
Parithimar kalaignan1 , Jaya Shree Mohan1 and Arun Jayakumar2
, Jaya Shree Mohan1 and Arun Jayakumar2
1Department of Prosthodontics, Vinayaka missions Sankarachariyar dental college, Salem.
2Department of Prosthodontics, Karpaga Vinayaga institute of dental Sciences Kancheepuram.
Corresponding Author E-mail: parithisiva@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1421
Abstract
To establish a definitive grading system & derive classification of maxillary &mandibular tori based on shape . A cluster sample of 72 patients who sought treatment at the dental college with maxillary and/or Mandibular tori were selected, alginate impression were made for each patient and the stone casts poured were evaluated based on the following criteria; shape, prominence and dimensions (length, width, height) to surface a new grading system for the tori. From a total sample size of 72 patients with tori, 38 (52.8%) patients were dentulous (either fully or partially dentulous), and remaining 34 (47.2%) patients were edentulous. A total of 5 patients only had both maxillary and mandibular tori simultaneously present at the time of inspection, while all other 67 patients had only maxillary tori. From the 72 patients who presented with torus palatinus, in relation to the tori shape, 10 (13.9%) were flat, 43 (59.7%) were lobular, 16(22.2%) were spindle shaped and only 3 (4.2%) were of nodular shape. From the 5 patients who presented with torus mandibularis, 3 presented with tori of mild prominence, and 2 others presented with a moderately prominent mandibular tori.In relation to torus palatinus dimension, the width of tori varied widely from 4.0mm to 25.0mm, while the length too had a wide variation from 10.0mm to 37.0mm. The height however hadn’t as much variation, ranging from 0.5mm to 5.0mm. A successful grading system was accomplished in relation to maxillary tori and its effect on the prognosis of maxillary denture stability and retention could be determined from this grading system; however this was not successful for mandibular tori due to insufficient sample size of patients in this category. The grading system devised in our study was reasonable for use by dental graduates, though the study had short comings in few aspects that were not looked upon on initiation, it would be a stepping stone towards more research in this field in relation to maxillary and mandibular tori.. From this study, it is anticipated that Prosthodontist can have a precise idea of the tori to prosthesis relationship when faced with such patients in their day to day practice.
Keywords
Grades Tori Mandibular Tori; Palatinus Torus;
Download this article as:| Copy the following to cite this article: kalaignan P, Mohan J. S, Jayakumar A. Determination of Grading for Maxillary and Mandibular Tori- an in Vivo Study. Biomed Pharmacol J 2018;11(2). |
| Copy the following to cite this URL: kalaignan P, Mohan J. S, Jayakumar A. Determination of Grading for Maxillary and Mandibular Tori- an in Vivo Study. Biomed Pharmacol J 2018;11(2). Available from: http://biomedpharmajournal.org/?p=20265 |
Introduction
The tori (meaning “to stand out” or “lump” in Latin) are bony exostoses that are formed by a dense cortical bone externally and a limited amount of bone marrow internally, and they are covered with a thin layer of poorly vascularized oral mucosa. They are commonly found on the roof of the mouth (palate) as well as projecting from the lingual borders of the mandible. Studies in relation to maxillary and mandibular tori only initiated a few decades ago, hence the minute amount of resources available on them, as not many studies were also conducted regarding tori, a proper criteria for grading, classification system and exact causative agent of such lesions are not yet established. There are many aetiologies that have been attributed to its development such as masticatory hyper function (bruxism, clenching), stress related factors involving teeth, environmental factors and genetics. Though tori can be multifactorial, studies have shown that genetics played a major role. The prevalence is high among Orientals and Eskimos. Their occurrence is thought to be varied with genders usually tori are asymptomatic in nature, however under certain circumstances they can pose problems. Firstly, if the tori are too large they may interfere with speech and mastication. Eating hard food and food with sharp edges such as potato crisp and candy can traumatize and ulcerate the overlying tori lining mucosa due to its thin and friable nature. Concerns may arise about airway management in some cases as well, because the growths could make it hard to control a patient’s airway in an emergency. Tori can also interfere with radiographic imaging. For example, large palatal tori may obstruct the view of maxillary sinus and may cause difficulties during placement of intra oral films. Next, tori are also known to make denture fabrication difficult. If a denture is to be fabricated over a tori, improper use by the patient can lead to ulceration of the overlying mucosa. The presence of tori reduces the stability of the denture. It may act as a fulcrum point which can lead to rocking of the denture. It also gives a poor peripheral seal especially in maxillary dentures when the palatal tori extends to the posterior palatal seal area. These conditions may require surgical removal of the tori. Despite all the disadvantage, those with tori have an advantage when it comes to bone grafting. Any surgery requiring autogenous bone graft can be obtained from this bony exostosis.
Aims and Objectives
To establish a definitive grading system of maxillary & mandibular tori
To derive a classification of maxillary & mandibular tori based on shape
To assess the prognosis for patient requires removable prosthesis in relation to denture retention and stability, and clinical cases at which these will be compromised
To notify the patient regarding the final denture design and outcome and what to expect in relation to the presence of the tori
Materials and Methods
The materials used in this study include mouth mirror, probe, measuring gauge, metal scale, impression trays (sizes XS- XL), Alginate impression material and Type III dental stone.
A cluster sample of 72 patients who received dental treatment our institution with maxillary and/or mandibular tori were evaluated. Upon receiving consent from the patients, proper tray size selection is carried out for each patient, an alginate impression is made and the cast is poured with type III dental stone. Once set, the casts are retrieved and patient’s tori are assessed in a three dimensional representation.
Criteria Used for Grading of Tori
Several criteria’s will be used to grade the tori, as stated in sequence below. Each criteria was measured from the stone casts of patients with tori and assessed manually, all measurements made using a metal gauge and ruler, and all measurements standardized to the nearest one decimal points in millimetres.
Criteria are based upon:-
Shape of tori
Prominence of the tori
Dimensions of the tori
Shape of Tori
In reference to the shape of the tori, it is of more relevance to torus palatines as compared to torus mandibularis. The diversity of tori shapes were mostly observed in palatine tori, as concluded from previous studies, as the mandibular tori that lie along the lingual border of the mandible is of more constant dome shape or irregular. Based on the shape of torus palatines, the overall outline of the structure of the tori is assessed by visual examination on the tori on the patient’s stone cast, and further graded as one of the following, each with a diagrammatic representation included to aid in identification:-
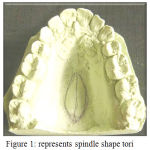 |
Figure 1: represents spindle shape tori
|
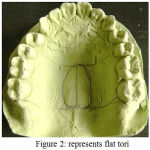 |
Figure 2: represents flat tori
|
 |
Figure 3: represents lobular tori
|
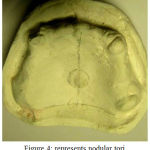 |
Figure 4: represents nodular tori
|
Lobular tori is limited only to multi-lobulated tori. Those with a single lobule are classified under nodular variety. Also, the number of lobules is taken into consideration, for future reference in case of increase in number of nodules.
Prominence of the Tori
Prominence of the tori describes the extent of its convexity at its most prominent points from its area of origin. For this characteristic, the tori are divided into the mild prominence, moderate prominence and very prominent. In general, palatine tori of Flat shapes are usually of mild prominence and those of nodular or lobular types would be very prominent. Prominence is mainly used to assess the mandibular tori protruding from the lingual border of the mandible as one of the three categories described above.Prominence of the tori is assessed visually from the casts although this method is not as accurate, other methods of assessments require more complicated means and hence for ease of assessment, visual method is used.
Dimensions of the Tori
To assess the tori dimensions, the tori are first grouped separately for maxillary tori and mandibular tori.
For Maxillary Tori
Width of Tori
Width of the tori is measured based on the greatest mesio-distal dimension obtained at the point of greatest convexity on the tori, measured in millimeters.
Length of Tori
Length of the tori is expressed as percentage ratio form, which is the greatest antero-posterior length of the tori.
Height of the Tori
Height or vertical dimension of the tori is measured in millimeters from the roof of the palatal vault to the most inferior point of convexity on the tori.
If the tori is lobulated, and multiple lobules of varying vertical heights are present, only the most inferior point of convexity on the most prominent lobule is measured.
For Mandibular Tori
In the case of Mandibular Tori, most commonly patients present with bilateral mandibular tori, however in very rare cases in our sample, certain patients did present with unilateral tori as well.In whichever case presented, both right and left mandibular tori are assessed individually and the mean average of their dimensions are used as reference.
Width of Tori
Width of the tori is measured based on the greatest mesio-distal dimension obtained at the point of greatest convexity on the tori, measured in millimeters.
Length of Tori
The greatest antero-posterior length of the tori is measured in mm.
Height of the Tori
Height or vertical dimension of the tori is measured in millimeters from the floor of the mouth to the most superior point of convexity on the tori, using 2 periodontal probes, one placed vertically from floor of mouth against the tori and the other perpendicular to the first probe at the most superior point of convexity on the tori.
If the tori is lobulated, and multiple lobules of varying vertical heights are present, only the most superior point of convexity on the most prominent lobule is measured. After individual measurements are made from each left and right tori, their mean average values are obtained by addition of both values of a category, and divided by two.2
Results and Observations
From a total sample size of 72 patients with tori, 38 (52.8%) patients were dentulous (either completely or partially dentulous), and remaining 34 (47.2%) patients were edentulous as presented in diagram. 1 A total of 5 patients only had both maxillary and mandibular tori simultaneously present at the time of inspection, while all other 67 patients had only maxillary tori. All patients with mandibular tori presented a bilateral lesion, none presented with unilateral torus mandibularis. Also, no patients presented during the time of study with only mandibular tori in the absence of maxillary tori. From the 72 patients who presented with maxillary tori, in relation to the tori shape, 10 (13.9%) were flat, 43 (59.7%) were lobular, 16(22.2%) were spindle shaped and only 3 (4.2%) were of nodular shape as shown in (diagram 2). From the five patients who presented with mandibular tori, three presented with tori of mild prominence, and two others presented with moderately prominent mandibular tori as shown in (diagram 3). In relation to torus palatinus dimension, the width of tori varied widely from 4.0mm to 25.0mm, while the length too had a wide variation from 10.0mm to 37.0mm. The height however hadn’t as much variation, ranging from 0.5mm to 5.0mm, with only one odd exception having a height of 8.0mm.
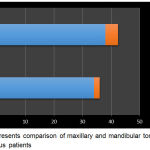 |
Graph 1: represents comparison of maxillary & mandibular tori in dentulous and edentulous patients
|
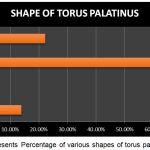 |
Graph 2: represents Percentage of various shapes of torus palatinus
|
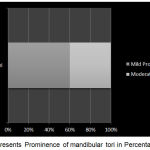 |
Graph 3: represents Prominence of mandibular tori in Percentage
|
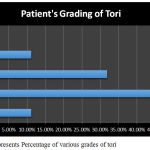 |
Graph 4 represents Percentage of various grades of tori
|
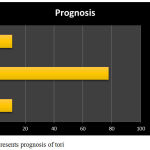 |
Graph 5: represents prognosis of tori
|
Discussion
In the past, few studies have ventured into the various aspects in regards to the topic of Torus (Tori) in the oral cavity as compared to most other oral conditions. Many previous studies mainly dealt with identifying common locations of these bony projections in the oral cavity and their origin and components being a structured form of compact bone with cancellous bony substructure.17,19,22 Oral tori have been defined as slow growing, osseous outgrowths at the midline of the hard palate and at the lingual surfaces of the mandible.6,20 In the mandible the tori can be bilateral or unilateral, usually in the premolar regions but infrequently also at the genial tubercles.4 The torus is considered a developmental anomaly and has been termed an exostosis, a benign hyperplastic overgrowth of the bony surface to differentiate it from a true neoplasm.5 It presents either as a smooth bulging of the bone surface continuous with the adjacent area or as discrete, multilocular spherical projections with a broad base that forms a nodular cluster.5,20
Much of the subsequent era of studies in relation to tori were done to identify specific populations in which these tori were associated a great deal with, tracing back anthropologically the genetic inheritance patterns associated with both torus palatinus and torus mandibularis.1,2,3,4,8,9,11,13,14,17,18 Tori have been consistently shown to be more frequently seen in the mongoloids than in the caucasians.9,24 Costich.8 speculated that tori may be less common in blacks than in whites. J.O. Agbaje et. Al.13 confirmed this view as a low prevalence rate of 3.74% of torus palatinus and /or mandibularis in the Nigerian population, a lower rate of 1.8% and 2.5% were calculated for torus palatinus and torus mandibularis respectively. Previous reports in mongoloid and Caucasian races showed higher rates.8, 12,24 Haugen.12 found a rate of 9.2% torus palatinus and 7.2% torus mandibularis in a Norwegian population. Yaacob et al.24 found a high rate of 24.4% of torus palatinus in Malaysian but low prevalence of torus mandibularis 2.2%.
The prevalence of torus palatinus is more common in females,12,14,15,19 but contrast with findings that torus mandibularis is more common in males.10,12,14,18,19 J.O. Agbaje et. al.13 stated that females were 2.0 times as likely to have torus palatinus as males and,3,2 times as likely to have torus mandibularis as males. Haugen,12 stated that there was no obvious explanation for the gender differences but suggested genetics as a responsible factor. J.O. Agbaje et. Al.13 stated that among Negroids, Torus mandibularis was more popular, even in the absence of torus palatinus, many patients still presented with torus mandibularis, which is contrast to the Caucasian and Mongoloids which presented mostly with torus palatinus and rarely torus palatinus with torus mandibularis as well, but never torus mandibularis as an isolated finding.
Previous studies were also done in relation to the peak age as which tori was a common occurrence, investigators reported a peak of occurrence of tori in the third decade of life.2,16 J.O. Agbaje et. Al.13 stated a peak of occurrence of both tori in the fifth decade. In our study, most patients presented with tori were in their 4th and 5th decades on life, consistent with findings of previous studies that the prevalence of tori tends to increase with age up to peak age group 40-49years. However, a trend for decreasing the occurrence of both tori was noted from the 50-59 year age group to the older age group this is in accordance with finding by previous authors.5,9,23 This variation in prevalence, therefore, should be influenced by functional factors. The regression of torus palatinus was probably observed after the extraction of teeth. Eggen &Natvig.10 reported the similar result in Norwegians and surmised that decreased prevalence of torus mandibularis among persons over 50 years of age was related to the decrease in number of remaining teeth. Sonnier et al.19 stated that the prevalence of torus mandibularis was directly related to the presence of teeth. Wandee et al.23 stated that functional influences may contribute to the clinical expression of torus palatinus and torus mandibularis. Eggen & Natvig ,10 have also correlated the high prevalence of torus mandibularis with increased masticatory stress.
The occurrence of tori can be considered as a dynamic phenomenon, responding during life to environmental and functional factors that act in a complicated interplay with genetic factors. Tori appears in various shapes. Up to now, there are no definitive classifications for torus palatinus and torus mandibularis. In general, all tori in the maxilla are called Palatal Tori , and those along the lingual border of mandible are referred to as Mandibular Tori. They are also grouped according to their shape as flat, nodular, lobulated and spindle. Their location can be grouped as premolar region, molar region, premolar to molar region, incisor to premolar region and incisor to molar region. Kolas .16 classified them according to number of nodes and their placement as bilateral single, bilateral multiple, unilateral single and unilateral multiple. Where size is concern, there are only two known classifications so far, based on Haugen’s .12 and Reichart’s.18 Haugen’s .12 classified tori into less than 2 mm in their largest diameter as considered as small, 2 – 4 mm in their largest diameter as considered as medium and more than 4 mm in their largest diameter as considered as large. Reichart,18 in his modification of Haugen’s,12 classification suggested few changes : Grade I – Tori up to 3 mm in their largest dimension, Grade II – Tori up to 6 mm in their largest dimension and Grade III – Tori above 6 mm belong to this group.
For grading the tori in our study we categorized the tori dimensions as below:-
Maxillary Tori
For each category (length, width and height) of tori, numbering from 1,2,3,4,5 were designated to a range of values for each of the measurements, and separately for each category. The total final grading was in a three numerical format. An example is given below:-
Table 1: shows an average width of various grades of tori
| Grading | Average Width (mm) |
| Grade I | <10.0 |
| Grade II | 10.0-15.5 |
| Grade III | 16.0-20.5 |
| Grade IV | 21.0-25.5 |
| Grade V | >26.0 |
Table 2: shows an average length of various grades of tori
| Grading | Average Length (mm) |
| Grade I | <18.0 |
| Grade II | 18.0-25.5 |
| Grade III | 26.0-32.5 |
| Grade IV | 33.0-37.5 |
| Grade V | >38.0 |
Table 3: shows an average height of various grades of tori
| Grading | Average height (mm) |
| Grade I | 0.5-1.0 |
| Grade II | 1.5-2.0 |
| Grade III | 2.5-3.0 |
| Grade IV | 3.5-4.0 |
| Grade V | >4.0 |
Table 4: shows prognosis of various grades of tori
| Prognosis | Final Grading of tori |
| Good | Grade 1 |
| Moderate | Grades 2 & 3 |
| Poor | Grades 4 & 5 |
Grading of this patient’s tori would be grade 3 for width, grade 3 for length and grade 3 for height. This grading system will then be written as 3.3.3.
The corresponding prognosis in relation to denture stability and retention was then determined for each of the final grades of the tori from the highest grading obtained between length and width. Example, for the patient above, the final grading of tori in relation to prognosis would be Grade 3.
In another cited example, from the data list:-
Grading for this patient would be written as 4.4.5. The final grading in relation to prognosis for this patient would be Grade 4. (Although a grade of 5 was given for height, we correlated in our study that “height” of tori had least effect on denture retention and stability in terms of the amount of denture base reduction in the area that would be required, as compared to “height” and “width” of the tori. Hence, the largest grade between width and length only is considered to make the final grading in relation to prognosis.)
From the study, we found it inappropriate to include the shape of tori into the grading system above, since the shape of the tori is subjective in relation to its dimensions, there was no specific pattern to justify certain shapes of tori occurred only with certain definite dimensions, any shape of tori could present with a wide range of sizes, either small or large. Hence, it was more appropriate to state the shape of the tori as a separate entity in the patient’s case sheet followed by grading it based on its dimensions.
Based on this grading, in our study we found that 8 (11.1%) patients had Grade I tori, 33 (45.9%) had Grade II tori, 23 (31.9%) had Grade III tori and 8 (11.1%) had Grade IV tori from the sample of 72 patients as shown in (diagram 4) We did not come across any patients with grade V tori in our study. A similar grading system for mandibular tori could not be done due to a very minute sample size that we obtained from our sample of patients.
Prognosis Based on the Grading System Devised
Denture Prognosis is an opinion or judgment given in advance of treatment for the prospects for success in the fabrication of dentures and their usefulness.
In this study, the term prognosis is based on three factors of consideration; the amount of stability and retention of a removable prosthesis that would be compromised by the presence of the tori, the chance of ulceration of the overlying mucosa of the tori if relief were not to be given over the tori area, and the aspect of surgical removal of tori and under which circumstances this should be necessary.
The prognosis devised for each patient is assessed from the final grading of the patient’s tori, as was mentioned previously. The prognosis derived from our grading system is as shown in Table 4.
A good prognosis indicates that stability and retention of the denture is not or very minimally affected by the presence of the tori. The denture base may be allowed to cover the mucosal area over the tori and there would be absence of any ulceration of the thin overlying tori epithelium. There is expected to be none or mild patient discomfort with the denture base extending over the tori of this size, in which case the operator should make a choice whether to give relief or not, depending on the severity of patient complaints.
*One may debate that a grade 5 tori height might cause tori ulceration. It must be emphasized that to have a grade 4 and above tori height with grades 0 & 1 of tori width and length is quite impossible as tori, despite having multiple forms, most certainly does not grow vertically.
A Moderate prognosis indicates that the stability and retention of the denture is compromised to a certain extent, but it can still be acceptable and functional without having the denture falling off or rocking in the oral cavity upon masticatory function. Denture base should not cover the tori for such cases as doing so may result in ulceration of the tori epithelium most certainly to a greater degree than before resulting in severe patient discomfort. Such tori are always questionable when it comes to the need for surgical removal, mostly these do not require so unless the operator has justifiable reasons to do so otherwise in relation to other factors like patient comfort, and esthetics quite rarely.
A Poor prognosis indicates a very large tori occupying a large area of the palate. Regardless of the shape of the tori, stability and retention of the denture is severely compromised due to the large amounts of relief of denture base often required for this category. These tori should never be covered by the denture base as continuous movements will result in ulceration and severe pain. Patient should be advised on this situation and that denture adhesives may not help much in securing the denture in the mouth due to lack of denture base area. Surgical removal of this group of tori is advocated here. In old patients who cannot undergo such a procedure, they may be willing to accept the denture of poor retentive qualities. Problems associated with this kind of denture prognosis should be clearly explained to the patient before fabricating one to avoid disappointments at delivery.
Based on these criteria, in our study we found that 8 (11.1%) patients had a good prognosis, while 55 (77.8%) patients had a moderate prognosis and 8 (11.1%) had poor prognosis of their prosthesis in relation to the tori as shown in (diagram 5).
There were some limitations to our study as stated below:-
Random walk-in patients in the dental clinic who presented with tori only were selected, and many patients with tori were missed out due to time factor for patients requiring treatments at respective departments and some patients refused consent on the basis of having pain and other symptoms at that point of time, and others who did not return for subsequent visits.
During the study, the ratio of dentulous to edentulous patients were about equal, however it was not certain as to the relationship of masticatory force difference between both groups of patients and their tori which was questionable
The severe lack of sample size in relation to mandibular tori was due to improper impression making technique in the lower arch, as most mandibular tori’s appeared much larger clinically than was represented on the casts, making analysis not very accurate.
Conclusion
The grading system devised in our study was reasonable for use by general dentist, though the study had shortcomings in few aspects that were not looked upon on initiation, it would be a stepping stone towards more research in this field in relation to maxillary and mandibular tori. From this study, it is anticipated that Prosthodontist can have a precise idea of the tori to prosthesis relationship when faced with such patients in their day to day practice.
References
- Ruprecht A, Hellstein J, Bobinet K and Mattinson C. The prevalence of radiographically evident mandibular tori in the University of Iowa dental patients. Dentomaxillo facial Radiology. 20002;9:291-296.
CrossRef - Austin J. E, Radford G. H, Banks S. O, Palatal J . r. and mandibular tori in the negro. N. Y. State Dent. J. 1965;31:187-191.
- Bernaba J, Morphology M and Incidence of Torus Palantinus and Mandibularis in Brazilian Indians. J. Dent. Res. 1977;56:499-501.
CrossRef - Bernal B. A, Moreira D. E, Rodriguez P. I. Prevalence of Torus Palatinus and Torus Mandibularis in the City of Havana. Rev. Cubana Estomatol. 1983;20:126-131.
- Bruce I, Ndanu T. A, Addo M. E. Epidemiological Aspects of Oral Tori in a Ghanaian Community. Int. Dent. J. 2004;54:78-82.
CrossRef - Carl O.B. Current Clinical Dental Terminology; The C.V. Mosby Company: Saint Louis.1974;411-412.
- Chew C. L, Tan P. H. Torus Palatinus. A Clinical Study. Aust. Dent. J.1984;29:245-248.
CrossRef - Costich E.R, Comment on Summer C.J. Prevalence of Tori. J. Oral Surg. 1968;718-720.
- Dosumu O.O, Arotiba J.T, Ogunyinka A.O. The Prevalence of Palatine and Mandibular Tori in a Nigerian Population. Odonto- Stomatologie Tropicale. 1998;6-8.
- Eggen S, Natvig B. Variation in Torus Mandibularis Prevalence in Norway. A Statistical Analysis Using Logistic Regression. Community Dent. Oral Epidemiol.1991;19:32-35.
CrossRef - Gorsky M, Raviv M, Kfir E, Moskona D. Prevalence of Torus Palatinus in a Population of Young and Adult Israelis. Arch. Oral Biol. 1996;41:623-625.
CrossRef - Haugen L. K. Palatine and Mandibular Tori. A Morphologic Study in the Current Norwegian Population. Acta Odontol. Scand. 1992;50:65-77.
CrossRef - Agbaje O, Arowojolu1 M.O, Kolude B, Lawoyin J.O. African. Qualitative Study; Torus Palatinus and Torus Mandibularis in a Nigerian Population. Journal of oral Health.2005;2:30-36.
- Kerdpon D, Sirirungrojying S. A. Clinical Study of Oral Tori in Southern Thailand: Prevalence and the relation to Parafunctional Activity.Eur. J. Oral Sci.1999;107:9-13.
CrossRef - King D. R, Moore G. E. An Analysis of Torus Palatinus in a Transatlantic Study. J. Oral Med.1976;31:44-46.
- Kolas S, Halperin V, Jefferis K , Huddleston S, Robinson H. B. The Occurrence of Torus Palatinus and Torus Mandibularis in 2,478 Dental Patients. Oral Surg. Oral Med. Oral Pathol.1953;6:1134-1141.
CrossRef - Ossenburg N.S, Mandibular Torus A. Synthesis of New and Previously Reported Data and Discussion of Its Causes. Ottawa. 1981;1-52.
- Reichart P. A, Neuhaus F, Sookasem M. Prevalence of Torus Palatinus and Torus Mandibularis in Germans and Thai. Community Dent. Oral Epidemiol.1988;16:61-64.
CrossRef - Sonnier K. E, Horning G. M, Cohen M. E. Palatal Tubercles, Palatal Tori, and Mandibular Tori: Prevalence and Anatomical Features in a U.S. Population. J. Periodontol.1999;70:329-336.
CrossRef - Stephen T. S, Robert C. F, Leslie F. Principle and Practice of Oral Medicine; W.B. Saunders Company: Philadelphia. 1984;476-477.
- Summers C. J. Prevalence of Tori. J. Oral Surg.1968;26:718-720.
- Topazian D. S, Mullen F. R. Continued Growth of a Torus Palatinus. J. Oral Surg.1977;35:845-846.
- Wandee A, Aree J, Somporn S . Torus Palatinus and Torus Mandibularis in a Thai Population. Science Asia. 2002;28:105-111.
CrossRef - Yaacob H, Tirmzi H, Ismail K.The Prevalence of Oral Tori in Malaysians. J. Oral Med. 1983;38:40-42.

