Prevalence of Cardiovascular Diseases and Prescription Patterns in A Randomly Selected Population in Bangladesh
1Department of Pharmacy, BRAC University, 41 Pacific Tower, Mohakhali, Dhaka-1212, Bangladesh.
2Department of Pharmacy, Faculty of Allied Health Sciences, Daffodil International University, 4/2-Sobhanbagh, Dhanmondi, Dhaka-1207, Bangladesh.
Corresponding Author E-mail: arifur@bracu.ac.bd
DOI : http://dx.doi.org/10.13005/bpj/1147
Download this article as:
![]()
The basis for assessment of cardiovascular disease management is reliable on the demographic study of cardiovascular diseases (CVDs) and drug usage in a population. The aim of this study was not only to observe the prevalence of CVD in a population and the trend of drugs prescribed but to also identify the most prominent CVDs, the reasons behind their occurrence, types of treatment for all kinds of CVDs reported and the reason for choosing the particular drug singly or in a combination with other therapeutic classes. This descriptive study was carried out for a period of three months from July 2016 to the end of September 2016 among 853 patients, of which 427 patients visited National Institute of Cardiovascular Diseases (NICVD) while the other 426 visited the National Heart Foundation Hospital in Dhaka, Bangladesh. The patients were questioned with a self-developed questionnaire and their prescriptions were analysed to comprehend the trends of prescribed medicines and other diagnosis results. Out of 853 patients, the male and female patients were distributed in the ratio 5.8:4.2 with most patients coming from urban areas and suffering from lipid level disorder (more than 48%). The other CVDs reported were hypertension (30%), heart failure (28.5%), myocardial infarction (20.9%), ischemic heart disease (19.9%), stroke (17.1%) and angina (11%). Among all the combinations of drugs advised, the antianginal, ACE inhibitor and coronary vasodilator combination had a prevalence of 27.5% which was the maximum while the second most prescribed combination was the beta blocker and antihyperlipidemic drug (21.3%). This particular study allowed a detailed and extensive analysis of the CVDs, different methods of diagnosis and preferred treatment choice by the physicians and will also further help to determine and evaluate the usage of cardiovascular drugs utilisation in Bangladesh to successfully manage CVDs in the future.
KEYWORDS:Cholesterol; Cardiovascular Disease; Demographic; Circulatory; Lipoprotein; Triglyceride
Introduction
Cardiovascular disease (CVD) is a class of diseases that is the leading cause of global death at present and is responsible for 75% of the deaths occurring in developing countries like Bangladesh [1]. Analysing the current situation, it has been predicted that 25 million people will face death due to CVDs by 2030 [2, 3]. The most prominent CVDs that prevails at present are ischemic heart disease, cerebrovascular disease (stroke), peripheral vascular disease, heart failure, rheumatic heart disease, congenital heart disease and acute myeloid leukaemia (AML) [3, 4]. Among these, coronary artery diseases and stroke are the most common causes of death from CVDs. The present review says that both mortality and morbidity due to CVDs is increasing in Bangladesh.
A study carried out in Bangladesh revealed that 27.93%, 21.08% and 13.41% stroke patients with lipid disorder had high cholesterol, low-density lipoprotein (LDL) and triglycerides (TG) level, respectively [4]. From this data, a clear picture of the causes behind CVD can be obtained. The common risk factors of CVDs were identified by interviewing a number of physicians in these two hospitals, having at least 10 years of work experience along with additional questions in the questionnaire inquiring patients about their daily habits. The final findings were unhealthy diet, physical inactivity, tobacco and alcohol use. These eventually lead to abnormal blood lipid profile and obesity and thus CVDs [5].
The approach of cardiovascular disease management is more preventive than cure. But during this study, it was markedly seen that cardiovascular drugs are effectively lifesaving too. The possible treatment options for the management of CVDs are vasodilators, beta-blockers, lipid lowering agents, calcium channel blockers, ACE inhibitors, diuretics, etc. [6].
The purpose of this study was to understand the prevalence of cardiovascular and other circulatory diseases and the prescribing patterns of cardiovascular medicines. Focusing on this purpose, a fixed number of patients visiting the National Institute of Cardiovascular Disease (NICVD) and National Heart Foundation Hospital & Research Institute were randomly selected and their prescribed medicines were scrutinised for trend analysis.
In the past, population-based studies carried out to perceive the trends in drug use that have high significance for patient health outcomes, treatment and other health services. To carry out an efficient study, it requires effective information on the patient level characteristics that are significantly important for determining the best treatment. The main concern of this study was not only to observe the trend of drugs but to also observe the CVDs with maximum prevalence, the reasons behind them, types of treatment for all kinds of CVDs reported and the reason choosing the particular drug singly or in a combination with other therapeutic classes.
Methods and Materials
The conducted study was aimed to find out the prevalence of CVD among patients who visited the National Institute of Cardiovascular Disease (NICVD) and the National Heart Foundation Hospital & Research Institute, both situated in Dhaka, Bangladesh (NHFH). Along with the CVD, the different therapeutic groups of drugs prescribed to the patients were also observed and noted. NICVD and NHFH are most vital and specialised healthcare institute for CVDs and deals with the maximum number of CVD patients in Bangladesh. Patients from both the urban regions and rural regions of the country are found to visit these hospitals to seek the best possible healthcare services regarding CVDs. Critical and sophisticated patients are referred to these institutes and their treatment patterns itself interpreted as a reference by the physicians residing distant places from the city. Moreover, these centres receive a mixture of all classes of people in the society to receive high-intensity tertiary care. These institutes were selected to obtain a cross sectional type of data and to extrapolate the current practice prevailing in Bangladesh.
This descriptive study was carried out for a period of three months from July 2016 to the end of September 2016 among 853 patients, of which 427 patients visited NICVD while the other 426 visited the National Heart Foundation Hospital. The patients were questioned with a self-developed questionnaire and their prescriptions were analysed to comprehend the trends of prescribed medicines and the diagnosis from their lipid profile, electrocardiogram (ECG), blood glucose level, echocardiogram, blood pressure and other blood profiles. For statistical significance, all the data were incorporate into the computer and analysed using the modified Wald method in GraphPad prism software package and MS Excel 2013 [7]. Patients who were non-cooperative or who denied to face the questionnaire were excluded from the study.
Results and Discussion
The study was carried out in two tertiary level hospitals situated at the heart of the city.
Socio-Demographic Characteristics
Among the 853 patients who visited the centres, it was observed that 57.8% of the patients were male while 42.2% were female. 59.1% of the patients belonged to demographically developed areas while 40.9% belonged to rural areas [8, 9]. All patients belonged to an age group of above 30.
Table 1: Distribution of sex and demographic factors for cardiac disorder (n=853)
| Number of patients | Percentages (%) | |
| Sex | ||
| Male | 493 | 57.8 |
| Female | 360 | 42.2 |
| Demography | ||
| Rural | 349 | 40.9 |
| Urban | 504 | 59.1 |
From the data, it is apparent that the male patients are more prone to CVDs than female patients. This was due to the social structure of Bangladesh which has more privileges for men than women. Additionally, it was reported that more patients were from the urban regions compared to the rural regions which can be explained by the daily habits of people in the urban area giving rise to the risk factors of CVDs [10].
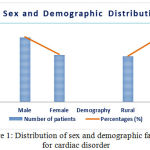 |
Figure 1: Distribution of sex and demographic factors for cardiac disorder |
Different Medical Disorders
From the diagnosis made by the physicians, it was seen that the patients suffered from different CVDs. It was reported that most patients, i.e. 48.7% suffered from lipid level disorder. 30% suffered from hypertension, 28.5% from heart failure, 20.9% from myocardial infarction and 19.9% from ischemic heart disease. It was also seen that 17.1% of the patients suffered a stroke while 11% of the patients suffered from angina.
Table 2: Scenario of different medical conditions among the patients (n=853)
| Medical condition | Number of patients | Percentages (%) |
| Lipid level disorder | 415 | 48.7 |
| Hypertension | 256 | 30 |
| Heart failure | 243 | 28.5 |
| Myocardial infarction | 179 | 20.9 |
| Ischemic heart disease | 170 | 19.9 |
| Stroke | 146 | 17.1 |
| Angina | 94 | 11 |
Most patients suffered from high cholesterol level, according to what the report suggested. This is probably a result of unhealthy diet, less physical activity and urbanisation. Hypertension was the most prevalent CVD and in one of the past studies, it has been seen that hypertension is the second leading CVD.
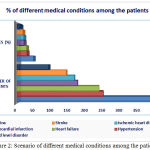 |
Figure 2: Scenario of different medical conditions among the patients |
Drugs Prescribed for Different Conditions
Different drugs of different pharmacological therapeutic classes were prescribed by the physicians, which have been categorised as shown below. More than 77% of the patients were advised to take lipid-lowering drugs and more than 82% patients were asked to take antiatherogenic drugs. Several antihypertensive drugs such beta blockers, ACE inhibitors, angiotensin receptor blockers and diuretics were prescribed in percentages of 52.1%, 32.4%, 15.4% and 39.2% respectively. The physicians also prescribed anxiolytics to 83.2% of the patients regardless of anxiety.
Table 3: Percentages of therapeutic classes prescribed (n=853)
| Therapeutic classes | Number of patients | Percentages (%) |
| Anxiolytics | 83.2 | 710 |
| Antiatherogenic | 82.3 | 702 |
| Antianginal | 78.9 | 673 |
| Lipid lowering drugs | 77.3 | 659 |
| Others | 62.3 | 531 |
| Beta-blockers | 52.1 | 444 |
| Diuretics | 39.2 | 334 |
| ACE inhibitors | 32.4 | 276 |
| Angiotensin receptor blockers | 15.4 | 131 |
| Calcium channel blockers | 13.0 | 111 |
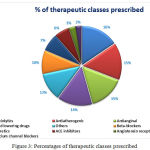 |
Figure 3: Percentages of therapeutic classes prescribed
|
In most cases, the patients were prescribed with 6.35 drugs on an average to treat all the clinical complications of cardiovascular disease, along with daily exercises and a proper healthy diet. Coronary heart disease patients were treated with antiatherogenic agents to prevent clotting at the coronary vessels because it may result in sudden myocardial infarction or stroke.
Beta-adrenergic receptor blockers are used mostly to treat hypertension. Beta-blockers are believed to reduce mortality rate when used for the prevention of myocardial infarction and chronic heart insufficiency [11]. The patients took ACE inhibitors and diuretics with very close frequency. Diuretics were recommended to older patients with type I and II hypertension as initial monotherapy or combined with other antihypertensives for patients with severe hypertension [12, 13]. The study significantly showed that angiotensin receptor blockers and calcium channel blockers were the least prescribed drugs by the specialists.
Therapeutic Combinations Prescribed
Among all the prescriptions of all the patients, it was mostly seen that physicians advised them to take a combination of different drug classes rather than a single class. It has been observed that most patients were prescribed to take the antianginal, ACE inhibitor and coronary vasodilator combination (more than 27%). Other class combinations have been seen to be advised more or less to similar percentages.
Table 4: Percentages of therapeutic combinations prescribed by physicians
| Therapeutic combination prescribed | Number of patients | Percentages (%) |
| ACE inhibitor + Beta blocker | 47 | 5.5 |
| Beta blocker + Angiotensin receptor antagonist | 47 | 5.5 |
| Antiangial + Antihyperlipidemic | 47 | 5.5 |
| Beta blocker + Antihyperlipidemic | 182 | 21.3 |
| ACE inhibitor + Antihyperlipidemic | 92 | 10.8 |
| ACE inhibitor + Antiangial | 92 | 10.8 |
| β blocker + Antiangial | 92 | 10.8 |
| Antihyperlipidemic + Angiotensin II receptor antagonist | 23 | 2.7 |
| Antihyperlipidemic + Coronary vasodilator | 23 | 2.7 |
| ACE inhibitor + Diuretics | 23 | 2.7 |
| Antihyperlipidemic + Beta blocker | 47 | 5.5 |
| Antiangial + Coronary vasodilator | 23 | 2.7 |
| ACE inhibitor + Coronary vasodilator | 47 | 5.5 |
| ACE inhibitor + Antiangial + Antihyperlipidemic | 47 | 5.5 |
| β blocker + Antihyperlipidemic + ACE inhibitor | 92 | 10.8 |
| Antiangial + ACE inhibitor + Coronary vasodilator | 235 | 27.5 |
| ACE inhibitor + Beta blocker + Antiangial | 23 | 2.7 |
| Angiotensin II receptor antagonist + ACE inhibitor+ Antihyperlipidemic | 23 | 2.7 |
Most patients were seen to be prescribed with more than one drug and a combination of three drug classes. Among all the combinations the antianginal, ACE inhibitor and coronary vasodilator combination had a prevalence of 27.5% which was the maximum. The second most prescribed combination was the beta blocker and antihyperlipidemic drug.
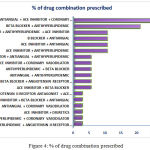 |
Figure 4: % of drug combination prescribed |
Conclusion
Several population-based studies have researched the trends in the drug use in the past but clinical studies on CVDs are not quite well known in Bangladesh. This particular study allowed a detailed and extensive analysis of the CVDs, different methods of diagnosis and preferred treatment choice by the physicians. The study aims to draw the attention of the Directorate General of Drug Administration (DGDA) to closely inspect the trends of drugs, prescribed by the specialists.
Statistical analysis reveals that statins and antiatherogenic agents are more dominantly prescribed or used cardiovascular drugs compared to others. Beta-blockers, ACE inhibitors and diuretics are predominant in the antihypertensive group. Changes in patterns of cardiovascular disease management and drug use are changing day by day. DGDA should undertake measures to change the law prescribing practice of ARBs and CCBs. This study will also further help to determine and evaluate the usage of cardiovascular drugs utilisation in Bangladesh.
Conflict of Interest
All authors have contributed equally and provided the consent to submit the article. The authors declare no conflict of interest for the article.
References
- Bangladesh Bureau of Statistics. Available at: http://www.bbs.gov.bd/. Accessed January
- American Heart Association. Heart and Stroke Statistical Update. Dallas, Tex.: American Heart Association, 2001.
- World Health Organization. Cardiovascular diseases. Available at: http://www.who.int/ mediacentre/factsheets/fs317/en/index.html. Accessed February
- Kabiruzzaman et al., Burden of heart failure patients in a tertiary level cardiac hospital. Journal of Bangladesh College of Physicians and Surgeons. 2010; 28:24-29
CrossRef - Badiuzzaman M, Mohammed FR, Chowdhury FR, Bari MS, Alam MB Ahasan Prevalence of modifiable risk factors among stroke patients in a tertiary care hospital in Dhaka. Journal of Medicine. 2009; 10(1): 18-21
- Science Daily, Depression and anxiety can double chances of heart ailments. January 19, 2008.
- Shaila A, Sonia S, Masuda M, Nargis P, Niru S, Samia S, Rishad M, Masuma A, Abu MS. Geriatric health problems in a rural community of Bangladesh. Ibrahim Med. Coll. J. 2007; 1(2): 17-20
- Esposti LD, Di Marrino M, Saragoni S, et al. Pharmacoeconomics of antihypertensive drug treatment: an analysis of how long patients remain on various antihypertensive therapies. Clin Hypetens. 2004; 6: 76-82
CrossRef - Psaty BM. Savage PJ, Tell GS, Polak JF. Hirsch CH. Gardin JM, McDonald RH. Temporal patterns of antihypertensive medication use among elderly patients. I993; 270(15): 1837-41
- Heaton PMJ and Cluxton RJ Jr. Beta-blocker underused in secondary prevention of myocardial infarction. Ann Pharmacother. 2004; 38: 286-293
CrossRef - European Society of Hypertension – European Society of Cardiology guidelines for the management of arterial hypertension, Guidelines Committee. J Hypertens. 2003; 21:1011-1053.
- Bloomfield P, Bradbury A, Grubb NR, Newby DE. Cardiovascular disease. In: Boon NA, Colledge NR, Walker BR, Hunter JAA (eds). Davidson Principles and Practice of Medicine, 20th ed. Churchill Livingstone, Edinburgh, 2006, pp. 519-644
- Esposti LD, Di Marrino M, Saragoni S, et al. Pharmacoeconomics of antihypertensive drug treatment: an analysis of how long patients remain on various antihypertensive therapies. Clin Hypetens. 2004; 6: 76-82
CrossRef




