
Neda Azarpey1, Mojgan Kalantari1, Elham Keshavarz1 and Azadeh Joolayee2
1Department Of Radiology, Mahdiyeh Hospital, Shahid Beheshti University Of Medical Sciences, Tehran, Iran
2Department Of Surjery, Mahdiyeh Hospital, Shahid Beheshti University Of Medical Sciences, Tehran, Iran.
Corresponding Author Email: Mojgankalantary@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1042
Abstract
Breast cancer is one of the most common types of cancer and constitutes one of the main reasons of death caused by cancer among women. Preventing cancer on one hand and treating it on the other hand can help reduce the burden of disease. Among the various diagnostic methods used, we may list sonography, mammography, and MRI. The present research seeks to provide a qualitative and quantitative account of variables in MRI and study the correlation between variables and consequences. The present research was conducted on 50 patients suffering from breast cancer resorting to hospitals of Shahid Beheshti University selected through convenient sampling. All of them underwent MRI with contrast. Pattern of various tumors was studied in patients. The results were analyzed and studied using Chi-Square Tests. According to the results, spiculated tumor patterns exhibited the greatest degree of frequency (36%). The results gained from the analysis of enhancement curve of MRI showed that T3 and T1 curves with respective frequencies of 40 and 12 percent exhibited the greatest and lowest frequencies. According to pathological results, invasive ductal carcinoma and lobular carcinoma in situ exhibited the greatest frequencies in T3 enhancement curve and the greatest frequency of ductal carcinoma in situ was observed in type 2 curve. A statistical analysis showed that variables such as the size of tumor and patient’s age had no significant correlation with the type of the curve (P-Value > 0.05). There was also no particularity between the size of tumor and patient’s age and pathological results. It was finally shown that no significant correlation existed between the triple types of MRI enhancement curves and the results of pathology (P-Value > 0.05). The results of this research showed no significant correlation between enhancement curve and variables such as patient’s age, tumor pathology and size of tumor.
Keywords
Breast Cancer; Tumor Pattern; Enhancement Curve; MRI
Download this article as:| Copy the following to cite this article: Azarpey N, Mojgan Kalantari M, Keshavarz E, Joolayee A. Enhancement Curve of MRI with Contrast in Malignant Breast Lesions. Biomed Pharmacol J 2016;9(3). |
| Copy the following to cite this URL: Azarpey N, Mojgan Kalantari M, Keshavarz E, Joolayee A. Enhancement Curve of MRI with Contrast in Malignant Breast Lesions. Biomed Pharmacol J 2016;9(3). Available from: http://biomedpharmajournal.org/?p=11743 |
Introduction
Cancer has been known as one of the main life threatening factors which affects its quality and the same fact has triggered plenty of researches in this field. Breast cancer is one of the most common types of cancer responsible for a large death toll among both men and women every year. In spite of various progresses made concerning the early diagnosis and appropriate treatment of this disease, it is still the main cause of deaths caused by cancer among women [1]. As many as 1.38 million new cases of this disease were recorded only in 2008. A large degree of heterogeneity is observed in the possibility of the survival of patients. The possibility of survival for 5 years in developed countries is 80%, but the same possibility in developing countries is no more than 40% [2]. Although new strategies are introduced every day to cope with breast cancer, this disease still threatens the life of many people.
Photographic methods such as mammography, ultrasound imaging (sonography) and magnetic resonance imaging are some of the methods used for the early diagnosis of breast cancer. Mammography is the most common technique of breast imaging. In spite of its convenience and affordability and availability, this method is not able to diagnose all types of breast cancer [3, 4]. As a result, other methods have been proposed for breast imaging among which, ultrasound method (whether the basic, Doppler or contrast) are the most widely used methods.
Breast MRI is a relatively new method which has quickly gained acceptance as a result of its sensitivity. However, after using it to diagnose malignancies and breast lesions for a short time, it turned out that the specificity of this method is not very promising [5, 6]. This problem is mostly caused by pseudo positive results in this type of imaging that causes mental problems for patients. What’s more, this method is more complex and costly than other methods [7, 8].
The present research seeks to study the enhancement curve of breast malignant lesions in MRI with injection.
Materials and Method
Convenient sampling method was utilized and the sample was set to 50 people according to the following formula. SPSS v.18 and chi-square and Fisher tests were used to analyze the data. The level of significance to interpret these relationships was set to 0.05.
In this cross sectional-observational study where a qualitative and quantitative account of variables and their relationships and consequences are discussed, 50 patients with breast cancer resorting to hospitals of Shahid Beheshti University were selected in accordance with the principles of convenient sampling and all of them underwent MRI with contrast.
Result
The average age of the participants in this research was 47.40 years old with a standard deviation of 9.37. The tumor size of the patients was also measured and reported in mm3. According to the results, as many as 41 people (82%) studied had tumors smaller than 25000 mm3 and the number of people with larger tumor sizes was much less.
Various tumor patterns were studied in patients and 9 patterns were diagnosed: irregular, siculated, irregular and spiculated (Ir and Sp), irregular and necrotic center, oval shape, lobulated, sharp, heterogenous large, and ill-defined. Spiculated and irregular patterns with respective frequencies of 18 people (36%) and 12 people (24%) had the greatest frequencies. The status of the patterns is presented in chart 1.
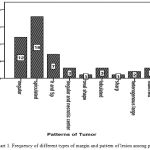 |
Figure 1: Frequency of different types of margin and pattern of lesion among patients |
After sampling the tumor tissue, the samples were sent to laboratory to determine the pathological state. According to pathological results, ductal carcinoma in situ with 22 cases had the highest frequency (44%), while invasive ductal carcinoma with 12 cases (24%) had the lowest percent of frequency. Different types of pathology identified in this research are presented in chart 2.
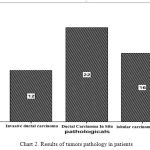 |
Figure 2: Results of tumors pathology in patients |
The results of the analysis of MRI enhancement curve showed that type 3 curve with 20 cases (40%) had the highest frequency, while type 1 curve with 12 cases (24%) had the lowest frequency. The frequency of all three types of MRI enhancement curve in the present research is presented in chart 3.
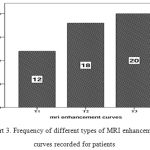 |
Figure 3: Frequency of different types of MRI enhancement curves recorded for patients |
Chart 4 presents the frequency of each pathology results in triple types of MRI enhancement curve (right hand side chart), while the frequency of all types of MRI enhancement curves in each pathology is also depicted (left hand side). A statistical analysis of the results showed that invasive ductal carcinoma and lobular carcinoma in situ had the greatest degrees of frequency in the third type of MRI enhancement curve (T3), while the highest frequency in type 2 curve belongs to ductal carcinoma in situ.
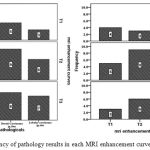 |
Figure 4: Frequency of pathology results in each MRI enhancement curves and vice versa |
The correlation between the tumor size recorded for patietns and their MRI enhancement curves was analyzed. The results gained through non-parametric Kruskal-Wallis test pointed to the fact that although the majority of the participants had type 3 enhancement curves, there was no statistically significant correlation between tumor size and type of curve (P-Value > 0.05). The present research also studied the correlation between patient’s age recorded in patient’s history and his MRI enhancement curve. The results of this part of research achieved through non-parametric Kruskal-Wallis statistical test shows that although the majority of participants had type 3 enhancement curve, no statistically significant correlation can be established between the age of patient and type of curve (P-Value > 0.05).
The average tumor sizes in each pathology group of invasive ductal carcinoma, ductal carcinoma in situ, and lobular carcinoma in situ were compared against one another through non-parametric Kruskal-Wallis statistical test. The results of this test failed to establish a significant correlation between tumor size and pathology results (P-Value > 0.05). This means there is no specificity between tumor sizes and pathology results. Thus, it is impossible to determine the type of pathology based on the size of tumor.
The average ages of patients in each pathology group of invasive ductal carcinoma, ductal carcinoma in situ, and lobular carcinoma in situ were compared against one another through non-parametric Kruskal-Wallis statistical test. The results of this test failed to establish a significant correlation between tumor size and pathology results (P-Value > 0.05). This means there is no specificity between patient’s age and pathology results. Thus, it is impossible to determine the type of pathology based on patient’s age.
Non-parametric Chi-Square Tests were used to statistically study the correlation between MRI enhancement curves and pathology results. Analysis of the data concerning this part of research (considered to be the most important part) failed to find a statistically significant correlation between three types of MRI enhancement curves and pathology results (P-Value > 0.05).
This results highlight the fact that MRI enhancement curves are not specific and predicting the type of pathology based on that is not possible.
Discussion
In most cases where mammography or clinical results show suspiciously abnormal findings, further analysis shows benign pathology [5]. Concerning the high contrast in soft tissue and the possibility of separating thin imaging slides, it is possible to achieve a higher degree of precision than normal methods of imaging. Although the sensitivity of MRI method for breast imaging has been estimated to range from 94% to 100%, various results have been reported concerning the specificity of this method (37% to 97%). The results of early MRI enhancement of breast indicates higher levels of correlation in the image of breast cancer after injection of contrast material [9, 10]. Further researches indicate the existence of this rising phenomenon not just in malignant cancers, but also in benign types such as Fibroma and fibrocystic changes [11-14].
There is no doubt that early diagnosis of cancer lesions is the biggest challenge of breast imaging. Although mammography is one of the most widely used breast imaging methods, but the sensitivity of this method in diagnosing malignancies of breasts (particularly in the congested areas of the breast) is far from being acceptable [5, 15]. What’s more, the patient is exposed to X-ray radiation and this makes several and regular repetition of the test impossible.
The results of this research failed to establish a significant correlation between MRI enhancement curves with contrast and tumor size, patient’s age and type of pathology. These are in line with the results reported by StasinHa et al who observed that enhancement alone has no efficiency in pathological diagnosis of disease and it is unable to diagnose breast cancer in 13% of the cases [16]. The results of this research also indicate no correlation between patient’s age and pathology results and tumor size with these results.
Many researchers have attempted to describe the reason of this weak correlation between enhancement with contrast and pathological diagnosis of disease (particularly diagnosing proliferating malignancies). For instance, Teifke et al studied 464 cases of MRI where 354 of them were diagnosed malignancy. 12% of these 354 cases showed no enhancement with contrast in MRI [17]. Various reasons were mentioned by these researchers to justify pseudo-negative results including technical errors (where the site of lesion is different from the site studied, shaking artifacts while imaging, incorrect use of the factor causing contrast), inability to distinguish cancer tissue from surrounding tissues with high enhancement, and the small size of tumor (smaller than 5 mm) in the early phases of Carcinogenesis. Orel et al. and Giller et al. believe that factors such as weak Angiogenesis of tumor tissue as effective factors in this phenomenon [17, 18].
Another point made clear in the researches conducted by other groups is the greater ability of mammography than MRI in diagnosing Premalignant cases in cancers which will become fully malignant in future.
In this case and when mammography indicates existence of suspicious microcalcification bundles, it is impossible to discard the possibility of lesion merely because there is no enhancement in MRI [16, 19, 20].
Based upon the above-said facts, analysis of MRI results can be effective merely when there is complete information and images captured through other methods (as a supplement).
References
- Ferlay, J., et al., Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer, 2010. 127(12): p. 2893-917.
- Siegel, R., D. Naishadham, and A. Jemal, Cancer statistics, 2013. CA Cancer J Clin, 2013. 63(1): p. 11-30.
- Kolb, T.M., J. Lichy, and J.H. Newhouse, Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology, 2002. 225(1): p. 165-75.
- Smith, A., et al., American Cancer Society guidelines for breast cancer screening: update 2003. CA Cancer J Clin, 2003. 53(3): p. 141-69.
- Kuhl, C.K., et al., Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology, 1999. 211(1): p. 101-10.
- Kang, S.S., et al., Background parenchymal enhancement on breast MRI: influence of menstrual cycle and breast composition. J Magn Reson Imaging, 2014. 39(3): p. 526-34.
- Hu, Q., et al., Meta-analysis of contrast-enhanced ultrasound for the differentiation of benign and malignant breast lesions. Acta Radiol, 2015. 56(1): p. 25-33.
- Yu, D., Y. Han, and T. Chen, Contrast-enhanced ultrasound for differentiation of benign and malignant thyroid lesions: meta-analysis. Otolaryngol Head Neck Surg, 2014. 151(6): p. 909-15.
- Kaiser, W.A. and E. Zeitler, MR imaging of the breast: fast imaging sequences with and without Gd-DTPA. Preliminary observations. Radiology, 1989. 170(3 Pt 1): p. 681-6.
- Heywang, S.H., et al., MR imaging of the breast with Gd-DTPA: use and limitations. Radiology, 1989. 171(1): p. 95-103.
- Fobben, E.S., et al., Breast MR imaging with commercially available techniques: radiologic-pathologic correlation. Radiology, 1995. 196(1): 143-52.
- Stomper, P.C., et al., Suspect breast lesions: findings at dynamic gadolinium-enhanced MR imaging correlated with mammographic and pathologic features. Radiology, 1995. 197(2): p. 387-95.
- Harms, S.E., et al., MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology, 1993. 187(2): p. 493-501.
- Orel, S.G., et al., Suspicious breast lesions: MR imaging with radiologic-pathologic correlation. Radiology, 1994. 190(2): 485-93.
- Gribbestad, I.S., et al., Comparative signal intensity measurements in dynamic gadolinium-enhanced MR mammography. J Magn Reson Imaging, 1994. 4(3): p. 477-80.
- Stusinska, M., J. Szabo-Moskal, and B. Bobek-Billewicz, Diagnostic value of dynamic and morphologic breast MRI analysis in the diagnosis of breast cancer. Pol J Radiol, 2014. 79: p. 99-107.
- Teifke, A., et al., Undetected malignancies of the breast: dynamic contrast-enhanced MR imaging at 1.0 T. Radiology, 2002. 224(3): 881-8.
- Schnall, M.D., et al., A combined architectural and kinetic interpretation model for breast MR images. Acad Radiol, 2001. 8(7): p. 591-7.
- Orel, S.G., et al., MR imaging of ductal carcinoma in situ. Radiology, 1997. 202(2): p. 413-20.
- Liberman, L., et al., Breast lesions detected on MR imaging: features and positive predictive value. AJR Am J Roentgenol, 2002. 179(1): p. 171-8.

