
Majid Galini1 and Seyed Morteza Bagheri2*
1Resident of Radiology , Iran University of Medical Sciences, Tehran, Iran.
2Department of Radiology, Hasheminejad Kidney Center (HKC), Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author E-mail : smb_53@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1003
Abstract
Varicocele is cited as one of the most common treatable causes of male factor infertility. Diagnosis of varicocele is based on physical examination and also sonography. The aim of this study was to assess the sensitivity and specifity of gray-scale sonography for diagnosis of varicocele . This cross-sectional study was performed on 92 patients in Hasheminejad kidney center , Tehran, Iran. Patients with suspected varicocele who referred to Radiology Department were included. Gray-scale sonography and Color Doppler Ultrasound were performed on patients at rest and Valsalva maneuver. Mean age of patients was 34/55±9/44. In this study a sensitivity of 71% and specificity of 60.7% in gray-scale sonography during Valsalva maneuver were compared to Doppler sonography at cut point of 3/25 mm, and positive predictive value was 80% and negative predictive value was 48/6% (p<0.000), and also there was a significant relationship between duration of reflux and increasing of venous diameter. A sensitivity of 98/4% and specificity of 71.4% in gray-scale solography (with consideration of differentiation of diameter before and during Valsalva maneuver) were compared to Doppler sonography at cut point of 0.2 mm, and positive predictive value was 85.9% and negative predictive value was 94.7%. Based on the results of this study, gray scale ultrasound is a good imaging technique for Diagnosis of varicocele and differentiation of diameter before and after Valsalva maneuver had better sensitivity, specificity, positive predictive value and negative predictive value.
Keywords
Varicocele; Gray scale ultrasound; Doppler ultrasound
Download this article as:| Copy the following to cite this article: Galini M, Bagheri S. M. Comparison of Gray-scale Sonography with Doppler Evaluation in Diagnosis of Varicocele. Biomed Pharmacol J 2016;9(2). |
| Copy the following to cite this URL: Galini M, Bagheri S. M. Comparison of Gray-scale Sonography with Doppler Evaluation in Diagnosis of Varicocele. Biomed Pharmacol J 2016;9(2). Available from: http://biomedpharmajournal.org/?p=7658 |
Introduction
Varicocele is an enlargement greater than 2 mm (1), [in some medical references more than 3 mm (2)] and tortusity of the pampiniform venous plexus in the scrotum (3, 4). Varicocele has been found in approximately 15% to 20% of the general population (5) however, it has been diagnosed in one third of infertile men (6). Varicocele is one of the most common causes of the decreased sperm production and quality (7). The clinical diagnosis of varicocele is commonly made by physical examination with observation of varicose veins in the scrotum that enhanced by valsalva maneuver. But in some cases clinical diagnosis is not reflect severity and it is necessary to use other accurate techniques (8). Color Doppler ultrasonography is the most sensitive non-invasive diagnostic method and has a sensitivity of approximately 95% in the diagnosis of varicocele. While the sensitivity of physical examination is 70%.In addition ultrasonography is a reliable, noninvasive and low cost method in comparison with other techniques (9). Doppler ultrasound can accurately detect varicoceles and determine the treatment plan; the simultaneous presence of venous reflux is a major factor affecting sperm production and infertility, and indication of surgery (10).
Despite the high diagnostic value of color Doppler ultrasonography, it has limitations like high cost and non availability in all centers. The aim of this study was to evaluate gray scale sonography in comparison with color Doppler ultrasonography in diagnosis of varicocele in rest and valsalva position.
Materials and Methods
Participants and Procedures
This diagnostic cross- sectional study was performed on 92 patients with suspected varicocele who were referred to radiology department in Hasheminejad Kidney center , Tehran, Iran in 2013. Inclusion criteria were suspected diagnosis of varicocele and patients’ willingness to participate. Patients with benign or malignant scrotal tumor, inflammatory testicular disease, hydrocele and secondary varicocele were not recruited in this study. The convenience sampling method was used. The sample size was 92 patients with α = 0.05 and β = 0.2(11).
Each participant was informed about the purpose of the study and written informed consent was obtained from all participants. Also, the confidentiality of information was managed by researchers. The study was approved by the ethical committee of the center.
Gray scale and Doppler sonography were performed with GE Voluson 730 pro (8-10MHz) for every patient. At first gray scale sonography was performed to evaluate pampiniform plexus. Then we evaluated vein diameter, presence of reflux and duration of reflux in both side of scrotum at supine position and Valsalva maneuver. Data were collected in specific check list.
Gray Scale and Doppler Sonography Examination
Statistical Analysis
In descriptive statistics, proportion was used to describe categorical and numerical variables. Mean and SD used to describe continuous variables and for assessing the normal distribution of continuous variables Kolmogorov‑Smirnov test was used. All analysis was conducted using the Statistical Package for the Social Sciences (SPSS) 20.0. Paired t‑test were used to compare means of continuous variables with normal distribution. The cut-off points, sensitivity, and specificity were determined by receiver operator characteristic (ROC) analysis. P-values less than 0.05 were considered statistically significant.
Results
In this cross- sectional study we have examined 92 patients. The mean age of patients was 34.55 ± 9.44 with the range from 18 to 65 years old. Mean diameter of vein before Valsalva maneuver was 3.046 ± 0.37 mm with the range from 2.3 to 4 mm and the mean diameter during Valsalva maneuver was 3.48 ± 0.43 mm with the range from 3 to 47 mm. The mean duration of reflux was 5.012 ± 3.52 seconds (range from 0 to 12).63 patients (68%) had reflux. A left-sided varicocele was seen in 81 cases (88%), and a bilateral varicocele in 11 cases (21%).There was no case of right-sided varicocele. The most common symptom was pain. 54 (58.7) cases due to pain, 33 patients (35.9%) because of infertility, and 5 (4/5%) cases due to other symptoms referred to our clinic. We determined the cut-off value of venous diameter during Valsalva maneuver for gray scale sonography in comparison with Doppler sonography. With the cut-off point of 3.25 mm, the best sensitivity, and specificity were achieved 71% and 60.7%, respectively. The area under curve (AUC) was 0.744(P value < 0.001) [Figure 1].
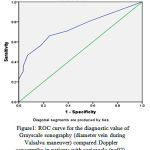 |
Figure 1: ROC curve for the diagnostic value of Grayscale sonography (diameter vein during Valsalva maneuver) compared Doppler sonography in patients with varicocele (n=92).
|
At this cut-off point positive predictive value (PPV) and negative predictive value (NPV) were 80% and 48.6% respectively. Then we computed the difference between venous diameter before and during Valsalva maneuver. Cut-off point, sensitivity, and specificity were determined by receiver operator characteristic (ROC).At the cut-off point of 0.2 mm the best sensitivity, and specificity were98.4% and 71.4 % respectively. The area under curve (AUC) was 0.984(P value < 0.001) [Figure 2]. At this cut-off point positive predictive value (PPV) and negative predictive value (NPV) were 85.9% and 94.7% respectively .There was statistical significant correlation between diameter of vein after Valsalva maneuver and reflux duration(r= 0.538, P value < 0.001) .With paired t-test there was differences between mean diameter of vein before and during Valsalva maneuver (t=14.513, df=91, P value < 0.001).
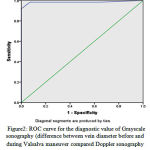 |
Figure 2: ROC curve for the diagnostic value of Grayscale sonography (difference between vein diameter before and during Valsalva maneuver compared Doppler sonography in patients with varicocele (n=92).
|
Discussion
Normal diameter of the pampiniform venous plexus is 0.5 to 1.5 mm. Varicocele is an enlargement greater than 2 mm of the pampiniform venous plexus in the scrotum and it is usually located on postero lateral of testis (1, 2). Testicular varicocele is the most common correctable cause of male infertility and surgery could improve quality of sperm up to 50%. It is abnormally dilated veins within the spermatic cord (12). Gray-scale ultrasonod shows multiple anechoic, serpiginous, tubular structures of varying sizes. Doppler sonography reveals venous flow pattern and retrograde flow. Our study showed that sensitivity and specifity of the difference between venous diameter before and during Valsalva maneuver at cut-off point of 0.2 mm were 94.8% and 71.4% respectively. At this cut-off point positive predictive value (PPV) and negative predictive value (NPV) were 85.9% and 94.7% respectively. These results showed that gray scale sonography had desirable sensitivity and specifity to diagnose of reflux during Valsalva maneuver. This research illustrated that the difference between venous diameter before and during Valsalva maneuver in comparison with venous diameter during Valsalva maneuver had better sensitivity, specifity, positive predictive value (PPV), and negative predictive value (NPV). Pierik et al evaluated 1372 infertile men and Doppler sonography could diagnose 407(29.7%) of patients with varicocele during Valsalva maneuver, but Gray scale sonography detected 60% of 407 patients with varicocele. Sensitivity of Gray scale was 60% in comparison with Doppler sonography (11). Our evaluations was almost consistent with Pierik,s study. Other research evaluated 34 asymptomatic young men with physical examination, standard scrotal sonography and color Doppler evaluation of the scrotal veins. Of the subjects 15% had varicoceles by physical examination and 18% by Gray scale sonography, while 35% had retrograde flow by color Doppler evaluation. At this study Gray scale ultrasound had a sensitivity of 48% compared with Doppler evaluation (13).Battino et al studied sensitivity and specificity of clinical examination and ultrasonography compared with venography. Sensitivity of clinical examination and Doppler sonography were 64% and 94% respectively and specifity of clinical examination and Doppler sonography was 100 %( 14).
Nabahaty et al evaluated 85 patients with symptom of scrotum pain, fullness and infertility who referred to a private office. Consistency rate of clinical grading of varicocele sonography findings were reviewed. A sensitivity of 94.7% and specificity of 64.9% in sonography were compared to physical examination, and positive predictive value was 68.6%, negative predictive value was 93.8%, and also there was a significant relationship between existence of reflux and increasing grade of varicocele in physical examination with increasing of venous diameter (15).
Karami et al assessed 103 men (44 normal and 59 with clinical varicocele). The strongest correlation between venous diameter and clinical grade of varicocele was observed when the venous diameter was measured at the level of epididymal head in the upright position with Valsalva maneuver (r: 0.87, P-value < 0.0001). In aforementioned conditions, venous diameter of 2.35 mm (sensitivity 87%, specificity 87%) can distinguish normal subjects from grade 1 varicocele, venous diameter of 3.15 mm (sensitivity 58%, specificity 70%) can discriminate grade 1 from grade 2, and venous diameter of 3.75 mm (sensitivity 83%, specificity 70%) can differentiate grade 2 from grade 3. Furthermore, venous diameter of 2.65 mm (sensitivity 91%, specificity 89%) can distinguish normal subjects from patients with clinical varicocele (16).
There was significant correlation between venous diameter during Valsalva maneuver and duration of reflux. This means that by increasing the diameter of the vein, the duration of reflux increased. It seems that that the difference in venous diameter before and during Valsalva maneuver in comparison with venous diameter during Valsalva is more appropriate for the diagnosis of varicocele.
References
- Sutton D. Text book of radiology & imaging.7 th ed .London: Churchill Livingstone; 2003: 1024.
- Goldberg SB. Diagnostic ultrasound. Philadelphia:Lippincott-Raven; 1998. p. 923-5.
- Diamond DA. Adolescent varicocele. Curr Opin Urol 2007; 17(4):263-7.
- Gat Y, Bachar GN, Zukerman Z, Belenky A, Gornish M. Varicocele: a bilateral disease. Fertil Steril Feb 2004; 81(2):424-9.
- Chen SS, Chen LK. Risk factors for progressive deterioration of semen quality in patients with varicocele. Urology 2012; 79(1):128-32.
- Vazquez-Levin MH, Friedmann P, Goldberg SI, Medley NE, Nagler HM. Response of routine semen analysis and critical assessment of sperm morphology by Kruger classification to therapeutic varicocelectomy. J Urol 1997; 158(5):1804-7.
- Evers JL, Collins JA. Assessment of efficacy of varicocele repair for male subfertility: a systematic review. Lancet 31 2003; 361(9372):1849-52.
- Hopps CV, Goldstein M. Varicocele: Unified Theory of Pathophysiology and Treatment. AUA Update Series 2004; 23:90-95.
- Kocakoc E, Serhatlioglu S, Kiris A, Bozgeyik Z, Ozdemir H, Bodakci MN. Color doppler sonographic evaluation of inter-relations between diameter, reflux and flow volume of testicular veins in varicocele. Eur J Radiol 2003; 47(3): 251-6.
- Tasçi AI, Resim S, Caskurlu T, et al. Color Doppler ultrasonography and spectral analysis of venous flow in diagnosis of varicocele. Eur Urol 2001; 39(3):316-21.
- Pierik FH, Dohle GR, van Muiswinkel JM, Vreeburg JT, Weber RF. Is routine scrotal ultrasound advantageous in infertile men? J Urol 1999; 162(5):1618-20.
- Lee J, Binsaleh S, Lo K, Jarvi K. Varicoceles: The diagnostic dilemma. J Androl 2008; 29:143–6.
- Meacham RB, Townsend RR, Rademacher D, Drose JA. The incidence of varicoceles in the general population when evaluated by physical examination, gray scale sonography and color Doppler sonography. J Urol 1994 Jun; 151(6):1535-8.
- Battino J,Battino A.Diagnosis of varicocele by Doppler effect.J Mal Vasc1989;14(4):339-420.
- Nabahati M,Kasayan AA,Bijani A,Mehraban AR.Assessment of consistency rate of clinical grading of varicocele and sonography finding(persian).J Babol Univ Med Sci 2011;13(2):76-80.
- Karami M, Mazdak H, Khanbabapour s, Adibi A, Naser N.Determination of the best position and site for color Doppler ultra sonographic evaluation of the testicular vein to define the clinical grades of varicocele ultra sono graphically. Adv Biomed Res 2014; 3: 17

