Efficacy of Chlorhexidine Varnish In Patients Undergoing Multibracketfixed Orthodontic Treatment: A Controlled Clinical Study
1Consultant Orthodontist 602 Sinchan A wing, New Link Road Andheri west. Opposite star bazaar. 400053, Mumbai.
2Department of Orthodontics and Dentofacial Orthopedics Manipal College of Dental Sciences, Manipal University Mangalore Karnataka, India.
3Consultant Orthodontist, Jaipur, Rajasthan.
DOI : http://dx.doi.org/10.13005/bpj/1452
Download this article as:
![]()
During fixed orthodontic treatment, maintenance of a good gingival health is challenging. This necessitates use of prophylactic measures, such as use of fluoridated tooth pastes and application of varnish. Use of chlorhexidine (CHX) varnish, is believed to reduce the bacterial count and have a longer duration of action, by virtue of sustained release. Therefore, the aim of the present study is to assess the clinical effects of chlorhexidine varnish (Cervitec plus) on plaque accumulation and gingival health during multibracketorthodontic treatment.
KEYWORDS:Chlorhexidine Varnish; Gingival Health; Orthodontics; Plaque
Introduction
Maintenance of periodontal health plays an important role in post orthodontic treatment stability and is important to prevent any relapse. Even after maintaining a good oral hygiene, new carious lesions can develop in adolescents undergoing orthodontic treatment.1Orthodontic appliances consist of bands, wires and ligatures, making it difficult for patients to maintain acceptable oral hygiene and thus, leading to periodontal problems due to the inherent irregularities of the fixed orthodontic appliances.2,3
Preventive measures that do not require the compliance of the patient are believed to be more appropriate for adolescents undergoing orthodontic treatment. Plaque accumulation can be reduced, and gingival health thus can be improved by using chlorhexidine in the form of gels or varnishes rather than rinsing solutions.5,6 The use of varnish avoids the undesirable effects of CHX, such as altered taste, extrinsic staining of the enamel. Low bacterial activity, maintenance of oral flora balance, excellent absorption by the enamel surface and good tolerance by patients are expected. The sustained release of chlorhexidine and prolonged contact of the varnish on the teeth has been suggested to enhance the antibacterial activity of chlorhexidine varnish.7,8
This study aims to assess the clinical effects of chlorhexidine varnish (Cervitec plus) on plaque accumulation and gingival health duringmultibracketorthodontic treatment.
Materials and Methods
A controlled clinical study design was adopted for this comparative study. In this prospective study, 26 patients in the age group of 12 to 18 years requiring orthodontic treatment were analyzed, based on the following subject inclusion criteria.
Inclusion criteria:
All patients were in the age group of 12 to 18 years.
Cases planned for fixed orthodontic treatment were included in the study.
Exclusion criteria:
History of or presence of any underlying systemic disease.
Patients with on medication, such as for asthma, epilepsy or any form of hypersensitivity.
Patients with previous history of orthodontic treatment were not included in the study.
Patients with poor gingival/periodontal index before the treatment. Also, any history of use of chlorhexidine as toothpaste or mouthwash in last one month for a period of 2 weeks or more.
Prior to the start of orthodontic treatment, all patients were given oral hygiene instructions and were asked to brush using modified bass technique.9,10 Informed consent was taken from every patient (and/or patient’s guardian) prior to the start of the study.
Chlorhexidine (CHX) varnish – Cervitec plus containing 1% chlorhexidine and 1% thymol, manufactured by IvoclarVivadent – Schaan Liechtenstein was used in this study.
To limit the number of variables, the study was designed as a split mouth comparison. To allow effective comparison in all quadrants of the oral cavity, patients were randomly allocated, using a lottery method into two equal groups of thirteen each. [figure 1] Two quadrants were designated as the test and the other two quadrants in both the groups were used as control. Patients were followed at a monthly interval for a period of 6 months at a four weeks interval.
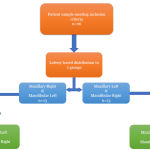 |
Figure 1
|
The principal investigator was blinded during randomization to avoid bias during result assessment.
The application of varnish was done using a stringent protocol. After bonding and banding, the oral cavity was dried using cotton rolls and a cheek retractor was used to keep the labial and buccal mucosa away. Cervitec plus varnish (IvoclarVivadentSchaan Liechtenstein) containing 1% chlorhexidine and 1% thymol was applied to the teeth up to premolar, of all the patients, in the two groups. Three drops of Cervitec plus varnish were added in the dappen dish. An applicator tip was used for the application of varnish, with new replaced tip for every application appointment. After 60 seconds the cotton rolls were removed. Patient was asked not to drink or eat anything for the next one hour. Varnish application was applied twice during the study, once at the initial visit after the bonding and banding procedure, and once after 12 weeks.
Plaque index by Sillness and Loeand gingival index by Loe and Silness22 were evaluated at the start of treatment and then every four weeks for a period of 6 months. The data was recorded on three surfaces of the tested teeth i.e. mesial, distal and buccal by single operator.
Statistical Analysis
Statistical analysis was performed using SPSS20 for windows release software. The values obtained for the chlorhexidine and control group were compared using individual Students T Test.
Results
The gingival score and the plaque score for chlorhexidine group at the start of treatment was 1.25±0.48 and 1.27±0.48 respectively and at the end of 6 months was 1.03±0.40 and 1.08±0.40 respectively whereas the gingival and plaque score for control group at the start of treatment was 1.25±0.47 and 1.26±0.44 respectively and at the end of 6 months was 1.26±0.40 and 1.33±0.42 respectively. The difference in the 4-weekly gingival index and plaque index scores for the control and chlorhexidine group did not show any statistical significance for the first four follow up visits, but difference in the gingival score and plaque score for the two groups was statistically significant for the fifth and sixth follow up visits as shown in Table 1 and Table 2. The comparison can be appreciated stage wise in the figure 2 and figure 3, for plaque and gingival index respectively.
Table 1: Comparison of Gingival Index scores between the Chlorhexidine and control group at each interval
| TIME INTERVAL (months) | CHLORHEXIDINE GROUP ( n =26) | CONTROL GROUP (n=26) | P VALUE |
| 0 | 1.25 ± 0.48 | 1.25 ± 0.47 | 1 |
| 1 | 1.26 ± 0.51 | 1.33 ± 0.48 | 0.568 |
| 2 | 1.19 ± 0.49 | 1.36 ± 0.49 | 0.183 |
| 3 | 1.14 ± 0.45 | 1.34 ± 0.49 | 0.129 |
| 4 | 1.09 ± 0.45 | 1.32 ± 0.46 | 0.061 |
| 5 | 1.06 ± 0.42 | 1.30 ± 0.42 | 0.032* |
| 6 | 1.03 ± 0.40 | 1.26 ± 0.40 | 0.038* |
* = p value < 0.05 = statistically significant
Table 2: Comparison of Plaque Index scores between the Chlorhexidine and control group at each interval
| TIME INTERVAL (months) | CHLORHEXIDINE GROUP ( n =26) | CONTROL GROUP (n=26) | P VALUE |
| 0 | 1.27 ± 0.48 | 1.26 ± 0.44 | 1 |
| 1 | 1.31 ± 0.51 | 1.39 ± 0.51 | 0.572 |
| 2 | 1.26 ± 0.4 | 1.42 ± 0.52 | 0.249 |
| 3 | 1.16 ± 0.45 | 1.4 ± 0.52 | 0.096 |
| 4 | 1.13 ± 0.45 | 1.4 ± 0.49 | 0.052 |
| 5 | 1.10 ± 0.42 | 1.37 ± 0.45 | 0.033* |
| 6 | 1.08 ± 0.40 | 1.33 ± 0.42 | 0.035* |
*= p value < 0.05 = statistically significant.
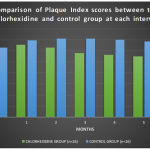 |
Figure 2
|
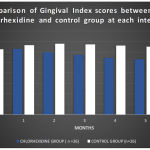 |
Figure 3
|
There was a significant reduction in the gingival and plaque scores at 3 and 6 months after the first visit as compared to the baseline value in the chlorhexidine group. On the other hand, control group showed an increase in the gingival and plaque scores at 0-3 and 0-6months interval. There was no significant reduction in gingival scores between 3 and 6 months in test group.
Discussion
In this prospective controlled clinical study, the effects of chlorhexidine varnish on plaque accumulation and gingival health were assessed in patients undergoing multibracket fixed orthodontic treatment.
Balanyk et al.,7 in a study found that due to first order kinetics, chlorhexidine varnish was effective for a longer period of time and showed that chlorhexidine was effective for atleast 12 days after its application. In first order release kinetics the rate of release diminishes exponentially with time as the concentration of the drug in the core of the matrix decreases. Since the rate of release is not constant this kinetics are called as “sustained release”. Schaekenet al11 used 50% chlorhexidine and found a high rate of chlorhexidine release on first 3 days which declined thereafter. Huizinga et al.,12 found greater sustained release of antimicrobial agents when combination of chlorhexidine and thymol was used as compared to only chlorhexidine. In another study Rahmathulla Khan et al.,13 showed that one application of chlorhexidine varnish was effective in reducing plaque accumulation and thereby improving gingival health for 3 months.
As compared to the test group, the plaque and gingival scores for the control group increased during first 3 months, after which there was a reduction in these values till 6 months. Even though there was slight reduction in the plaque and gingival scores between 3rd and 6th months, the control group the scores for both gingival and plaque indices remained higher than the baseline value at the end of 6 months. This finding on the control side corresponded with Zachrissonet al.,14 and Alexander SA et al.,15 whose results also concluded an increase in plaque and gingival index during orthodontic treatment.
In this study, the test group showed a significant reduction in the gingival scores 3 and 6 months after the first visit as compared to the baseline value. On the other hand, control group showed an increase in the gingival scores at 0-3 and 0-6 months interval. This finding agreed with the study findings of Laurie Brightman et al.,16 in which the results showed greater reduction in the occurrence of gingivitis from baseline to 3 months in the chlorhexidine group than in the placebo group when a 0.12% chlorhexidine mouth rinse was used in orthodontic patients. Also, the reduction in plaque scores were similar to the present study. Segretoet et al.,17 found an average of 28% reduction of gingivitis in a 3-month study. Grossman et al.,18 in a six month follow up study found decrease in gingival occurrence averaged 29% after 3 months and 37% at the end of 6 months. Ousehalet al.,19 found reduction in plaque and gingival scores on using a dentifrice containing 0.12% chlorhexidine gluconate mouthrinse.
EkateriniPaschos et al.,20 studied the effect of chlorhexidine varnish on gingival health in orthodontic patients and measured plaque and gingival indices along with pocket depth for a total of 24 weeks and found significant reduction in plaque and gingival scores at end of 24 weeks. Rahmathulla Khan et al.,13 showed that one application of chlorhexidine varnish was effective in reducing plaque accumulation and thereby improving gingival health for 3 months. These observations were in accordance to the results achieved in the present study.
However, a contrasting observation was reported by Ogaardet al.,21 where no significant difference in visible plaque index and gingival bleeding index, after a follow up of 24 weeks in orthodontic patients, was seen.
In this study,only plaque and gingival indices were scored to assess the gingival health of the patient. For complete status analysis of the gingiva and periodontium, CPI-TN and Gingival bleeding index can be conducted in addition to presently carried measurements.
Conclusion
Chlorhexidine varnish brought about both significant reduction in gingival and plaque index scores over a period of 6 months when compared to the control.
Second application of varnish did not bring about significant reduction in gingival and plaque scores when compared to control group.
Reference
- Zachrisson BU. Fluoride application procedures in orthodontic practice, current concepts. AngleOrthod. 1975;45:72-81.
- Lundstrom F, Hamp SE. Effect of oral hygiene education on children with and without subsequent orthodontic treatment. Scand J Dent Res. I980;88:53.9.
- Lundstrom F, Krasse B. Streptococcus mutans are frequently in orthodontic patients, the effect of chlorhexidine treatments. Eur J Orthod. 1987;9:109-16.
CrossRef - Lee S.M, Yoo S.Y, Kim H.S, Kim K.W, Yoon Y.J, Lim S.H, Shin HY, Kook J.K. Prevalence of putative periodontopathogens in subgingival dental plaques from gingivitis lesions in Korean orthodontic patients. J Microbiol. 2005;43:260–265.
- Olympio KP, Bardal PA, de Bastos M Jr, Buzalaf MA. Effectiveness of a chlorhexidine dentifrice in orthodontic patients: a randomized-controlled trial. J ClinPeriodontol. 2006;33:421–426.
CrossRef - Yucel-Lindberg T, Twetman S, Skold-Larsson K, Modeer T. Effect of an antibacterial dental varnish on the levels of prostanoids, leukotriene B4, and interleukin-1 beta in gingival crevicular fluid. ActaOdontol Scand. 1999;57:23–27
CrossRef - Balanyk T.E, Sandham H.J. Development of sustained-release antimicrobial dental varnishes effective against Streptococcus mutans in vitro. J Dent Res. 1985;64:1356–1360.
CrossRef - Pienihakkinen K, Soderling E, Ostela I, Leskela I, Tenovuo J. Comparison of the efficacy of 40% chlorhexidine varnish and 1% chlorhexidine-fluoride gel in decreasing the level of salivary mutans streptococci. Caries Res. 1995;29:62–67.
CrossRef - Nassar P.O,Bombardelli C.G, Walker C.S, Neves K.V, Tonet K, Nishi R.N, Bombonatti R, Nassar C.A Periodontal evaluation of different toothbrushing techniques in patients with fixed orthodontic appliances. Dent Press J Orthod. 2013;18(1):76-80.
CrossRef - M PoyotoFerrera, J.J Segura-Egea. Comparison of modified bass technique with normal tooth brushing practices for efficacy in supragingival plaque removal. Int J Of Dent Hygiene. 2003;1;110-114.
CrossRef - Schaeken M.J, van der Hoeven J.S, Hendriks J.C. Effects of varnishes containing chlorhexidine on the human dental plaque flora. J Dent Res. 1989;68:1786-1789.
CrossRef - Huizinga E. D, Ruben J. L, and Arends J. Chlorhexidine and thymol release from a varnish system. Journal de BiologieBuccale. 1991;19;343–348.
- Rahamathulla Khan, Verdine Virginia Antony. A randomized clinical trial evaluating the efficacy of chlorhexidine varnish on streptococcus mutans in plaque and gingival status in patients undergoing orthodontic treatment. The Orthodontic Cyber Journal.
- Zachrisson S, Zachrisson B.U. Gingival condition associated with orthodontic treatment. Angle Orthod. 1972; 42:26-34.
- Alexander SA et al., Effects of orthodontic attachments on gingival health of permanent second molars. AJODO.1991;100(4):337-40.
- Brightman L.J, Terezhalmy G.T, Greenwell H, Jacobs M, Enlow D.H. The effects of a 0.12% chlorhexidine gluconate mouthrinse on orthodontic patients aged 11 through 17 with established gingivitis. Am J OrthodDentofacialOrthop. 1991;100:324–329.
CrossRef - Segreto V.A, Collins E.M, Beiswanger B.B, et al., A comparison of mouthrinses containing two concentrations of chlorhexidine. J Periodont Res 1986;21:23-32.
CrossRef - Grossman E, Reiter G, Sturzenberger OP, et al., Six month study of the effects of a chlorhexidine mouthrinse on gingivitis in adults. J Periodont Res. 1986;21:33-43.
CrossRef - Ousehal L, Es-Said R, Hamdoune H, Elquars F, Khadija A. Evaluation of dental plaque control in patients wearing fixed orthodontic appliances: a clinical study. IntOrthod. 2011;9(1):140-55.
CrossRef - Ekaterini Paschos, Mirjam Limbach, Marion Teichmann, Karin C. Huth, Matthias Folwaczny, Reinhard Hickel, Ingrid Rudzki-Janson. Orthodontic Attachments and Chlorhexidine-Containing Varnish Effects on Gingival Health. Angle Orthodontist.2008;78;5.
CrossRef - Ogaard B, Larsson E, Glans R, Henriksson T, Birkhed D. Antimicrobial effect of a chlorhexidine-thymol varnish (Cervitec) in orthodontic patients: a prospective, randomized clinical trial. J OrofacOrthop. 1997;58:206–213.
- Löe H. The gingival index, the plaque index and the retention index systems. Journal of periodontology. 1967;38(6 Part II):610-6.
CrossRef




