
Laishram Monisha1 and Waikhom Arvind2
1Orthodontics and Dentofacial Orthopedics.
2Oral and Maxillofacial Surgery.
DOI : https://dx.doi.org/10.13005/bpj/1242
Abstract
The most important question to the clinician is whether it is warranted to extract a single lower incisor in borderline cases. In the present case report, in order to resolve the minor crowding, a lingually placed lower incisor has been extracted and also the soft tissue profile was maintained. Lower incisor extraction is indicated in the carefully selected cases,especially where space requirement do not call for greater dento-alveolar movement.
Keywords
Asymmetric extraction Crowding; Cross Elastics; Lower incisor; Quad Helix;
Download this article as:| Copy the following to cite this article: Monisha L, Arvind W. Wilson Quad Helix Expansion and Uncommon Extraction of Mandibular Incisor: A Case Report. Biomed Pharmacol J 2017;10(3). |
| Copy the following to cite this URL: Monisha L, Arvind W. Wilson Quad Helix Expansion and Uncommon Extraction of Mandibular Incisor: A Case Report. Biomed Pharmacol J 2017;10(3). Available from: http://biomedpharmajournal.org/?p=16255 |
Introduction
The decision to extract permanent teeth as aid in resolving arch length deficiencies presents a challenge to the orthodontist. Few patients are not ideal either for extraction or non extraction.1 Hahn in 1942 advocated the removal of a mandibular incisor to close the extraction space and thus reduce the anterior crowding.2 As pointed out by Kokich and Shapiro (1984), the deliberate extraction of a lower incisor in certain cases allows the orthodontist to improve occlusion and dental a esthetics.2
Tooth-size and arch-length discrepancy, or arch crowding has traditionally been managed by means of first or second premolar extraction. First or second molar extraction is a less common approach. Incisor extraction is another alternative in the mandibular arch. In 1905, Jackson described a case in which two lower incisors were extracted at different times to relieve mandibular crowding.3 According to Proffit, mandibular incisor extraction comprised 20% of all the orthodontic extraction cases in 1950s, but was rarely use thereafter.
Case Report
A 14 years old female reported with the chief complaint of irregular teeth. The patient’s past Medical and Dental history were not contributory. The patient presented with a Orthognathic facial profile, Incompetent lips, Average Mandibular Facial Height (fig. 1)
 |
Figure 1: Pre treatment extra oral photos.
|
Intra oral examination revealed Angle’s Class I molar relationship with mild crowing, constricted upper arch, overjet of 3mm, overbite of 3mm and lingually inclined lower first molars, and average curve of spee.
Carey’sand Arch Perimeter analysis indicates a tooth size-arch length discrepancy of 0.4mm in the maxillary arch and 4mm in the mandibular arch. Bolton’s analysis indicated mandibular anterior tooth material excess of 4mm.
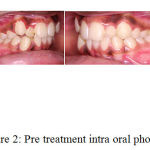 |
Figure 2: Pre treatment intra oral photos.
|
The treatment objectives were to Eliminate crowding in Upper and Lower arches, Upper arch expansion, Uprighting the lower molars and maintaining the Overjet and Overbite, and the acceptable facial profile. Considering the above treatment objectives, it was planned to extract the mandibular right lateral incisor, which would help resolve the lower anterior crowding while maintaining the patient’s soft tissue profile.
Treatment Objectives
Expansion of upper arch
Extraction of lower single incisor
Correction of lingually inclined lower molars
Maintaining the Class I molar relationship
Achieving a competent lip closure
Treatment Plan
Expansion of upper arch with Quad helix.
Extraction of 42
Correction of lingually inclined lower molars with cross elastics.
Treatment Progress
Initially Quad helix was given during the start of the treatment. Quad helix was activated once a month for a period of 4 months. Expansion took place in the upper arch after 4 months. 0.022-inch slot MBT brackets were bonded,0.014 NiTi followed by 0.016 NiTi arch wires were given for aligning the upper and lower arches. After the alignment, the extraction of 42 was done, followed by 0.016 x 0.022 NiTi arch wires for 1 month. Later, 0.017 x 0.025 NiTi arch wires were given in Upper and Lower archers. After placement of these arch wires Quad helix was removed,and Upper arch was consolidated. Lingual buttons were welded to 36 and 46 molar bands and Red cross-elastics were given for correction of lingually inclined molars (36 and 46) along with 0.016 Australian arch wires in Upper and Lower arches for a period of 2 months. After this period of 2 months, the lower molars were uprighted. Later on 0.017 x 0.025 NiTi wires placed in upper and lower arches followed by 0.017 x 0.025 SS wires which was followed by 0.019 x 0.025 SS archwires in upper and lower arches.
 |
Figure 3: Quad Helix.
|
Wire Sequences
0.014 NiTi
0.016 NiTi
0.016 x 0.022 NiTi
0.017 x 0.025 NiTi
0.016 Australian wires with cross elastics
0.017 x 0.025 NiTi
0.017 x 0.025 SS
0.019 x 0.025 SS
Discussion
In 1905, Jackson was the first to advocate extraction of lower incisor to relieve crowding. Extraction of mandibular incisor is a logical alternative that may improve the dental occlusion and dental aesthetics, and may allow the stability in the mandibular anterior region. A careful case selection is necessary for an extraction of incisor. This patient reported with moderate overjet and overbite, lingually placed lower incisor, lingually inclined lower molars with acceptable soft tissue profile. Careful diagnosis is necessary to analyze the treatment goal and outcome.
 |
Figure 4: Mid treatment intra oral photos.
|
Patients who are suitable for single lower incisor extractions usually fit the following pattern4:
Class I molar relationship; moderately crowded lower incisors; mild or no crowding in the upper arch; acceptable soft-tissue profile; minimal to moderate overbite and overjet; minimal growth potential; missing lateral incisors or peg laterals4; under development of premaxillary area, tendency for anterior relationship of mandible to cranial base, short ramus, obtuse gonial angle and long body of mandible.6
Generally treating patients with extractions in both arches might have compromised the facial balance. Treating non-extraction would have produced gingival recession of the mandibular anterior. The extraction of a mandibular incisor capitalized on the advantages of both treatment approaches while minimizing disadvantages.1
 |
Figure 5: Post treatment intra oral photos with lingual retainers.
|
Factors to be considered regarding choice of extraction are6:
Amount of tooth size and arch size deficiency; Amount of anterior tooth ratio; Periodontal conditions; and Upper and Lower midline relationships.
Approximately 80% of orthodontic patients need arch expansion in cases of narrow maxilla.7
According to the literature, maxillary expansion can be done in two procedures. The first, Rapid Maxillary Expansion (RME), can be done by using an appliance that incorporates a screw, for example a Hass or Hyrax. The second is a slow maxillary expansion group which in cludes removable expansion plates, Porter W arch, and Quad Helix.
 |
Figure 6: Post treatment extra oral photos.
|
The Quad-Helix was developed in 1975 by Robert Murray Ricketts from Porter’s “W” arch, adding four loops to the appliance, increasing the wire length on 40 to 50 mm. The objective was to reduce the forces and better molar control.8 Several authors have written that the Quad-Helix appliance can deliver sufficient forces to promote skeletal changes on maxillary bone in younger patients.9-18
Some of the authors like Zachrisson in 1990 AJO, Hopkins in 1977 AJO, Fusher, Schwartz, Wits, Kokich and Shapiro also have studied the effects of incisor extractions.
Conclusion
Significant crowding case’s may be reasonably treated by either premolar or incisor extraction, but a single incisor extraction might yield a more stable result. But this is not a recommendation to resolve all cases of mandibular crowding with mandibular incisor extraction. A thorough careful case selection selection is a important criteria for deciding for the option of mandibular incisor extraction.
References
- Douglas J. K. The Mandibular central incisor, an extraction option. American Journal Of Orthodontics and Dentofacial Orthopedics. 1997.
- Jose-Antonio C. Mandibular incisor extraction: indications and long-term evaluation. uropean Journal of Orthodontics. 1996;18:485-489.
CrossRef - Nanda R. Considerations in Mandibular Incisor Extraction Cases. JCO. 2009;43(1):45-51.
- Owen H. A. Single lower incisor extractions. JCO. 1993.
- Negi K. S and Kapoor P. Mandibular incisor extraction in Orthodontics: case reports. Journal of Dental Applicaions. 2014.
- Levin S. Lower incisor extraction. AJO. 1969.
- Bench R. W et al. Terapia Bioprogressiva. 3a Edição. São Paulo: Editora Santos. 1996.
- Duarte M. S. O. aparelho quadrihélice (qua-helix) e suas variações. R Dental Press Ortodon Ortop Facial. 2006;11(2):128-156.
CrossRef - Bench R. W., Gugino C. F., Hilgers J. J. Bioprogressive Therapy. J Clin Orthod. 1978;12:279-298.
- Myers D. R., Barenie J. T. Bell R. A., et al. Condylar position in children with functional posterior crossbites: before and after crossbite correction. Pediatr Dent. 1980;2(3):190-4.
- Chaconas S. J., Levy J. A. A. Orthopedic and orthodontic applications of the quad-helix appliance. Am J Orthod. 1977;72(4):422-8.
CrossRef - Hicks E. P. Slow maxillary expansion: a clinical study of the skeletal versus dental response to low magnitude force. Am J Orthod. 1978;73(2):121-41.
CrossRef - Frank S.W., Engel G. A. The effects of maxillary on cephalometric measurements in growing orthodontic patients. Am J Orthod. 1982;5(81):378-389.
CrossRef - Chaconas S. J., Caputo A. A. Observation of orthopedic force distribution produced by maxillary orthodontic appliances. Am J Orthod. 1982;82(6):492-501.
CrossRef - Proffit W. R. Ortodontia Contemporânea. Pancast Editora Com e Repes Ltda. 1991;589.
- Brin I., Ben-Bassat Y., Blustein Y. Skeletal and functional effects of treatment for unilateral posterior crossbite. Am J. Orthod. Dentofac. Orthop. 1996;109(2):173-9.
CrossRef - . Sandikçioglu M., Hazar S. Skeletal and dental changes after maxillary expansion in the mixed dentition. Am J. Orthod. Dentofac. Orthop. 1997;111(3):321-7.
CrossRef - Boysen B., Cour K. L., Athanasiou A. E., et al. Three-dimensional evaluation of dentoskeletal changes after posterior cross-bite correction by quad-helix or removable appliances. Br J Orthod. 1992;19(2):97-107.
CrossRef

