
Maria Francis Yuvaraj1 , Thotakura Balaji2, Rajendran Hannah Sugirthabai Rajila2, Gnanasundaram Vaithianathan2, Subramanian Aruna3 and Karunakarn Balaji4
, Thotakura Balaji2, Rajendran Hannah Sugirthabai Rajila2, Gnanasundaram Vaithianathan2, Subramanian Aruna3 and Karunakarn Balaji4
1Tutor Department of Anatomy Saveetha Medical College Hospital Thandalam Chennai India.
2Department of Anatomy Chettinad hospital and Research institute Kelambakkam, Kanchipuram Dist, Chennai, India.
3Department of Anatomy Indira Gandhi medical College and Research Institute Kathirkamam Puduchery, India.
4Meenakshi Ammal Dental College and Hospital Alapakkam , Chennai, India.
Corresponding Author E-mail: sujinalways@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1602
Abstract
The variations in blood vessels are common and have long received the attention of anatomists and surgeons. The true pelvic cavity usually refers to that part of pelvis, which has its bony walls, the sacrum and lower part of hip bone. This small area is well covered by bones and has important structures namely the pelvic viscera, pelvic floor muscles, vessels and nerves supplying it. The aim of the study was to know the branching pattern of internal iliac artery based on the Adachis classification, along with length and thickness of artery. The internal iliac artery was traced from its origin, course, branching pattern, length and thickness of the trunk of internal iliac artery was measured by using digital vernier calliper from its point of origin to bifurcation into anterior and posterior division. The length of right & left internal iliac artery ranged from 2.4 cm to 5.4 cm with average length of 3.943cm ± 0.859cm, whereas the length of left internal iliac artery ranged from 2.7cm to 4.7cm with average length of 3.610cm ± 0.626cm. Bilateral ligation of internal iliac artery is helpful in controlling postpartum haemorrhage. Applying ligatures on an anomalous blood vessel may lead to alarming haemorrhage. The most ideal point of ligation of internal iliac artery would be distal to its posterior division, since proximal ligation has been associated with buttock claudication and necrosis. Knowledge regarding the internal iliac artery and its branches is helpful in applying ligatures safely during pelvic surgeries.
Keywords
Anomalous; Claudication; Internal iliac artery; Ligation; Necrosis; Postpartum Haemorrhage
Download this article as:| Copy the following to cite this article: Yuvaraj M. F, Balaji T, Rajila R. H. S, Vaithianathan G, Aruna S, Balaji K. Study on Variations in the Origin and Branching Pattern of Internal Iliac Artery in Cadavers. Biomed Pharmacol J 2018;11(4). |
| Copy the following to cite this URL: Yuvaraj M. F, Balaji T, Rajila R. H. S, Vaithianathan G, Aruna S, Balaji K. Study on Variations in the Origin and Branching Pattern of Internal Iliac Artery in Cadavers. Biomed Pharmacol J 2018;11(4). Available from: http://biomedpharmajournal.org/?p=24628 |
Introduction
The variations in our body are rampant in nature. Developmental variations of blood vessels, nerves, bones, organs and almost all tissues in the body can occur. Even though many variations occur, they may or may not interfere with the functions of the body. The variations in blood vessels are common and have long received the attention of anatomists and surgeons. The true pelvic cavity usually refers to that part of pelvis, which has its bony walls, the sacrum and lower part of hip bone. This small area is well covered by bones and has important structures namely the pelvic viscera, pelvic floor muscles, vessels and nerves supplying it.
The principal blood supply to the pelvic viscera is by internal iliac artery and its branches. The internal iliac artery also known as hypogastric artery is found bilaterally in the pelvic cavity. It is one of the branches of common iliac artery given in front of the sacroiliac joint and runs downwards sub-peritoneal. At the upper margin of greater sciatic foramen it divides into anterior and posterior divisions. The anterior division gives nine branches while the posterior division gives three branches. It mainly supplies the pelvic cavity, medial compartment of thigh and gluteal region.1 Any compromise in the blood supply will produce ischemia to these organs. The embryological explanations for the variations in the arterial pattern are based on unusual selection of channels from a primary capillary plexus, wherein the most appropriate channels enlarge while others retract and disappear thereby establishing the final arterial pattern.2,3 During posterior pelvic fractures, anterior and anterolateral spinal approaches, lumbosacral spinal endoscopic procedures, lateral disc excision, anterior approaches to the sacroiliac joint for arthrodoses or intenal fixation, injury to the iliolumbar artery may occur. During surgical repair of fracture of superior ramus of pubis, the obturator artery may be injured due to anomalous origin from the external iliac artery which might lead to profuse bleeding. The knowledge regarding the course and branches of internal iliac artery is necessary which might greatly help the surgeon during surgical procedures of the pelvic region. The aim of the study was to know the branching pattern of internal iliac artery based on the Adachis classification, along with the length and thickness of artery.
Materials and Methods
The present study was carried in the Department of Anatomy, Chettinad Hospital and Research Institute. A Total of 80 formalin fixed specimen, inclusive of both male and female were utilized for the present study. The internal iliac artery was traced from its origin and the course of the artery was studied. The length and thickness of the trunk of internal iliac artery was measured by using digital vernier calliper from its point of origin to bifurcation into anterior and posterior division. Variations in the origin and branching pattern of internal iliac artery was recorded and photographed.
Results
The variations in the branching pattern of internal iliac artery were observed in the specimens. The variations in the origin of branches of both anterior and posterior divisions of internal iliac artery were also observed. Among the branches of anterior division, variations were observed in origin of obturator artery, other branches of anterior division showed a normal course. Among the branches of posterior division, variations were observed in the origin of iliolumbar artery, lateral sacral artery and superior gluteal artery. In all 80 specimens, the length of internal iliac artery was measured. In Table:I the length of right internal iliac artery ranged from 2.4 cm to 5.4 cm with average length of 3.943cm ± 0.859cm, whereas the length of left internal iliac artery ranged from 2.7cm to 4.7cm with average length of 3.610cm ± 0.626cm. The calculated P valve (0.0914) shows that the differences between the lengths of internal iliac artery of both sides were statistically not significant.
Table 1: Comparison of minimum, maximum and average length of right and left internal iliac arteries.
| Side | Minimum (cm) | Maximum (cm) | Average (cm) | StandardDeviation | T – Value | P – Value |
| RIGHT | 2.4 | 5.4 | 3.943 | 0.859 | 1.72 | 0.0914* |
| LEFT | 2.7 | 4.7 | 3.610 | 0.626 |
P value ≥ 0.05 not significant
*Statistically not significant
The calibre thickness of main trunk of internal iliac artery (4.85 ± 0.60cm), obturator artery (3.27 ± 0.52cm), ilio-lumbar artery (3.25 ± 0.49cm) were also studied in this study shown in Table:III
The obturator artery took origin from several sources as shown in Table: II it originated from anterior division of internal iliac artery (45%), posterior division of internal iliac artery (20%), with ilio-lumbar artery (3%) or superior gluteal artery (5%), directly from external iliac artery (5%) or from inferior epigastric artery (22%).
Table 2: Different modes of origin of obturator artery
| S.No | Mode of Origin | Percentage |
| 1 | Anterior division of Internal iliac artery | 45 |
| 2 | posterior division of Internal iliac artery | 20 |
| 3 | With ilio-lumbar artery | 3 |
| 4 | Superior gluteal artery | 5 |
| 5 | External Iliac artery(Direct) | 5 |
| 6 | Inferior epigastric artery | 22 |
Branching pattern of obturator artery in present study with percentage.
Table 3: Various origins of ilio lumbar artery
| S.No | Modes of Origin | Present Study | Previous Study Chandrika et al., 2013 | Kiray et al., 2010 |
| 1 | Posterior division | 25% | 80% | 19% |
| 2 | Trunk of internal iliac artery | 75% | 20 | 71.4% |
| 3 | External iliac artery | – | – | – |
| 4 | Common iliac artery | – | – | 4.8% |
| 5 | Abdominal aorta | – | – | – |
Branching pattern of iliolumbar artery
The origin of ilio lumbar artery from main trunk of internal iliac artery was observed in 75% of the specimen. In rest of the cases, ilio lumbar artery originated from posterior division of internal iliac artery as showed in Table: IV
Table 4: Thickness of important branches of internal iliac artery
| S.No | Thickness of Arteries | Mean | Standard Deviation |
| 1 | Thickness of trunk | 4.85 | 0.60 |
| 2 | Thickness of obturator artery | 3.27 | 0.52 |
| 3 | Thickness of ilio lumbar artery | 3.25 | 0.49 |
Calibre thickness of branches of internal iliac artery
Discussion
The first known person to do a study on variations of internal iliac artery was Jaschinski in 1891. Later this study was modified by Adachi19284 and he added the 5th type. The variations in branching pattern of internal iliac artery are mainly due to embryological reasons. Abnormal vasculature could be abnormal angiogenesis, as a result of hypoxia, as low oxygen saturation leads to the stabilization of hypoxia inducible factor 1-A, which upregulates vascular endothelial growth factor (VEGF) and nitric oxide synthase expression. The production of nitric oxide causes dilation of the existing vessels and extravasation of plasma proteins, leading to protease and matrix metalloproteinase expression. The plasma proteins then play a major role in the proliferation and angiogenesis of endothelial cells which leads to formation of abnormal vasculature. The variations in vasculature are essential while performing surgery for safe and successful outcomes. In our study the variations are more commonly seen in the following arteries namely, obturator artery, iliolumbar artery, lateral sacral artery and superior gluteal artery.
Obturator Artery
The variations observed in obturator artery and its accessory artery are difference in origin and in its relation to pubic ramus. The internal iliac artery usually provides the obturator artery, which may communicate with the external iliac artery through either the accessory obturator or inferior epigastric artery. A collateral circulation between the external and internal iliac system is known as Corona mortis.5 The most commonly occurring variation in internal iliac artery is associated with obturator artery. Normally the obturator artery takes origin from the anterior division of internal iliac artery. In our study only about 45% were from anterior division, while the rest of them had different origins. About 20% originated from the posterior division as shown in Fig: 1. This is mainly due to persistence of vascular channels in relation to the posterior division and the vascular channels in relation to the anterior division might be disappeared.6 The origin of obturator artery from the posterior division had increased the length of obturator artery, thus providing an added advantage for vascular grafting.3 The posterior division variation is most commonly seen by Kumar and Sharmishta et al.6,7 The origin of obturator artery from inferior epigastric artery is previously reported by Sanudo JR et al [8]. In the present study Fig: 2 shows, origin from inferior epigastric is 22%. The origin of obturator artery from external iliac artery is only 5% and it is also previously reported by Pung papong SU et al [9]. The origin of obturator artery from superior gluteal artery is very minimally reported and in our study it is only 5% as shown in Fig: 3. In 3% of specimens, it originated commonly wtih ilio-lumbar artery Fig: 4. The knowledge regarding the calibre of the vessel is also important for ligation of obturator artery during various pelvic surgeries. The average size of calibre is 3.27 ± 0.5cm. A complete knowledge of abnormal origin of arteries in the retropubic pelvic vascular anatomy plays an important role in reducing the complications while performing endoscopic, inguinal herinoplasty and laparoscopic surgical procedure [10].
 |
Figure 1: Origin of obturator artery from posterior division of internal ilac artery.
|
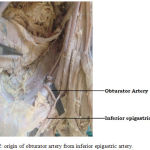 |
Figure 2: Origin of obturator artery from inferior epigastric artery.
|
 |
Figure 3: Origin of obturator artery from superior gluteal artery.
|
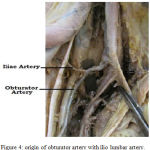 |
Figure 4: Origin of obturator artery with ilio lumbar artery.
|
Iliolumbar Artery
Iliolumbar artery arises from posterior division of internal iliac artery and is important, as it may be injured during lumbo sacral spinal surgeries. It further divides into iliac and lumbar branch at the medial side of psoas major and supplies cauda equina. Later it anastomosis with 4th lumbar artery.11 In our study we mainly studied the modes of origin and also calculated the calibre of the artery. The artery took origin from the trunk of internal iliac artery in 75% as shown in Fig: 5, as against the previous studies done by Kiray (71.4%) and Chandrika (20%).12,13 In 25%, it took origin from the posterior division of internal iliac iliac artery as shown in Fig: 6 and the artery did not take origin from the external iliac artery, common iliac artery and abdominal aorta. The average size of the calibre was 3.2 ± 0.5cm whereas, in Chandrika et al.,13 it was 3.4 ± 0.5cm. Ilio lumbar arteries are used as vascular pedicles in iliac crest flaps. The relationship of artery with sacropelvic joint is importantly considered because during the shear fracture or open book fracture, it is possible to injury the artery.14,15 The arterial anatomy of the pelvis, lumbar vertebrae and the sacrum is very important in neurosurgeries and orthopedicans for spinal fixations.
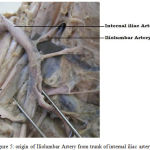 |
Figure 5: Origin of Iliolumbar Artery from trunk of internal iliac artery.
|
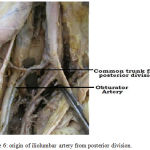 |
Figure 6: origin of iliolumbar artery from posterior division.
|
Lateral Sacral Artery
Lateral sacral artery is a branch from posterior division of internal iliac artery. It commonly divides into superior and inferior branches and mainly supplies the lumbar and sacral roots.16 The variations in the origin of lateral sacral artery are concerned with sciatic artery. The lateral sacral artery plexus does not arise from the dorsal aspect of primitive axial artery due to delay in posterior trunk development and early anterior trunk development. The lateral sacral artery arises directly or indirectly from internal iliac artery due to regression from sciatic artery.17,18 In previous studies the artery took origin from anterior trunk in 1%, posterior trunk in 79%, dorsally in 3.7%, superior gluteal artery in16.8% inferior gluteal artery in 5.4%, internal pudendal artery in 0.3%, and persistent sciatic artery in 8.8% .19 In the present study the artery originated from the trunk of internal iliac artery as shown in Fig: 7. Lateral sacral artery aneurysm associated with thrombosis can create pressure or impairment of the collateral circulation. If the blood supply is minimal to sciatic sacral roots it may lead to sciatic neuropathy with symptoms of sciatica.20,21 The origin may be helpful for orthopaedic and neurosurgeons while doing graft and lumbar surgeries.
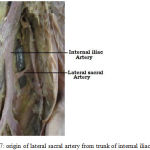 |
Figure 7: Origin of lateral sacral artery from trunk of internal iliac artery.
|
Superior Gluteal Artery
The origin of superior gluteal artery from the trunk of internal iliac artery which was observed in the present study is seldom reported (3%). It is either mentioned by Adachi (1928),4 Villimen (1952),22 Kosinski (1929),23 or Terek (2004).24 Sound knowledge of superior gluteal vessels is required during surgical repair of acetabular fractures. Knowledge of superior gluteal artery is essential for constructing myocutaneous flaps since the branches of this artery anastomosis with inferior gluteal, lateral circumflex and deep circumflex arteries.25
Length of Internal Iliac Artery
Knowledge regarding the length of internal iliac artery is absolutely necessary while applying ligature to the internal iliac artery during various pelvic surgeries. The morphometry of the artery at its origin and length were previously studied.26,27,28
The length of the internal iliac artery varies in different races. The length for English is 36.8±0.6mm,26 Japanese is 44.3±1.32mm,4 Romanian is 49±3.34mm29 and in south Indian population is 37±4.62mm.30 According to present study, the length of the artery ranged between 2.4 and 5.4cm. The mean value was 37.7±0.76mm without major differences between two sides. These value matches with previous study by Naveen et al.,30 in south Indian population (37±4.6mm).
A severe and potentially lethal complication in pelvic injuries is arterial bleeding commonly involving the branches of the internal iliac artery, namely, the lateral sacral, iliolumbar, obturator, vesical, and inferior gluteal arteries. The most ideal point of ligation of internal iliac artery would be distal to its posterior division, since proximal ligation has been associated with buttock claudication and necrosis.
Conclusion
In the present study variations in the origin of obturator artery, iliolumbar artery, lateral sacral artery and superior gluteal artery were observed. Among the branches mentioned above obturator artery showed a higher incidence of variations. The average length of internal iliac artery was found to be 37.7± 0.76mm and there was no significant difference in the length between the right and left side. Bilateral ligation of internal iliac artery is helpful in controlling postpartum haemorrhage. Applying ligatures on an anomalous blood vessel may lead to alarming haemorrhage. Knowledge regarding the internal iliac artery and its branches is helpful in applying ligatures safely during pelvic surgeries.
Acknowledgments
The author(s) received no specific funding for this work.
References
- Susan Standring,Gray’s Anatomy: The Anatomical Basis of Clinical Practice, Elsevier, London, UK, 40th edition. 2008;1086-1089.
- Arey L. B. The development of peripheral blood vessels. In: Smith J. L., Orbison D. E., editors. The Peripheral Blood Vessels. Baltimore, Maryland, USA: Williams & Wilkins Co. 1963;1–16.
- Fitzgerald M. J. Human Embryology: A regional approach. . New York, USA: Harpercollins College Div; 1st edition. 1978;38–56.
- Adachi. Das Arteriensystem der Japaner,” in Supplementb ande zu den “Acta Scholae Medicinalis Universitatis Imperialis in Kyoto”, Bd. II. Aorta thoracalis. Arcus plantaris profundus. Kyoto, Kai-serlich-japanische Universit¨at zu Kyoto, in Kommission bei, Maruzen, Kyoto, Japan. 1928;9.
- Al T. W. A new concept and classification of corona mortis and its clinical significance. Chinese Journal of Traumatology. 2016;19:251-254.
- kumar D and rath G. Anomalous origin of Obturator artery from the internal iliac artery. Intl.J. Morphol. 2007;25:939-41.
- Biswas S. Variation of origin of Obturatorartery in eastern Indian population – A study. Journal of Anatomical Society of India. 2010;59(2):168-72.
- Sañudo Jr., Mirapeix R., Niedenführ M. R., Maranillo E., Parkin I. G. Vázquez T. Obturador artery revisited. International urogynecology. journal and pelvic floor dysfunction. 2011;22(10):1313-1318. Http://dx.doi.org/10.1007/ s00192-011-1467-3.
- Pungpapong S. U, Thum-umnauysuk S. Incidence of corona mortis preperitonealanatomy for laparoscopic hernia repair. J Med Assoc Thai. 2005;88:51-53.
- Lau H., Lee F. A prospective endoscopic study of retropubic vascular anatomy in 121 patients undergoing endoscopic extraperitoneal inguinal hernioplasty. Surg Endosc. 2003;17:1376–9.
- Winters H. A., van Harten S. M., van Royen B. J. The iliolumbar artery as the nutrient pedicle for an iliac crest graft: a new technique in reconstruction of the lumbar spine. Plast Reconstr Surg. 2002;109:249-52.
- Yiming A., Baqué P., Rahili A., Mayer J., Braccini A. L., Fontaine A., et al. Anatomical study of the blood supply of the coxal bone: radiological and clinical application. Surg Radiol Anat. 2002;24: 81-86.
- Kiray et al. Anatomical variations of iliolumbar artery and its relation with surgical landmarks. Acta Orthop Traumatol Turc. 2010;44(6):464-468
- Teli G. C et al., Morphometry of Iliolumbar Artery, Iliolumbar Veins. JCDR. 2013;7(3):422-426.
- Harrington J. F Jr. Far lateral disc excision at L5-S1 complicated by iliolumbar artery incursion case report. Neurosurgery. 2001;48:1377-80.
- Carter. Anatomy Descriptive and Surgical, BlanchardandLea, Philadelphia, Pa, USA, 1st edition. 1858.
- Day H. The blood supply of the lumbar and sacral plexuses in the human foetus. Journal of Anatomy. 1964;98(1):105–116.
- Naguib N. N., Nour-Eldin N. E. A., Hammerstinglet R. M. al., Three-dimensional reconstructed contrast-enhanced MR angiography for internal iliac artery branch visualization before uterine artery embolization. Journal of Vascular and Interventional Radiology. 2008;19(11):1569–1575.
- Poynter W. M. Congenital anomalies of the arteries and veins of the human body of man with bibliography,” University Studies of the University of Nebraska. 1922;22:1–106.
- Alberstone D., Rupp F. W and Anson J. A. Spinal aneurysm of the lateral sacral artery case report. Journal of Neurosurgery. 2000;92(1):101–104.
- Ates O. K., Cayli S. R and Sarac K. Isolated posterior spinal artery aneurysm.British Journal of Neurosurgery. 2006;20(4):241–244.
- Villemin F.,Rigaud A., Gouuaza A. General considerations of divisions of the internal iliac artery: fixed course of the pudendal and superior gluteal mobile element of inferior gluteal. Sem.Med. 1952;28:211-213.
- Kosinski C. Quelques notions sur la ramification des arteries iliiaques. CR Ass. Anat. 1929;46-48.
- Terek M. C., Saylam C., Orhan M.,Ylmaz A., Oztekin k. Surgical anatomy of the posterior division of the internal iliac artery: the important point for internal iliac artery ligation to control pelvic haemorrhage. Aust N.Z. J Obstet. Gynaecol. 2004;44:374.
- Zhonghua Zheng Xing Wai Ke Za Zh Anatomy study of superior and inferior gluteal artery perforator flap. 2005;21(4):278-80.
- Quain J. In: W. Sharpey (Ed.), Quain’s Elements of Anatomy, 8th ed, London. 1908;1.
- Tesut L. Traited. anatomiehumaine, ed. Masson,Paris (tome IV). 1948.
- Kosinski C. Quelques notions sur la ramification des arteries iliiaques. CR Ass. Anat. 1929;46-48.
- Fatu C, Puisoru M, FatuIC.Morphometry of the internal iliac artery in different ethnic groups. Annals of Anatomy. 2006;188:541-546.
- Naveen N. S.,Murlimanju B. V., Kumar V et al. Morphological Analysisof human internal iliac artery in south Indian population. OJHAS. 2011;10(1):11.

