
Manuscript accepted on :August 28, 2017
Published online on: --
Plagiarism Check: Yes
N. Raj Vikram1, Ramachandra Prabhakar2, S. Aravind Kumar3, M. K. Karthikayan2, R. Saravanan2, K. S. Nagachandran4, S. karthik4 and V. Anbu2
1Research Scholar, Thai Moogambigai Dental College And Hospital, Dr.Mgr Educational Research Institute University, Chennai.
2Department of Orthodontics Thai moogambigai Dental college and hospital Chennai, Tamil nadu, India.
3Department of Orthodontics Saveetha Dental college and hospital Chennai, Tamil nadu, India.
4Department of orthodontics Meenakshi ammal dental college and hospital Chennai, Tamilnadu, India.
Corresponding Author E-mail: n_rajvikram@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1219
Abstract
A new implant is designed innovatively for the purpose of protracting the maxilla in a growing class III patient. This implant is placed on the maxilla to give a protracting force from the reverse pull head gear without using the occlusal splint. FEM model along the implant is created to analyse the stress and displacement of the maxilla and its structures.
Keywords
Finite element method; Finite element analysis; finite models; dual ball head implant; modified mini implants; stress and displacement of maxilla
Download this article as:| Copy the following to cite this article: Vikram N. R, Prabhakar R, Kumar S. A, Karthikayan M. K, Saravanan R, Nagachandran K. S, karthik S, Anbu V. Fem Models of Cranium Along with Maxilla and Modified Implants to Analyse Stress and Displacement for the Purpose of Maxillary Protraction. Biomed Pharmacol J 2017;10(3). |
| Copy the following to cite this URL: Vikram N. R, Prabhakar R, Kumar S. A, Karthikayan M. K, Saravanan R, Nagachandran K. S, karthik S, Anbu V. Fem Models of Cranium Along with Maxilla and Modified Implants to Analyse Stress and Displacement for the Purpose of Maxillary Protraction. Biomed Pharmacol J 2017;10(3). Available from: http://biomedpharmajournal.org/?p=16531 |
Introduction
System of oral cavity and dentition is similar to biomechanical conditions which are very complicated and the accessibility to it is very restricted. The researches and the study done in oral cavity are mostly in vitro rather than in vivo due to its complicated conditions. This requires a proper method to analyse the condition of stress in a numerical way. The modern tool for this stress analysis which is numerical is Finite Element Analysis (FEA). It has an advantage of being applied to solids of irregular geometry that contain heterogeneous material properties.1 The clear understanding of the interactions and reactions of the structures can be bought about by this numerical technique.2
This FEA solves the biological problem numerically in a mathematical way. FEA was introduced to solve structural problems. Later it was found to be useful in physical problems.3 The structure is made of numerous elements connected through nodes. The procedure of this FEA is to analyse the elements for its strain and stress.4
Retrognathic maxilla or prognathic mandible or the combination is the general features of a skeletal class III malocclusion. The typical condition of the underdeveloped maxilla comes with a deficiency of height or width of its bone or its sagital position5 which needs to be corrected. The toughest part is to correct this underdeveloped maxilla in a growing patient.
Mild to moderate maxillary deficiency can be corrected by protraction head gear in a growing class III individual.6,7
The face mask force is applied via elastics to jaws by the device supported by teeth and or palate. There will be an intra oral device to support the maxillary dentition. It will consist of rapid maxillary expander, a bite in the occlusal area, an arch which runs between buccal to lingual side and hooks to hold elastics to the face mask. These hooks are placed in between lateral incisor and canine.
When maxillary dentition is used as an anchorage, it may result in unwanted side effects. The maxillary molars can get extruded, rotation of palatal plane can occur in counter clock wise direction, incisors can procline or mandible can rotate in a clockwise direction.8-15
To allow the direct transmission of orthopedic force to the circummaxillary sutures, intentionally ankylosed deciduous canines, osseointegrated onplants and implants, and orthodontic miniscrews have been used as skeletal anchorage for maxillary protraction.16-21
Three-dimensional (3D) finite element model analysis can enumerate the biomechanical variables such as stress, strain, and displacement in the maxillofacial complex induced by various conditions of force and direction in maxillary protraction22-26
The purpose of this study is to create a new innovative implant and FEM model to find the stress, strain and displacement of maxillary protraction.
Materials and Methods
New type of mini implant has been designed in 3D CAD software. A 3D printing of that implant has been done.
Computed tomography scan of a skull of a boy aged 9 years has been taken. The boy had typical class III features of retrognathic maxilla and anterior cross bite. The images obtained were horizontal. It was obtained from the superior part of cranium to the maxillary occlusal plane to develop a model.
A normal 3D model was reconstructed with the help of the CT images. Mesh was added to this 3D model to make it a 3D finite element model. This was done using simulation software. All the sutural systems were incorporated to the model. Nodes were placed and elements were developed in the models. 173303 nodes and 621482 elements have been used to build up this 3D FEM model. This helped in identifying the stress and displacement of the points and structures necessary when the orthopaedic force is applied.
Also a new design of mini implant was developed. Initially it was made in a schematic form. Then using CAD diagram 3d schematic form of the mini implant was obtained. Using a 3D printer, the implant was created.
This 3D printed implant is scanned with the photo scanner to insert it in the previously developed 3D finite element model. Two models are created. In the first model implants are placed anteriorly between the lateral incisor and canine on either side. In the second model implants are placed between deciduous first molar and permanent first molar on either side.
Protraction force of 350 grams per side and 500 grams per side are applied to both the models with 100, 200 and 300 with the downward and forward force vector to the maxillary occlusal plane in all the models.
Results
The models are created and are represented in figures.
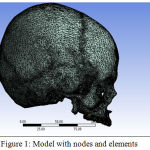 |
Figure 1: Model with nodes and elements
|
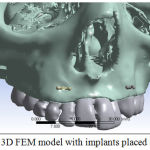 |
Figure 2: 3D FEM model with implants placed anteriorly
|
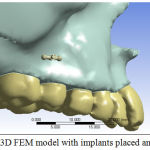 |
Figure 3: 3D FEM model with implants placed anteriorly
|
Stress and displacement of the sutures and the surface landmarks are determined by ANSYS software.
The surface landmarks are identified in four different regions such as maxilla, zygoma, frontal bone and temporal bone.
Six Cranial sutures are considered – fronto –nasal and maxillary, zygomatico – maxillary, temporal and frontal , pterygomaxilary
Discussion
Mini screws were introduced as absolute anchorage devices in orthodontic treatment 27
Biological compatibility by the implants to provide anchorage in animals28-30 and humans31-34 with varying orthodontic forces have been demonstrated. Then the same was proved with orthopaedic force in animals.
Monkeys have been placed with osseointegrated implants and tested for maxillary protraction. It showed good skeletal results. Then many workers proved the efficiency of TAD.
Bone plates and implants which are used in the previous studies have a surgical procedure in placing them. That had a uneasiness to the patient and the wound healing was delayed. There was no implant which can be directly placed and force applied through elastics.
A new design has been innovated to avoid the surgical procedure and to provide comfort to the patient. The new implant is named as dual ball headed mini implant. The parts are as follows:
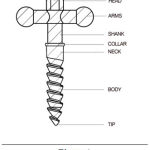 |
Figure 4
|
Parts of Dual Ball Head Implant35
Head
Arms
Shank
Collar
Neck
Body
Tip
Conclusion
With this innovative mini implant and the 3d FEM models, stress and displacement of various structures can be determined from the four regions and six cranial sutures.
Reference
- Geng J. P., Tan K. B., Liu G. R. Application of finite element analysis in implant dentistry a review of the literature. J Prosthet Dent. 2001;85:585-598.
CrossRef - Tanne K., Sakuda M., Charles J. Three dimensional finite analyses for stress distribution in the periodontal tissue by orthodontic forces.Am J Orthod Dentofacial Orthop. 1987;92:499-505.
CrossRef - Basic Concepts of Finite Element Analysis and its Applications in Dentistry: An Overview Mohammed SD and Desai H. oral hygiene and health. 2014;2(5).
- Gallagher R. H. Finite element analysis fundamentals. (4th Edn) Englewood Cliffs: Prentice-Hall. 1975
- Enlow D. H. Facial growth, 3rd Philadelphia,pa: WB saunders. 1990.
- Mcnamara JA. An orthopaedic approach to the treatment of classIII malocclusion in young patients. J clinic Orthod. 1987:21;598-608.
- Baek H. S. Clinical results of the maxillary protraction in Korean children. Am J Orthod Dentofacial Orthop. 1995;158:583-92.
CrossRef - Baek S. H., Yang I. H., Kim K. W., Ahn H. W. Treatment of Class III malocclusions using miniplate and mini-implant anchorage. Semin Orthod. 2011;17(2):98–107.
CrossRef - Itoh T., Chaconas S. J., Caputo A. A.,matas J. photoelastic effects of maxillary protraction on the craniofacial complex. Am J orthod Dentofacial Orthop. 1985;88:117-24.
CrossRef - itoh T. s. H., Nakagawa M., Kamogahira k.,Ichikawa k. l.,Matsumoto M., et al. Biomechanical effects of maxillary protraction on the craniofacial. Am J. Orthod Dentofacial orthop. 1987;91:305-11.
- Chong V. H., IVC J. C., Artun J. Changes following the use of protraction headgear for early correction of class III malocclusion Angle orthod. 1996;66:351-62.
- Ngan P. W Hagg U., Weish i. Treatment response and long term dentofacial adaptations to maxillar expansions and protraction. semin orthod. 1997;3:255-64.
CrossRef - piyiuc N., Hagg U. H., gunel E. W. cephalometric and occlusal changes following maxillary expansion and protraction. Eur J orthod. 1998;20:237-54.
CrossRef - Kapast A. J., Sinclair P. M., Turley P. K. cephalometric effects of facemask expansion therap in class III children a comparison of three age groups. Am J orthod dentofacial orthod. 1998;113:204-12.
CrossRef - Keles A., Tokmak E. C., Ervedi N., Nanda R. Effects of varying the force direction on maxillary orthopaedic protraction. Angle orthod. 2002;72:387-96.
- Kokich V. G., Shapiro P. A., Oswald R., Koskinen-Moffett L., Clarren S. K. Ankylosed teeth as abutments for maxillary protraction: a case report. Am J Orthod Dentofacial Orthop. 1985;88:303-7.
CrossRef - Smalley W. M., Shapiro P. A., Hohl T. H., Kokich V. G., Branemark P. Osseointegrated titanium implants for maxillofacial protraction in monkeys. Am J Orthod Dentofacial Orthop. 1988;94:285-95.
CrossRef - Singer S. L., Henry P. J., Rosenberg I. Osseointegrated implants as an adjunct to face mask therapy a case report. Angle Orthod. 2000;70:253-62.
- . Enacar A., Giray B., Pehlivanoglu M., Iplikcioglu H. Facemask therapy with rigid anchorage in a patient with maxillary hypoplasia and severe oligodontia. Am J Orthod Dentofacial Orthop. 2003;123:571-7.
CrossRef - Hong H., Ngan P., Han G., Qi L. G., Wei S. H. Use of onplants as stable anchorage for facemask treatment. Angle Orthod. 2005;75:453-60.
- Vachiramon A., Urata M., Kyung H. M., Yamashita D. D., Yen S. L. Clinical applications of orthodontic microimplant anchorage in craniofacial patients. Cleft Palate Craniofac J. 2009;46:136-46.
CrossRef - Tanaka O. M., Araújo E. A., Oliver D. R and Behrents R. G. A finite element analysis of the maxillaryfirst molar PDL with maxillary protraction in a mixed dentition Class III malocclusion. Orthod and Craniofac Res. 18(4):240-50.
- Tanne K., Hiraga J., Kakiuchi K., Yamagata Y., Sakuda M. Biomechanical effect of anteriorly directed extraoral forces on the craniofacial complex a study using the finite element method. Am J Orthod Dentofacial Orthop. 1989;95:200-7.
CrossRef - Tanne K., Hiraga J., Sakuda M. Effects of directions of maxillary protraction forces on biomechanical changes in craniofacial complex. Eur J Orthod. 1989;11:382-91.
CrossRef - Tanne K., Matsubara S., Sakuda M. Location of the centre of resistance for the naso-maxillary complex studied in a three-dimensional finite element model. Br J Orthod. 1995;22:227-32.
CrossRef - Vikram R. N., kumar K. S. S., Nagachandran K. S. Y MD Hashir Apical stress distribution on maxillary central incisor during various orthodontic tooth movements by varying cemental and two different periodontal ligament thicknesses: A fem study. Indian J Dent Res. 2012;23:213-20.
CrossRef - Leung M. T., Lee T. C., Rabie A. B and Wrong R.W. Use of mini screws and minip-lates in orthodontics.Journal of oral and maxillofacial surgery. 2008;66;1461-1466.
CrossRef - Hoffman M. S. A new device for absolute anchorage for orthodontics. Am J Orthod Dentofacial Orthop. 1995;107:251-258
CrossRef - Roberts W. F., Smith R. K., Ziberman Y., Mozsary P. G., Smith R. S. Osseous Adaptation to continous loading of rigid endosseous implants Am J Orthod Dentofacial Orthop. 1984;86:95-111.
CrossRef - Gray J. B.,Steen M. E., King G. J.,Clark A. E. Studies on the efficacy of implants as orthodontic anchorage Am J Orthod Dentofacial Orthop. 1983;83:311-317.
CrossRef - Higuchi K. W.,Slack J. M. The use of titanium fixtures for intraoral anchorage to facilitate orthodontic tooth movement. Int J Oral Maxillofac Implants. 1991;6:338-344.
- Roberts W. E.,Smith R. K.,Ziberman Y., Mozsary P. G. Rigid endosseous implant utilized as anchorage to protract molars and close an atrophic extraction site.
- Roberts W. E.,Nelson C. L.,Godacre C. J. Rigid implant anchorage to close a mandibular first molar extraction site J Clin Orthod. 1994;28:693-704.
- Odman J.,Lekholm U., Jemt T., Thilander B. Osseointegrated implants as orthodontic anchorage in the treatment of partially edentulous adult patients. Eur J Orthod. 1994;16:187-201.
CrossRef - Vikram R. N., prabhakar R.,kumar A. S., karthikeyan M. k.,Saravanan R. Ball headed mini implant J Clin Diagn Res. 2017;11(1).

