98.6°F), smooth texture and ease of adding additional layers without demarcation and hardens readily when chilled. 7,11 Impression waxes used in fluid wax technique are IOWA wax developed by Dr. Earl S. Smith, Korecta wax no. 4 by Dr. O. C. Applegate, H-L physiologic paste by Dr. C.S. Howkins and adaptol by Dr. Nathen G. Kyne. Korecta wax and IOWA wax were preferred by 44% and 49% of the participants respectively, and only 7% preferred adaptol.
A study by Lye 11 in 100 randomly selected subjects found the fovea palatine were posterior to the vibrating line in 13% of the cases, 17% coincide with it and 70% lay anterior to it. Location of posterior palatal seal is not consistent and show lot of variation but on an average anterior vibrating line is 1.31 mm distal to fovea palatine.23 Only 26% of the participants correctly indicated the location of vibrating line to fovea palatine. A lot of variation has been found in the posterior palatal seal area. Midpalatal raphe and hamular notch has been observed to have low compressibility. Lateral part of cupids bow has been observed as having the highest compressibility, which is correctly responded by 31% of the participants. With regards to size, only 45% indicated the anteroposterior width of posterior palatal seal is 5-12mm. On an average, the dimension of posterior palatal seal was 2mm at the midpalatal region and hamular notch, which was claimed by Hardy and Kapur. 2 A previous study performed by Silverman evaluated the posterior palatal seal clinically, histologically and radiographically, and he found that 8.0mm (with range of 5-12mm) is the greatest mean anteroposterior width of posterior palatal seal [21]. This indicates that the participants had poor knowledge on parameters of posterior palatal seal such as location, size, shape and compressibility. Clinicians should appreciate that the shape and dimension of posterior palatal seal cannot be only arbitrarily made on edentulous cast because it needs to be physiologically compatible with the tissues at rest and during function. A previous study observed that dental students have an intermediate level of confidence in selecting various techniques available for recording posterior palatal seal.24 Students need to be taught that recording posterior palatal seal is a clinical procedure and should not be ignored and delegate the task to laboratory technicians. As mentions by Laney and Gonzalez,25 to assign the laboratory technician this responsibility is a breach of the patient’s faith in the diagnostic ability of the dentist.
Conclusion
The finding of this survey showed that the preferred materials and methods to record posterior palatal seal vary among them but one technique which was mostly preferred was the arbitrary scraping technique. Most of them had common preference on materials to be used. The participants have an acceptable knowledge on anatomical landmarks and surrounding structures of posterior palatal seal. However, knowledge on specific parameters such as size, shape, location and compressibility was poor. This indicates that there is a need to emphasize on the importance of posterior palatal seal with proper learning as it plays an important role in complete denture stability and retention and patient’s satisfaction. Without knowledge on posterior palatal seal, there will be an increase chance of errors that will affect the success of a complete denture prostheses and patient’s satisfaction.
References
- The Glossary of Prosthodontic Terms 8th. J Prosthet Dent. 2005;95:10-81.
- Hardy I. R., Kapur K. K. Posterior border seal—its rationale and importance. Journal of Prosthetic Dentistry. 1958;8(3):386-97.|
CrossRef - Nallaswamy D. Textbook of prosthodontics. 2nd Jaypee Brothers Medical Publishers (P) Ltd. 2017.
- Bindhoo Y. A., Thirumurthy V. R., Jacob S. J. Posterior Palatal Seal: A Literature Review. International Journal of Prosthodontics and Restorative Dentistry. 2011;1(2):108-14.
CrossRef - Weintraub G. S. Establishing the posterior palatal seal during the final impression procedure: a functional approach. The Journal of the American Dental Association. 197;94(3):505-10.
CrossRef - Zurasky J. E., Duke E. S. Improved adhesion of denture acrylic resins to base metal alloys. Journal of Prosthetic Dentistry. 1987;57(4):520-4.
CrossRef - Ettinger R. L., Scandrett F. R. The posterior palatal seal. A review. Australian Dental Journal. 1980;25:197-200.
CrossRef - Schwarz W. D. The post dam. Dental Update. 1991;18:26-30.
- Skinner E. W., Campbell R. L., Chung P. A clinical study of the forces required to dislodge maxillary denture bases of various designs. The Journal of the American Dental Association. 1953;47(6):671-80.
CrossRef - Goyal S., Goyal M. K., Balkrishanan D., Hegde V., Narayana A. I. The posterior palatal seal: Its rationale and importance: An overview. European Journal of Prosthodontics. 2014;2(2):41.
CrossRef - Lye T. L. The significance of the fovea palatini in complete denture prosthodontics. Journal of Prosthetic Dentistry. 1975;33(5):504-10.
CrossRef - Avant W. E. A study of some factors associated with denture retention. The Journal of prosthetic dentistry. 1973;29(4):383-9.
CrossRef - Maison W. G. Denture outline form. The Journal of the American Dental Association. 1959;59(5):938-43.
CrossRef - Hicky J. C., Zarb G. A., Bolender C. L. Boucher’s prosthodontic: treatment for edentulous patient. 8th ed. St. Louis: Mosby publishers. 1980:411-5.
- Naylor W. P., Stephens V. A. Location and transfer of the vibrating line clinical and laboratory techniques. Quintessence of dental technology. 1986;10(9):557.
- Naylor W. P., Rempala J. D. The posterior palatal seal–its forms and functions (II)–Design and cast preparation. Quintessence of dental technology. 1986;10(8):489-92.
- Chen M. S., Welker W. A., Pulskamp F. E., Crosthwaite H. J., Tanquist R. A. Methods taught in dental schools for determining the posterior palatal seal region. Journal of Prosthetic Dentistry. 1985;53(3):380-3.
CrossRef - Winkler S., editor. Essentials of complete denture prosthodontics. 2nd Year Book Medical Publishers. 1988:119.
- Winkler S. Essentials of complete denture prosthodontics. WB Saunders Company. 1979:183-90.
- Rashedi B., Petropoulos V. C. Current concepts for determining the postpalatal seal in complete dentures. Journal of Prosthodontics. 2003;12(4):265-70.
CrossRef - Winkler S. Essentials of complete denture prosthodontics. WB Saunders Company. 1979:171-92.
- Chen M. S., Welker W. A., Pulskamp F. E., Crosthwaite H. J., Tanquist R. A. Methods taught in dental schools for determining the posterior palatal seal region. Journal of Prosthetic Dentistry. 1985;53(3):380-3.
CrossRef - Silverman S. I. Dimensions and displacement patterns of the posterior palatal seal. Journal of Prosthetic Dentistry. 1971;25(5):470-88.
CrossRef - Swathy S., Ashish R. J. Knowledge and Self Perception among Dental Students (Interns) about Procedures Involved in Complete Denture Fabrication. The Journal of Pharmaceutical Sciences and Research. 2017;9(5):708-11.
- Laney W. R., Gonzalez J. B. The maxillary denture: its palatal relief and posterior palatal seal. The Journal of the American Dental Association. 1967;75(5):1182-7.
CrossRef

