
Alagarsamy Venkatesh1, Suresh Mitthra1, Venkatachalam Prakash1 and T. Srinivasa Prasad2
1Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College and Hospital, Bharath University, Chennai, Tamilnadu, India.
2Department of Oral and Maxillofacial Surgery, Meenakshi Ammal Dental College and Hospital, MAHER University, Chennai, Tamilnadu, India.
Corresponding Author Email: denvenkat@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1071
Abstract
Gemination and fusion are the most commonly encountered anomalies in dental practice, and distinction between the two is always challenging. Fusion is when two tooth buds fuse to make a large tooth. Gemination, also called double tooth is an anomaly exhibiting two joined crowns and usually a single root. It represents an incomplete attempt of a single tooth germ to split. It is considered multifactorial in etiology, with genetic and environmental causes. It is extremely difficult to differentiate between fusion and germination especially when a supernumerary is attached with the adjacent tooth. This paper highlights the importance of diagnosing developmental anomalies of teeth and the proper treatment outcome of these abnormalities.
Keywords
Gemination; fusion
Download this article as:| Copy the following to cite this article: Venkatesh A, Mitthra S, Prakash V, Prasad T. S. Gemination or Fusion ? – A case report. Biomed Pharmacol J 2016;9(3). |
| Copy the following to cite this URL: Venkatesh A, Mitthra S, Prakash V, Prasad T. S. Gemination or Fusion ? – A case report. Biomed Pharmacol J 2016;9(3). Available from: http://biomedpharmajournal.org/?p=11859 |
Introduction
Third molars may clinically presents with varied morphology. The most common involves the varied number and forms of root. Involvement of the crown resulting in abnormal coronal morphology is rare. Gemination is a developmental anomaly as a result of a single tooth bud to divide. This leads to the formation of a tooth exhibiting a bifid crown with a common root and root canal. [1] Gemination is clinically similar to fusion and is assessed by the count of teeth in the dentition. Gemination is a single enlarged tooth in which the tooth count is normal when the anomalous tooth is counted as one. Fusion is the combining of two tooth germs to form an enlarged tooth. Here the tooth count is one less, when the anomalous tooth is counted as one.
This anomaly leads to higher caries potential, malocclusion, changes in the dental arch shape, periodontal disease, hyper/ hypodontia, eruptive disturbance of successional tooth and creates poor esthetics, periodontal diseases,high caries incidence. [2]
Case report
A 26 year old female patient presented to the dental clinic with a complaint of pain in 38 region.The patient was the second of 3 siblings of parents with no history of consanguinity. The patient appeared normal and healthy with no reported history of orofacial trauma.
On examination,the patient had a unusually large left third molar presenting like a double tooth. . Dental caries was present in the mesial surface of the the tooth. Intraoral periapical (IOPA) radiographs revealed radiolucent groove in the crown region. C.T was taken to determine the presence of double tooth [Figure 1 & 2]. Patient was not willing for extraction and after opinion from endodontist root canal treatment was performed. Separate canals were located and obturated and crowns were placed [Figure 3].
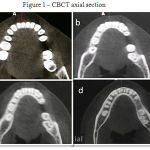 |
Figure 1: Cbct Axial Section |
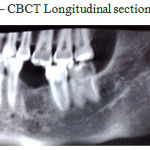 |
Figure 2: Cbct Longitudinal Section |
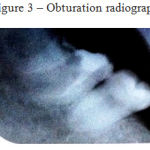 |
Figure 3: Obturation Radiograph |
Discussion
Developmental abnormalities in the form and number of teeth are congenital and appear in primary and permanent dentition. Fusion and germination are two different dental anomalies clinically manifested by formation of a large tooth[3].Gemination occurs when a single tooth bud attempts to divide resulting in two completely or incompletely separated crowns with a single root or root canal [4]. Fusion occurs when there is union of two completely separate tooth buds. The terms “double tooth”, “double formations”, joined teeth” or “fused teeth” are often used to describe gemination and fusion [5]. When a single tooth is partially cleaved it is ‘true gemination’ and completely cleaved they are also named ‘twinning’. Similarly when two tooth germs fuse during formation and show union of enamel and dentine they are termed ‘true fusion’. When union occurs in dentin and /or cementum, they are termed ‘late fusion’ and a late fusion by cementum is termed ‘concresence’ [6].
Higher prevelance is seen in deciduous dentition though it occurs in both with anterior region being the most common site[7]. It is found with a higher incidence in the lower jaw, with equal sex predilection [ 8,9]. Unilateral gemination is with a prevalence rate of 0.5 % and 0.1% in deciduous and permanent dentition respectively. Bilateral cases are seen in 0.01% to 0.04% in primary dentition and in 0.02% to 0.05% in permanent dentition [10]. Commonly affecting the anterior teeth with germination more commonly in maxillary arch and fusion in the mandibular arch, this anomaly manifests itself from a minor notch in the incisal edge of an abnormally wide tooth to the appearance of almost two separate crowns in both the sexes with an equal sex predilection [11, 12]. Our case reported with a unilateral anomaly in the mandibular arch which is relatively rare.
Inspite of various studies the etiology of gemination remains unknown. Evolution, trauma, heredity and environmental factors are thought to play a role in formation of germination and fusion [13]. Studies by Spouge have suggested that it may also result from traumatic disturbances to the developing tooth bud [14]. Other reasons which are considered as the cause of gemination and fusion are infectious inflammatory processes, nutritional and endocrine disturbances [15]. It is understood that these anomalies are caused by an interaction between a variety of genetic and environmental factors [16].
Clinically these patients present with a poor esthetics in case of anterior teeth, a higher degree on caries and periodontal problems. Due to the deep grooves present in the tooth these patients have a greater incidence of caries presentation. These grooves also lead to periodontal problems like pocket formation and gingival inflammation [10]. When present in the primary dentition, exfoliation may occur depending on root resorption [17].
Diagnosis of gemination and fusion are usually carried out clinically. Clinically if not impossible it may be difficult for diagnosing gemination and fusion. In case of fusion the number of clinical teeth is reduced as there is an attempt of two tooth buds to fuse to one and gemination represents as as attempt of a single tooth bud to divide with no change in the number of teeth. However radiographically there will be two distinct pulp chambers in fused tooth and in gemination there is only one pulp chamber [18].Gemination can be differentiated from fusion by the number of tooth but if the fusion is with a supernumerary tooth the count would be normal. Thus making diagnosis between fusion and gemination difficult. Our case reported with the anomaly on the third molar making it difficult to conclude whether it was a fusion between a third molar and supernumerary tooth or a gemination of a third molar.
The treatment depends upon the patient requirement, the teeth involved, and the degree of involvement. If a primary tooth is involved the treatment depends upon the presence of the succedaneous tooth [18]. In our case retaining the tooth was the primary concern of our patient .Pain due to caries, periodontal problems and occlusal disturbances were taken into consideration for this patient and a multidisciplinary approach was required for establishment of proper and functional success of treatment.Endodontist opinion was taken and two separate access cavities were opened. One access opening corresponds to the molar tooth and the other to the geminated or fused tooth. A communication between the two was found below the dentine. Five canals were located, three for the third molar and two for the additional tooth. The canals were instrumented, irrigated and working length was determined. The canals were obturated and filled with permanent restoration. Patient was called for follow-up and reported asymptomatic.
Conclusion
The presence of dental anomaly and correct diagnosis is always a challenge for the dentist. Early observation of the anomaly followed by clinical and radiographic evaluation will result in restoration of the tooth. Knowledge of the existence and morphology of the tooth will help the dentist in proper treatment planning.
References
- Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology ed 2. Philadelphia: Saunders, 2002; 84-85.
- Knezevic, S. Travan, Z. Tarle, J. Sutalo, B. Jankovc and I. Ciglar. Double Tooth, Coll. Antropol. 26 (2002) 2: 667–672
- Patel JR. Gemination. Oral Surg Oral Med Oral Pathol 1984 ; 57(2) : 232.
- Blank BS, Ogg RR, Levy AR. A fused central incisor. Periodontal considerations in comprehensive treatment. J. Periodontol 1985;56:21-4.
- Duncan WK, Helpin ML. Bilateral fusion and germination: A literature analysis and case report. Oral Surg Oral Med Oral Pathol 1987; 64:82-7
- Tannenbaum AK , Alling EE. Anamolous tooth development: Case report of germination and twinning. Oral Surg,Oral Med, Oral Pathol 1963;16,883-88.
- Chipshvili n, Vadachkoria D,Beshkenadze E. Gemination or fusion ? – challenge for dental practitioners. (case study). Georgian Med News.2011 May;(194):28-33.
- Hagman F.T., J Dent. Child, 52(1985) 459.
- Duncan. K, P.J.M. Crawford, J.Dent.Child, 17(1996) 365.
- Turkaslan S,Gokce HS, Dalkiz M (2007). Esthetic rehabilitation of bilateral geminated teeth; a case report. Eur J Dent 7; 188-191.
- Welbury RR. Paediatric dentistry 2nd Pg 277 -78.Oxford : Oxford University Press,2001.
- Yeun SWH, Chan JCY, Wei SHY. Double primary teeth and their relationship with the permanent successors: a radiographic study of 376 cases. Pediatr Dent 1987; 9:42-52.
- Wu CW,Lin YT.Lin YT. Double primary teeth in children under 17 years old and their correlation with permanent successors. Gung Med J 2010;33: 188-93.
- Spouge JD.Oral Pathology.St.Louis:C.V.Mosby Co: 1973
- Turkaslan s,Gokce HS, Dalkiz M.(2007) Esthetic rehabilitation of bilateral geminated teeth: a case report.Eur J dent 7: 188-91.
- Faiez N.Hattab, Abdalla M. Hazz’a. An unusal case of talon’s cusp on geminated tooth.J Can Dent Assoc 2001;67:263-6.
- Sandya Shrivastava,Manish tijare,Swetha Singh. Fusion/Double teeth.Journal of Indian Academy of Oral Medicine and Radiology.July – Sep 2011;23(3):S468-470.
- Ahmetercan Sekerci, Yildiray Sisman, Yasin Yasa, Halil Sahman, Abdullah Ekizer.Prevelance of fusion and germination in permanent teeth in Coppadocia population in Turkey. Pakistan Oral & Dental Journal. Vol 31,no 1.( June 2011).

