
Manuscript accepted on :August 05, 2016
Published online on: 27-08-2016
Plagiarism Check: Yes
L. Leelavathi1, R. Karthick2*, S. Leena Sankari1* and N. Aravindha Babu1*
1Department of Public Health Dentistry, Tagore Dental College and Hospital, Rathinamangalam, Vandalur post, Chennai - 600107.
2Dept of Oral Pathology, Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, Chennai-600100.
DOI : https://dx.doi.org/10.13005/bpj/1015
Abstract
Avulsion of permanent teeth is one of the most serious dentalinjuries, and a prompt and correct emergency management is very importantfor the prognosis.Tooth avulsion or exarticulation is a traumatic injury of dental tissue characterised by complete displacement of the tooth out of its socket. Successful treatment outcome of such an injury is dependent on the survival of the viable periodontal ligament cells attached to the tooth root surface. The viability of the periodontal ligament cells is best preserved either when the tooth is immediately replanted into its socket or if it is stored in an appropriate storage /transport medium till a time, the tooth can be replanted into its socket.
Keywords
Trauma; Storage media; Transport media; Avulsion
Download this article as:| Copy the following to cite this article: Leelavathi L, Karthick R, Sankari S. L, Babu N. A. Avulsed Tooth - A Review. Biomed Pharmacol J 2016;9(2). |
| Copy the following to cite this URL: Leelavathi L, Karthick R, Sankari S. L, Babu N. A. Avulsed Tooth - A Review. Biomed Pharmacol J 2016;9(2). Available from: http://biomedpharmajournal.org/?p=8159 |
Introduction
Avulsion is the totaldislodgement of an intacttooth from its socket.According to Andreasen andAndreasen, avulsion ofpermanent teeth accounts forapproximately 0.5–3% of alldental trauma. The peak agefor avulsion is between 7 to 9years and mainly involvesmaxillary anteriors. Losing ananterior tooth at an young agemay have severe psychologicalconsequences. The immediatereplantation of a permanentavulsed tooth is essential torestore the function andesthetics and critical for longterm success of the treatment.Avulsion presents a challengewith regard to its properemergency management. Theprincipal challenge is tomaintain the vitality ofperiodontal cells, as prognosisof a replanted tooth is directlyproportional to the viableperiodontal cells. Use ofphysiological storage medialike milk, saliva or saline iscritical to maintain the viabilityof periodontal cells untilprofessional help is obtained.1
Tooth avulsion mainlyoccurs during sports, physical violence, road traffic accidents, fall and other physicalimpacts. Many patients withavulsed tooth visit medicaldoctors due to lack ofawareness or unavailability ofa dentist.2 Avulsion of permanent teeth is seen in 0.5–3% of alldental injuries3
Storage Medium
A storage medium may be defined as a physiological solution that closely replicates the oral environment to help preserve the viability of PDL cells following avulsion.4
The ideal requirements for a storage medium are5
It should have antimicrobial characteristics
It should maintain the viability of periodontal fibres for an acceptable period of time
It should favour proliferative capacity of the cells (clonogenic and mitogenic capacity)
It should have the same osmolarity as that of body fluids (290-300 mosmol/ kg) and pH balanced (7.2 – 7.4)
It should be unreactive with body fluids
It should not produce any antigen-antibody reactions
It should reduce the risk of post-replantation root resorption or ankylosis
It should have a good shelf life
It should be effective in different climates and under different conditions
It should wash off extraneous materials and toxic waste products
It should aid in reconstitution of depleted cellular metabolites.
Use of such a storage media has been associated with favourable healing outcomes.
The storage media can be classified as Laboratory prepared and Natural source.5
| Laboratory prepared | Natural source |
| Hank’s Balanced Salt Solution | Milk |
| Normal saline | Saliva |
| ViaSpan | Propolis |
| Eagle’s medium | Coconut water |
| Custodiol | Egg white |
| Dubelco’s storage | Emdogain |
| Tooth rescue box | Morusrubra |
| Conditioned medium | Salvia officinalis extract |
| Gatorade | Honey milk |
| Contact lens solution | Tap water |
| Growth factors | |
| Ascorbic acid | |
| L-DOPA | |
| Cryoprotective agents | |
| Catalase supplementation |
There is not a single product or solution thatpossesses all the characteristics required to be indicatedas the ideal storage medium for avulsed teeth, that is,
be capable of preserving the vitality of the PDL and pulpcells, while presenting compatible physiological pH andosmolality, clonogenic capacity, antioxidant property, no orminimal microbial contamination, high availability, readyaccessibility at accident sites, homes, schools, hospitalsand dental offices, and low cost.Milk is anisotonic liquid with a physiologically compatible pH andosmolality (fluid pressure) with the root-surface adheredPDL cells, has low or no bacterial content, contains growthfactors and essential nutrients for cells, in addition tobeing highly available mostly everywhere and having alow cost. Taking together the characteristics, efficacyand availability and accessibility, milk appears as the bestindication of a temporary storage medium for avulsedteeth before replantation, and its use is recommended bythe International Association of Dental Traumatology andthe American Academy of Pediatric Dentistry.6
Outcomes Of Avulsion
The speed with which the avulsed tooth is replanted is the most importantfactor for success. There are several possible effects on the rootsurface and attachment apparatus of an avulsed tooth.
Normal PDL healing: complete regeneration of the PDL. Damagecannot be clinically or radiographically detected.
Surface resorption: the crushing injury is restricted, inflammatoryresponse is limited and repair can occur with replacement cementum.Clinically, the tooth presents aymptomatic, with normal mobility andpercussion sounds. Radiographically, there are no periradicularradiolucencies and no loss of lamina dura.
Ankylosis and replacement resorption: occurs when excessive dryingdamages the PDL cells and evokes an inflammatory response thatresults in the replacement of the cells with alveolar bone.Dentoalveolarankylosis is the term used when precursor bone cellspopulate the damaged root resulting in a direct bone-root contact voidof an attachment apparatus. Replacement resorption occurs whenosteoclasts in contact with the root resorb dentin that is eventuallyreplaced with new bone by osteoblasts. Clinically, the tooth will beimmobile and have a high-pitched sound when percussed.Radiographically, there is absence of the lamina dura. Withreplacement resorption, the root surface appears moth-eaten. Inyoung patients, infraocclusion or submergence results whenreplacement resorption interferes with the tooth’s ability to movewith the normal downward growth of the alveolar process.
External inflammatory root resorption: the result of a combination ofseverely damaged attachment and bacterial contamination of anecrotic pulp. It may rapidly progress. Clinically, it presents asradiolucencies in the root and adjacent bone.7
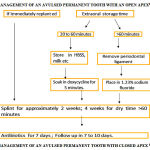 |
Figure 1
|
The Above Steps In The Management Of An Avulsed Permanent Tooth With An Open Apex Followed By Initiatingpulpectomy/Debridement Within 7 To 10 Days.
Adjunctive Treatment And Follow-Up7
Soft tissue management: gingival tissue should be tightly secured in thecervical area of the replanted tooth to help prevent the ingress of bacteria. Lip lacerations must be thoroughly cleaned and approximatedtension-free before suturing. It is best to consult an oral or plastic surgeonif the laceration extends through the vermilion border into the skin.
Splinting
a flexible (semi-rigid) splint is recommended for 7-10 days. Thereare many acceptable types of splints available and it is left to the providerto choose one that is effective and easy to use. The splint should allowphysiologic movement of the tooth, should not have memory and notimpinge on the gingiva. Proper repositioning of the replanted tooth shouldbe verified with a radiograph. Avulsions that have concomitant alveolarfractures should be splinted for 4-8 weeks.
Systemic antibiotics
recommended. If the patient is not susceptible totetracycline staining, the antibiotic of choice is doxycycline at anappropriate dose for patient age and weight. Penicillin V can besubstituted for doxycycline. Adult dosage of doxycycline is 100mg b.i.d. x7 days. Adult dosage of Penicillin V is 1-2g stat, then 500mg q.i.d. x 7days. Fractures of the alveolus may have their own indications for antibiotic coverage
Tetanus
refer the patient to a physician within 48 hours for a tetanusbooster if the avulsed tooth contacted soil or if the status of the tetanuscoverage is uncertain.
Analgesics
prescribe if needed. Typically, an over the counter nonsteroidalanti-inflammatory drug suffices.
Diet
post-operative instructions should include a soft diet for 2 weeks.
Oral hygiene
instruct the patient to brush with a soft toothbrush afterevery meal and prescribe a 0.1% chlorhexidine mouth rinse 2x per day for 7days.
Follow-up appointments
include splint removal and initiation of endodontictreatment, if required, at one week. Clinical and radiographic exams shouldbe scheduled at 2-3 weeks, 3-4 weeks, 6-8 weeks, 6 months, 1 year andannually for 5 years.
Conclusion
Avulsion is one of the most serious dental injuries. It has psychological, esthetic and functional consequences and the prognosis is mainly related to the injury to periodontal membrane. Knowledge levels of the individuals should be improved related to the emergency management of tooth avulsion. This can be done through targeted education programs. Posters and videos to be designed about the management and should be delivered to the public through camps and mass media.
References
- Jyothi KN, Venugopal P, Soumyaranjan Nanda, Mahaveerkumar Shah. Knowledge And Attitude Of Medical Doctors Towards Emergency Management Of Avulsed Tooth- A cross sectional survey. Journal of Dental Sciences & Research 2:1: Pages 156-167
- Abu Dawoud M, Al Enezi ,Andersson L, Knowledge of emergency management of avulsed teeth among young physicians and dentist. Dental Traumatology 2007; 23: 348- 55.
- Lars Andersson et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth.Dental Traumatology 2012; 28: 88–96
- Suresh Kotumachagi Sangappa1, Dr A. Pravin Kumar2, Dr Shruti3, Dr Pooja Srivastava. Extra-Alveolar Storage Media for teeth: A Literature review. International Journal of Advanced Research (2014), Volume 2, Issue 7, 963-972
- Siddiqui et. al., Storage Media for An Avulsed Tooth: Nature to the Rescue. Br J Med Health Res. 2014; 1(3)
- Wilson Roberto Poi, Celso KoogiSonoda, Christine Men Martins, Moriel Evangelista Melo, Eduardo Pizza Pellizzer, Marcos Rogério de Mendonça, Sônia Regina Panzarini. Storage Media For Av u l s e d Te e t h : A L i t e r a t u r e Review.Brazilian Dental Journal (2013) 24(5): 437-445
- Lieutenant ShermaSaif, DC, USNR, and Commander Patricia A. Tordik, DC, USN. Avulsed permanent teeth – new treatment guidelines. Vol 26, no 2, 2004
- McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):137-44.

