
Manuscript accepted on :
Published online on: 08-01-2016
Plagiarism Check: Yes
Karthick1, K. M. K. Masthan2, N. Aravindha Babu3, R. Jayasri Krupaa4, N. Anitha5
1Post Graduate Student, Department Of Oral Pathology and Microbiology, SreeBalaji Dental College and Hospital, Bharath University, Chennai. 2Professor and Head Of The Department, Department Of Oral Pathology and Microbiology, SreeBalaji Dental College and Hospital, Bharath University, Chennai. 3Professor, Department of Oral Pathology and Microbiology, Sree Balaji Dental College and Hospital, Bharath University , Chennai. 4Senior Lecturer, Department Of Oral Pathology and Microbiology, Sree Balaji Dental College and Hospital, Bharath University , Chennai. 5Senior Lecturer, Department Of Oral Pathology and Microbiology, Sree Balaji Dental College and Hospital, Bharath University , Chennai
DOI : https://dx.doi.org/10.13005/bpj/714
Abstract
Dermatoglyphics, a branch of physical anthropology, medicine and genetics refers to study of the intricate dermal ridge configurations on the skin covering the palmar and plantar surfaces of hand and feet. Dermatoglyphic patterns remain unchanged from birth to death and genetically determined, hence considered as an ideal marker for individual identification and the study of populations. Also used for detection of defects due to intra-uterine irregularities in the early weeks of pregnancy. Dermatoglyphics is considered as a window of congenital and intrauterine abnormalities. Several researches claim dermatoglyphics as an important diagnostic tool for some diseases especially the diseases with obscure etiology and mysterious pathogenesis. This paper aims to present the dermatoglyphic pattern configuration and methods for recording dermatoglyphics.
Keywords
Dermatoglyphics; Fingerprints; Palmar prints; Arch; Whorl; Loop
Download this article as:| Copy the following to cite this article: Karthick, Masthan K. M .K, Babu N. A, Krupaa R. J, Anitha N. Dermatoglyphics -A Review. Biomed Pharmacol J 2015;8(October Spl Edition) |
| Copy the following to cite this URL: Karthick, Masthan K. M .K, Babu N. A, Krupaa R. J, Anitha N. Dermatoglyphics -A Review. Biomed Pharmacol J 2015;8(October Spl Edition). Available from: http://biomedpharmajournal.org/?p=3748> |
Introduction
Since the early days of civilization, the features of the hands have fascinated scholars, doctors, and laymen alike. Through decades of scientific research, the hand has come to be recognized as a powerful tool in the diagnosis of psychological, medical, and genetic conditions. Cummins in 1926 first introduced the term “dermatoglyphics” which refers to the study of the naturally occurring patterns of the surface of the hands and feet. Since then, this approach has been used in various scientific studies to establish relationship of fingerprints as genetic and/or chronic health markers.1
The word ‘dermatoglyphics’ comes from two Greek words (derma, skin and glyphe, carve) and refers to the epidermal skin ridge formations which appear on the fingers, palms of the hands and soles of the feet.2 This term was coined by Harold Cummins in 1926. It is known that finger and palm prints are formed during the 6-7th week of the embryonic period and are completed after 10-20 weeks of gestation.3 Genetic process of dermatoglyphic traits is complex and is not perfectly known.2 Their variable characteristics are not duplicated in other people, even in monozygotic twins or even in the same person, from location to location.4 Abnormalities in these areas are influenced by a combination of hereditary and environmental factors, but only when the combined factors exceed a certain level, can these abnormalities be expected to appear.5
At present, several researches claim this study of dermatoglyphics as an important diagnostic tool for some diseases especially the diseases with obscure etiology and mysterious pathogenesis. Significant investigations have also been carried out into the dermatoglyphic indicators of Down’s syndrome, Trisomy 18, D trisomy, cat cry syndrome, Turner’s syndrome, Klinefelter’s syndrome, congenital heart disease, leukemia, cancer, celiac disease, intestinal disorders, rubella, rheumatoid arthritis, bronchial asthma, Alzheimer’s disease, schizophrenia as well as other forms of mental illness. Diagnosis of Diabetes Mellitus, Schizophrenia, hypertension, etc. can now be aided by dermatoglyphic analysis.6 In dentistry, dermatoglyphics have been studied to help predict disorders like cleft lip and cleft palate, dental caries, malocclusion, congenital anomalies like ectodermal dysplasia, gingival fibromatosis, periodontitis, bruxisium etc.1
Dermatoglyphic Pattern Configuration7
1Dermatoglyphic landmarks
The three basic dermatoglyphic landmarks found on the fingertip patterns are tri-radii, cores and radiants.
i) Tri-radius: It is formed by the confluence of three ridge systems that form angles of approximately 120o with one another.
ii) Core: It is in the approximate centre of the pattern.
iii) Radiant: They emanate from the tri-radius and enclose the pattern area.
2Fingertip patterns
The ridge patterns on the distal phalanges of the fingertips are divided into the three groups: arches, loops, and whorls.
i) Arches: It is the simplest pattern found on fingertips. It is formed by succession of more or less parallel ridges, which traverse the pattern area and form a curve that is concave proximally (Figure Sometimes, the curve is gentle; at other times it swings more sharply so that it may also be designated as a low or high arch respectively. The arch pattern is subdivided into two types:
a) Simple or plain arch composed of ridges that cross the fingertip from one side to the other without recurving.
b) Tented arch composed of ridges that meet at a point so that their smooth sweep is interrupted.
ii) Loops: It is the most common pattern on the fingertip. A series of ridges enter the pattern area on one side of the digit, recurve abruptly, and leave the pattern area on the same side (Figure 2). The loop pattern is subdivided into two types:
a) Ulnar loop composed of ridges that open on the ulnar side.
b) Radial loop composed of ridges that open on the radial side.
Loops may vary considerably in shape and size. They may be large or small, tailor short, vertically or horizontally oriented, plain loop or double loop. Occasionally, transitional loops can be found which resemble whorls or complex patterns.
iii) Whorls: It is any ridge configuration with two or more tri-radii. One tri-radius is on radial and the other on the ulnar side of the pattern (Figure 3). Subtypes of whorl patterns include:
a) Plain/simple/concentric whorl composed of ridges that are commonly arranged as a succession of concentric rings or ellipses.
b) Spiral whorl is a configuration in which ridges spiral around the core in either a clockwise or a counter clockwise direction.
c) Central pocket whorl is a pattern containing a loop within which a smaller whorl is located. Central pockets are classified as ulnar or radial according to the side on which the outer loop opens.
d) Lateral pocket/twinned loop pattern is composed of interlocking loops.
e) Accidentals/complex patterns are one in which patterns cannot be classified as one of the above patterns.
Some represent a combination of two or more configurations such as a loop and a whorl, triple loops and other unusual formations.
3Palmar patterns
The palm has been divided into several anatomically designed areas and includes thenar areas; four inter-digital areas, and the hypothenar area (Figure 4).
i) Thenar and first inter-digital area: These two areas are closely related anatomically and are considered one area. Patterns, when present, are most often loops.
ii) Second, third and fourth inter-digital area: Configurations encountered in the inter-digital regions are loops, whorls, vestiges and open fields.
iii) Hypothenar area: Patterns commonly seen are whorls, loops and tented arches.
4Quantitative analysis
Many dermatoglyphic characteristics can be described quantitatively, e.g. by ridge counting, and measuring distances or angles between specified points.
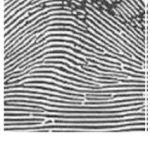 |
Figure 1: Arches |
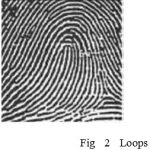 |
Figure 2: Loops |
 |
Figure 3: Whorls |
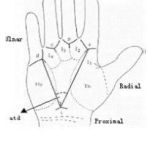 |
Figure 4: Palm patterns |
Methods of Recording Dermatoglyphics
Reviewing the literature one can find number of methods for recording dermatoglyphics. Variability lies in their requirements for equipment, time and experience, and in the quality of the prints produced.
The various methods that can be employed are: 7
i) Ink method,
ii) Inkless method,
iii) Transparent adhesive tape method, and
iv)Photographic method.
The most common method used for dermatoglyphic studies is the ink method first described by Cummins and Midlow (1943). Other methods have been tried which include a ‘Scotch-tape India-ink’ method which is an inkless method using sensitizing fluid, adhesive tape, powder, and carbon paper. Recent “hi-tech” methods are generally computer based and begin by scanning prints with a video camera followed by digitizing the print features which are then subjected to analysis. Okajima (1975) developed a method to study ridges on the dermal surface instead of the epidermal surface using chemical treatment and staining with toluidine blue that can be done even in fetuses from the 14th gestational week. Misumi et al (1984) used scanning electron microscope. Others have used Rubber and Plaster of Paris casts also. These methods are costly or cumbersome.
The lipstick method is easy, harmless, cheap, subject and user friendly and a single person can do the procedure alone too. The chemical composition of lipstick varies greatly from brand to brand. A typical lipstick has the following composition: dye, 5%; titanium dioxide 10%; oil 40%; wax 20%; emollient 25%, with traces of other components to impart a pleasant odor, a preservative to kill microbes, vitamin E, sunscreens and sometimes even a flavoring agent. Commonly used dyes are 4′, 5′-dibromo-fluorescein and 2′, 4′, 5′, 7′-tetrabromo-fluorescein, which is also known as eosin. Forensic science also recognizes ‘Cheiloscopy’, which is the study of lip prints.8
Advantages
The major advantages of the dermatoglyphics are:9
i) They are fully developed at birth and thereafter remain unchanged for life.
ii) Scanning or recording of their permanent impressions can be accomplished rapidly, inexpensively, conveniently and without causing any trauma to the patient or hospitalization.
Conclusion
It is important that methods to be developed to identify the person who are either at risk or already have a given illness in the most cost‑efficient manner without compromising quality of care. The use of dermatoglyphics is a rather unique approach and cost effective for identification in such individuals. Health care professionals, dental professionals and researchers should adopt this approach of dermatoglyphics for an early diagnosis, treatment and better prevention of many genetic disorders and other diseases whose aetiology may be influenced directly or indirectly by genetic inheritance.
References
- Ambika Gupta and Freny R Karjodkar: Role of dermatoglyphics as an indicator of precancerous and cancerous lesions of the oral cavity. Contemp Clin Dent. 2013 Oct-Dec; 4(4): 448–453.
- Namdeo Prabhu, Rakhi Issrani, Saurabh Mathur, Gaurav Mishra, Shruti Sinha: Dermatoglyphics in Health and Diseases-A Review.J Res Adv Dent 2014; 3:2:20-26.
- Gh. Mohd. Bhat, M. Arif Mukhdoomi, Bahir Ahmed Shah, Mohd Saleem Ittoo. Dermatoglyphics: in health and disease – A review. International Journal of Research in Medical Sciences 2014;2(1):31-37.
- Rokaya H. Ahmed, Mohammed I. Aref , Rania M. Hassan, Noura R. Mohammed. Dental fillings and its correlation to apoptosis that induced by using dental fillings. Nature and Science 2010;8(10):54-57.
- Natekar PE, DeSouza FM. Fluctuating asymmetry in dermatoglyphics of carcinoma of breast. Indian J Hum Genet 2006;12:76-81.
- Tamgire D W, Fulzele R R, Chimurkar V K, Rawlani S S and Sherke A R: Quantitative dermatoglyphic analysis in patients of oral sub mucousfibrosis. IJBR (2013) 04 (06).
- Pratibha Ramani, Abhilash PR, Herald J Sherlin, Anuja N, Priya Premkumar Chandrasekar, G.Sentamilselvi, V.R. Janaki. Conventional Dermatoglyphics–Revived Concept: A Review. International Journal of Pharma and Bio Sciences 2011; 2(3):446-458.
- Roopam K Gupta, Aruna K Gupta. New, easy and effective method to take dermatoglyphic prints. National Journal of Medical Research 2013;3(1):45-47.
- Kiran. K , Kavitha Rai, Amitha M Hegde. Dermatoglyphics as a noninvasive diagnostic tool in predicting mental retardation. Journal of International Oral Health 2010;2(1):95-100.

