Assessment of Myeloperoxidase Levels in Relation to the Nature and Duration of Orthodontic Forces – An In Vivo, Split Mouth Study
 , Poornima Manjrekar2, Asavari Desai1 and Pramod Philip3
, Poornima Manjrekar2, Asavari Desai1 and Pramod Philip3 1Department of Orthodontics, Manipal College of Dental Sciences, Manipal Academia of Higher Education Mangalore 576104 , India.
2Department of Biochemistry, Kasturba Medical College, Mangalore, India.
3Department of Orthodontics, Case Western Reserve University, Ohio, USA.
Corresponding Author E-mail: supriya.nambiar@manipal.edu
DOI : http://dx.doi.org/10.13005/bpj/1583
Download this article as:
![]()
To assess the change in the myeloperoxidase levels(MPO)in the gingival crevicular fluid(GCF) at different time intervals during the course of orthodontic treatment with the application of intermittent and continuous forces. It was an interventional, split mouth study done on twenty patients scheduled to undergo fixed orthodontic treatment with therapeutic extractions of the first premolars.Mini implant assisted enmasse retraction was done after leveling and aligning of the arch.Continuous force with the help of Niti coil spring was used in the first quadrant and intermittent force with an elastomeric chain was used in the second quadrant. MPO was collected from the GCF using What man’s paper at baseline,1 week and 2 weeks after the application of retraction forces.The levels were assessed using a commercially available ELISA kit. Mean MPO activity was increased in the GCF of all the patients at 1 and 2 weeks after retraction,in both quadrants.At 2 weeks, MPO levels at the intermittent force application site were found to be significantly higher than those at the site of continuous force application. Myeloperoxidase is a useful marker to assess inflammation associated with orthodontic tooth movement.Intermittent forces cause a higher degree of inflammation as compared to continuous forces.
KEYWORDS:Inflammation; Myeloperoxidase; commercially
Introduction
Tooth movement by orthodontic force application is characterized by remodeling changes in dental and paradental tissues, including dental pulp, periodontal ligament(PDL),alveolar bone and gingiva. These tissues, when exposed to varying degrees of magnitude, frequency and duration of mechanical loading,express extensive macroscopic and microscopic changes. Orthodontic tooth movement differs markedly from physiological tooth eruption which is a slow process that occurs mainly in the occlusal and mesial direction into cancellous bone.In contrast,orthodontic tooth movement is characterized by the abrupt creation of compression and tension regions in the PDL and can occur rapidly or slowly depending on the characteristics of the applied force and the biological response of the PDL. These force-induced strains alter the PDL’s vascularity and blood flow resulting in local synthesis and release of various key molecules such as neurotransmitters, cytokines, growth factors, colony-stimulating factors and arachidonic acid metabolites. These molecules evoke many cellular responses by various cell types in and around teeth, providing a favorable microenvironment for tissue deposition or resorption.1
Orthodontic movements promote remodeling of the alveolar bone,which is mediated by inflammatory-like reactions characterized by vascular changes and infiltration of leucocytes. During orthodontic movements changes in the periodontium occur, depending on the magnitude, direction, and duration of the applied force. Biochemical analysis of the gingival crevicular fluid (GCF) is a useful and promising method for monitoring these changes at a single site during a certain period as well as investigating the response of dental and periodontal tissues to fixed orthodontic appliance forces.
Azurophilic granules of polymorphonuclear neutrophils (PMNs) contain the enzyme myeloperoxidase (MPO), which is included in the host-derived group of compounds that are important for the tissue defense promoted by PMNs.It has been established that the level of MPO activity is directly correlated with the number of PMNs in the tissues and therefore MPO activity,but not its protein amounts is used in studies on inflammation of tissues.Studies conducted previously have shown that MPO is increased in the GCF collected from inflamed sites.
Since MPO levels found in the GCF represent the extent of PMN infiltration,the determination of MPO will be a valuable tool to assess the degree of inflammation in tissues which is of particular significance in orthodontics.After the application of this force,PMNs migrate into the tissues and finally extravasate in increased numbers into the GCF.
Previous studies have found that MPO level is increased in patients undergoing fixed orthodontic2 treatment but the characteristics of the involved mechanical stress have not been specified.3
Therefore this study was done to investigate the changes of MPO levels in the gingival crevicular fluid with different types of force in vivo.
Objectives
To assess the change in the myeloperoxidase levels in GCF at different time intervals during the course of orthodontic treatment with the application of intermittent and continuous forces.
Materials and Methods
It was an experimental, in vivo split mouth study for which clearance from the Institutional Ethics Committee,Manipal College of Dental Sciences,Mangalore dated 13th December,2014 (Ref No:MCODS198/2014) was obtained.
Methods
Twenty orthodontic patients who were scheduled to undergo fixed appliance therapy were enrolled in the study with prior informed consent. Patients of either gender,requiring therapeutic extraction of the first premolars and were generally healthy were included in the study.Smokers and subjects who had been administered anti- inflammatory drugs/antibiotics in the month preceeding the study or had periodontally compromised dentitions were not considered.
Fixed appliance therapy was started using brackets with an 0.022” slot and Roth prescription.Levelling and aligning was carried out conventionally after which space closure was initiated by enmasse retraction using mini implants(SK Surgicals,India) placed between the second premolar and first molar.
In order to compare the effect of continuous and intermittent forces on MPO levels, a Niti closed coil spring(6mm,Astradent,India) and closed clear elastomeric chain(Rabbit force,India) was used in the first and second quadrants respectively.A retraction force of five ounces,measured with a Dontrix gauge,was used on both sides.
GCF samples were taken from the mesiobuccal or distobuccal aspects of the canine using Whatman absorbent paper strips in both quadrants and were maintained separately in different vials.The GCF samples were taken at three time intervals namely,
T1- (Baseline sample)-taken before retraction was begun,
T2-After one week of retraction
T3-After two weeks of retraction.
Oral hygiene was maintained by oral prophylaxis and reinforcing instructions.Subjects were instructed not to consume anything for 1 hour before the examination. After isolating the tooth with a cotton roll, the crevicular site was gently dried with an air syringe. The GCF samples were collected by using Whatman absorbent paper strip placed into the sulcus or pocket until mild resistance was felt and left in place for 30 seconds(Figure 1)All the samples were always taken from the same site at the 3 time points.Strips contaminated by saliva or blood were excluded.At T1 and T2, the elastomeric chain placed in the left quadrant was reactivated and the force was calibrated to five ounces as described by H Park et al4.The NiTi closed coil spring used on the right side was left as such. All strips with GCF were immediately and individually placed in Eppendorf vials containing 100 mL of buffer (50 m mol/L Tris-HCl, pH 7.4; 200 m mol/L NaCl; 10 m mol/L CaCl2;and 0.02% Triton X-100). The vials were maintained on ice for 30 minutes and then centrifuged at 13,000g for 10 minutes at 4 degree celsius(Figures 2).Supernatants were stored at –70 degree C until further analysis.All analyses were performed directly on this 100 mL sample,without further dilution.
 |
Figure 1: GCF collection on the right side.
|
 |
Figure 2: GCF samples before cold centrifugation.
|
The Myeloperoxidase levels were then estimated using commercially available ELISA kit(QAYEE BIO QY EO1364).It uses a double-antibody sandwich enzyme-linked immunosorbent one-step process assay (ELISA) to assay the level of Myeloperoxidase(MPO).
The test was run by addition of standard,test sample and HRP-labeled Myeloperoxidase(MPO) antibodies to enzyme wells which were pre-coated with Myeloperoxidase(MPO) antibody,then the wells were incubated and washed to remove the uncombined enzyme.Upon adding chromogen solution A and B, the color of the liquid changed into blue, and the reaction with the acid caused the color to change to yellow.The depth of color and the concentration of the Myeloperoxidase(MPO) sample are positively correlated.
Statistical Analysis
The statistical analysis was performed using Statistical Package for Social Sciences(SPSS version 20).
Students unpaired `t` test was performed to assess the correlation between right and left quadrants where light continuous forces and intermittent forces were applied respectively,at the three time intervals -T1,T2 and T3.
Analysis of variance(ANOVA) was used to determine whether there were any significant changes in either of the two sides over the duration of the study at T1, T2 and T3.The values of this procedure were derived using Fisher test.
To compare the changes of the right and left sides separately over the duration of the study at the mentioned timelines and to check whether there are any significant changes at different intervals, Bonferroni`t` test was carried out.
Results
Comparison of intragroup changes in MPO levels at the three timelines (Table 1)
Table 1: Group statistics to compare intragroup changes at the three time intervals using Students’ unpaired t test.
| Time | Side | N | Mean | Std. Deviation | T |
| T1 | R | 20 | 298.850 | 22.354 | 1.612 |
| L | 20 | 287.000 | 24.092 | p = 0.115 | |
| T2 | R | 20 | 346.650 | 27.683 | 1.580 |
| L | 20 | 330.950 | 34.759 | p = 0.122 | |
| T3 | R | 20 | 325.050 | 27.927 | 2.590 |
| L | 20 | 349.750 | 32.195 | p = 0.013 |
p values of <0.05 were considered as statistically significant.
At T1,the mean value of Myeloperoxidase for the right side(light continuous force) was found to be 298.85 ng/ml s.d 22.35.and the left side(intermittent force) it was 287ng/ml s.d.24.09.
At T2,the mean value of Myeloperoxidase for the right side was found to be 346.65 ng/ml s.d.27.68 whareas for the left side it was 330.95 ng/ml s.d.34.75.
At T3,the mean value of Myeloperoxidase for the right side was found to be 325.05 ng/ml s.d.27.92 whereas for the left side it was 349.75 ng/ml s.d. 32.19.
Students `t` test revealed a statistically significant difference between right and left sides at T3 with a p value of 0.013. However,no significant difference was noted at T1 and T2 with p values of 0.115 and 0.122 respectively.
Comparison of MPO levels between the two quadrants at all the three timelines
The mean, standard deviation, fisher test value and p values for the same are given in (Table 2,fig 3).
Table 2: Descriptive statistics to compare MPO values at the three time periods for right side(continuous force) and left side(intermittent force) using ANOVA.
| SIDE | N | Mean | Std. Deviation | F | p | |
| R | T1 | 20 | 298.850 | 22.354 | ||
| T2 | 20 | 346.650 | 27.683 | |||
| T3 | 20 | 325.050 | 27.927 | 16.803 | <0.001 | |
| T1 | 20 | 287.000 | 24.092 | |||
| T2 | 20 | 330.950 | 34.759 | |||
| T3 | 20 | 349.750 | 32.195 | 22.026 | <0.001 | |
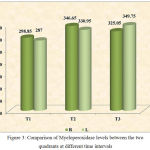 |
Figure 3: Comparison of Myeloperoxidase levels between the two quadrants at different time intervals.
|
For the right side where continuous force was applied, the mean value of Myeloperoxidase at T1 was found to be 298.85 ng/ml 22.35.At T2 it was 346.65 ng/ml s.d.27.68 and T3 the mean was 325.05 ng/ml s.d. 27.92.
For the left side,the mean value of myeloperoxidase at T1 was 287.00 ng/ml s.d.24.09.At T2 the mean was 330.95 ng/ml s.d. 34.75 and at T3 the mean value was 349.75 ng/ml s.d. 32.195.
Analysis of variance(ANOVA) revealed that the MPO levels for the right side at the three time levels was found to be highly significant at p value of <0.001.The Fisher value was 16.803.
Similarly the myeloperoxidase values for the left side at the three timelines was also found to be highly significant at p value of <0.001.The Fisher value was 22.026.
For the right side, the comparison of myeloperoxidase values between T1 and T2 showed mean difference of 47.80 which was highly significant at p value of <0.001. The comparison between T1 and T3 showed a mean value of 26.20 which was statistically highly significant with a p value of 0.007. The comparison between T2 and T3 showed a mean difference 21.60 which was significant at p value of 0.34.
Comparison of MPO levels of the right and left quadrants at a particular time line and its relation to the other two timelines (Table 3)
Table 3: Multiple comparison statistics used to compare value of MPO at a particular time period for the two sides with the value of MPO at the other two time periods using Bonferroni`s t test.
| SIDE | (I) time | (J) time | Mean Difference (I-J) | P |
| R | T1 | T2 | 47.800 | <0.001 |
| T3 | 26.200 | .007 | ||
| T2 | T3 | 21.600 | .034 | |
| L | T1 | T2 | 43.950 | <0.001 |
| T3 | 62.750 | <0.001 | ||
| T2 | T3 | 18.800 | .173 |
Similarly for the left side,the comparison of myeloperoxidase values between T1 and T2 showed mean difference of 43.95 which was highly significant with a p value of <0.001.The MPO levels between T1 and T3 showed mean difference of 62.75 which was also highly significant with a p value of <0.001.However, the difference between T2 and T3 was not significant as the p value was 0.173.
Discussion
Judging the amount of inflammation after the application of orthodontic forces has always remained elusive for the orthodontist.There was always felt a need for some simple efficient technique which would help an orthodontist to gauge the amount of inflammation around a specific site.This is all the more important so as to avoid potential problems arising from excessive forces which could then only be seen after taking X-rays several months into the treatment.
Several studies in the past have been done to evaluate the level of inflammatory markers such as cytokines and proteases during orthodontic tooth movement.5,6,7 In this study,we have attempted to measure the effect on Myeloperoxidase levels during enmasse retraction using intermittent force and light continuous force in different quadrants.A significant advantage of assessing myeloperoxidase levels over cytokines and proteases is that it can be measured with a relatively simple assay which just uses substrate of the enzyme (MPO) and after a mere 30 minutes of reaction the readings can be obtained,so this could prove to be a valuable chairside tool in the days to come.
Due to the high sensitivity and specificity required for the detection of myeloperoxidase in the sparse quantity of GCF available for the study,ELISA was thought to be more reliable method for estimation as opposed to manual method which has been used for samples having relatively larger volume such as plasma and serum. ELISA has been used earlier in many studies8-14 for the estimation of various inflammatory mediators levels throughout the studies to give precise measurements with least amount of human errors possible in manual estimation techniques.
A similar study was done by Lee KJ et al15 in 2004 where the effect of light continuous forces and interrupted force on interleukin-1 and prostaglandin E2 was assessed in vivo. For the quadrant where continuous force was applied, there was significant upregulation of IL-1 beta after 24 hours of force application.The levels reduced thereafter but still remained higher than baseline levels.A second peak was seen after 28 days of force application which was due to the surge of cytokines due to their periodic recycling at around the same time period.However,on the interrupted side after initial peak at 24 hrs there was another peak after 1 week due to rhythmic activation of the appliance but there was an insignificant increase seen at second reactivation at second week which was postulated due to the feedback mechanism of cytokines over the inflammatory markers.The results of the study are concurrent with the findings of our study.
A study done by Grieve et al16 in 1994 which measured IL-1 beta and PGE levels showed the values of these mediators significantly increased after 24 hours of force application but came back to baseline levels after 1 week of orthodontic tooth movement.Similarly,a study done by Uematsu et al6 also showed increased levels of TNF-alfa, IL`s and epidermal growth factor after 24 hours of appliance activation but dropped to normal levels after a week.The probable reason behind this was that force levels decay after a while leading to declining cytokine levels.Contrary to this study,a study done by Tzannetou et al17 showed significant and constant increased levels of IL-1 beta till 28 days after a regular regime of rapid palatal expansion,which used heavy interrupted forces provided by screws.The possible reason given for this was the tendency of relapse of expansion bringing the two segments of maxilla together thereby increasing levels of inflammation or due to alterations brought about in the soft tissue
The use of a split mouth design in the current study for the measurement of MPO between the two different nature of forces has proven to be a reliable and effective study design as demonstrated by an interesting study done by Yamaguchi M. et al11 in 2009.He used conventional brackets in the maxillary left quadrant and the Damon system in the maxillary right quadrant.GCF samples were collected at specified time intervals.He concluded that the side on which self-ligating brackets were bonded showed significant lower levels of substance P,a potent marker of inflammation and pain, compared to the quadrant having conventional bracket system.On similar lines myeloperoxidase, also an inflammatory mediator,shows an initial high level of MPO suggesting increased degree of inflammation during course of orthodontic treatment in conventional bracket system.
In the present study,we have used NiTi closed coil springs to provide continuous forces but as has been shown by the study done by Cox C et al18 in 2014,there is a statistically significant force decay which is approximately 12 percent after 4 weeks of activation and another 5 percent at 8 weeks.After this it remains steady.However,this decay was negated in our study since all the samples were collected within 3 weeks.Hence we expected a reasonably constant amount of force throughout the study period.
Studies done by Kapoor P et al8 and Ahmet Arif Celebi et al19 demonstrated a significant correlation between gender and mediator levels.Mediators such as PG E2 and IL-1B have a significant correlation with the ovarian activity during orthodontic tooth movement. These mediator levels were found to be significantly and consistently lower in esterous groups than in anesterous and ovariectomized groups whereas no such correlation has been established between myeloperoxidase and ovarian activity to our knowledge.This again shows the significance of measuring MPO levels without bothering about this confounding factor.
Multiple comparisons between MPO levels at a particular time point to the remaining timelines also revealed significant values. The only insignificant value found here was the change from T2 to T3 on the left side with intermittent force.The possible reason for this as mentioned by Richard J. smith et al20 in 1984 could be due to formation of wide area of hyalinization on the pressure side leading to formation of wide acellular zone and impediment of release of cytokines into the gingival crevice.
Conclusion
The findings of this study show that the nature of the orthodontic force applied significantly affects inflammation,which was demonstrated by different levels of Myeloperoxidase with continuous and intermittent forces.Intermittent forces lead to significantly higher levels of inflammation compared to light,continuous forces and hence should be preferably avoided to bring about any kind of tooth movement.
References
- Krishnan V., Davidovitch Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am J Orthod Dentofac Orthop. 2006;129(4). doi:10.1016/j.ajodo.2005.10.007.
CrossRef - Marcaccini A. M., Amato P. A. F., Leão F. V., Gerlach R. F., Ferreira J. T. L. Myeloperoxidase activity is increased in gingival crevicular fluid and whole saliva after fixed orthodontic appliance activation.Am J Orthod Dentofac Orthop. 2010;138(5):613-616. doi:10.1016/j.ajodo.2010.01.029.
CrossRef - Lee K. J., Park Y. C., Yu H. S., Choi S. H., Yoo Y. J. Effects of continuous and interrupted orthodontic force on interleukin-1? and prostaglandin E2 production in gingival crevicular fluid. Am J Orthod Dentofac Orthop. 2004;125(2):168-177. doi:10.1016/j.ajodo.2003.03.006.
CrossRef - Park H. S., Kwon T. G. Sliding mechanics with microscrew implant anchorage. Angle Orthod. 2004;74(5):703-710. doi:10.1043/0003-3219(2004)074<0703:SMWMIA>2.0.CO;2.
- Alhashimi N., Frithiof L., Brudvik P., Bakhiet M. Orthodontic tooth movement and de novo synthesis of proinflammatory cytokines. Am J Orthod Dentofacial Orthop. 2001;119(3):307-312. doi:10.1067/mod.2001.110809.
CrossRef - Uematsu S., Mogi M., Deguchi T. Increase of transforming growth factor-beta 1 in gingival crevicular fluid during human orthodontic tooth movement. Arch Oral Biol. 1996;41(11):1091-1095. doi:S0003-9969(96)00063-5 [pii].
- Lowney J. J., Norton L. A., Shafer D. M., Rossomando E. F. Orthodontic forces increase tumor necrosis factor ?? in the human gingival sulcus. Am J Orthod Dentofac Orthop. 1995;108(5):519-524. doi:10.1016/S0889-5406(95)70052-8.
CrossRef - Kapoor P., Kharbanda O. P., Monga N., Miglani R., Kapila S. Effect of orthodontic forces on cytokine and receptor levels in gingival crevicular fluid a systematic review. Prog Orthod. 2014;15:65. doi:10.1186/s40510-014-0065-6.
CrossRef - Insee K., Pothacharoen P., Kongtawelert P., Ongchai S., Jotikasthira D., Krisanaprakornkit S. Comparisons of the chondroitin sulphate levels in orthodontically moved canines and the clinical outcomes between two different force magnitudes. Eur J Orthod. 2014;36(1):39-46.
doi:10.1093/ejo/cjs109.
CrossRef - Ribagin L. S., Rashkova M. R. Matrix Metalloproteinase-8 And Interleukin-1Β In Gingival Fluid Of Children In The First Three Months Of Orthodontic Treatment With Fixed Appliances. Folia Med (Plovdiv). 2012;54(3):50-56. doi:10.2478/v10153-011-0097-3.
CrossRef - Yamaguchi M., Takizawa T., Nakajima R., Imamura R., Kasai K. The Damon System and release of substance P in gingival crevicular fluid during orthodontic tooth movement in adults. World J Orthod. 2009;10:141-146.
CrossRef - Tzannetou S., Efstratiadis S., Nicolay O., Grbic J., Lamster I. Comparison of levels of inflammatory mediators IL-1beta and betaG in gingival crevicular fluid from molars, premolars, and incisors during rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2008;133(5):699-707. doi:10.1016/j.ajodo.2006.03.044.
- Giannopoulou C., Mombelli A., Tsinidou K., Vasdekis V., Kamma J. Detection of gingival crevicular fluid cytokines in children and adolescents with and without fixed orthodontic appliances. Acta Odontol Scand. 2008;66(3):169-173. doi:10.1080/00016350802123126.
CrossRef - Isik F., Sayinsu K., Arun T., Ünlüçerçi Y. Bone marker levels in gingival crevicular fluid during orthodontic intrusive tooth movement: A preliminary study. J Contemp Dent Pract. 2005;6(2):27-35.
- Yu H. S., Lee K. J., Choi S. H., Park Y. C., Yoo Y. J. Effects of continuous and interrupted orthodontic force on interleukin-1beta and prostaglandin E2 production in gingival crevicular fluid. Am J Orthod Dentofacial Orthop. 2004;125(2):168-177. doi:14765054.
- Grieve W. G., Johnson G. K., Moore R. N., Reinhardt R. A., DuBois L. M. Prostaglandin E (PGE) and interleukin-1 beta (IL-1 beta) levels in gingival crevicular fluid during human orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 1994;105(4):369-374. doi:8154462.
- Tzannetou S., Efstratiadis S., Nicolay O., Grbic J., Lamster I. Interleukin-1beta and beta-glucuronidase in gingival crevicular fluid from molars during rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1999;115(6):686-696. doi:10.1016/S0889-5406(99)70295-7.
CrossRef - Cox C., Nguyen T., Koroluk L., Ko C. C. In-vivo force decay of nickel-titanium closed-coil springs. Am J Orthod Dentofac Orthop. 2014;145(4):505-513. doi:10.1016/j.ajodo.2013.12.023.
CrossRef - Celebi A. A., Demirer S., Catalbas B., Arikan S. Effect of ovarian activity on orthodontic tooth movement and gingival crevicular fluid levels of interleukin-1β and prostaglandin E2 in cats. Angle Orthod. 2013;83(1):70-75. doi:10.2319/012912-78.1.
CrossRef - Smith R. J., Burstone C. J. Mechanics of tooth movement. Am J Orthod. 1984;85(4):294-307. doi:10.1016/0002-9416(84)90187-8.
CrossRef




