
Manuscript accepted on :
Published online on: --
Plagiarism Check: Yes
Mehdi Moghtadaei1, Babak Otoukesh1, Peyman Kaghazian2, Negin Hatami3 , Bahram Boddouhi1 and Ali Yeganeh1*
1Department of Orthopedic Surgery, Rasoul-e-Akram Hospital, Iran University of Medical Science, Tehran, Iran 2Department of Orthopedic Surgery , Universitätsklinikum Bonn , Bonn , Germany 3MD, Zanjan University of Medical Science , Zanjan , Iran. Corresponding author Email: yeganeh471@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/954
Abstract
Antegrade intramedullary femoral nailing (AIFN) is used as the preferred treatment for diaphyseal and subtrochanteric femur fractures. Nevertheless, clinically important complications associated with obtaining nail entry including loss of hip abductor strength, chronic hip pain, heterotopic ossification and femoral head osteonecrosis have been previously shown.This study was aimed to evaluate the risk of injury to the superior gluteal nerve when Ante-grade femoral nailing is used for insertion. In current study, 25 patients with femoral shaft fractures were included in this study that 21 were male with an average age of 25.40 years, Also 4 cases were female with an average age of 28.20 years. The patients were between the ages of 93 to 05 years. EMG-MCV was taken from all patients and were reported by neurologist. Plain radiographs were taken from all patients. Pain intensity of patients in the last month were identified from 4 to 944 according to the patients statements. The frequency of patients with subjective lameness separately with or no signs was determined. In terms of the pain score, its average among all patients was calculated to be 4.92, while the average of 4.75 among men was calculated. Among women, the average was 5.60. All patients had a mean duration of 3.64 months for using crutches, that the average duration of 3.80 months for men and 3 months for women were calculated.In terms of subjective limping, 15 patients (60%) complained from limping, while 10 people were not affected (40 %), of which, 12 patients (80%) was belonged to men group and 3 patients (20%) were assigned in women group. 5 patients were diagnosed with atrophy of gluteus medius and gluteus minimus muscles that, 3 patients were male (60%) and 2 cases (40%) were women respectively. EMG-NCV indicated that the Superior gluteal nerve injury had occurred in 2 patients (8%) and myogenic damage of gluteus medius and gluteus minimus muscles in 5 patients (20%). Our study indicated that the superior gluteal nerve injury had occurred in 2 8% of patients and myogenic damage of gluteus medius and gluteus minimus muscles in 20%.
Keywords
Ante-grade femoral nailing; Gluteus; Lameness; Patient; Injury
Download this article as:| Copy the following to cite this article: Moghtadaei M, Otoukesh B, Kaghazian P, Hatami N, Boddouhi B, Yeganeh A. Risk of Superior Gluteal Nerve Injury After Using Ante-Grade Femoral Nailing. Biomed Pharmacol J 2016;9(1) |
| Copy the following to cite this URL: Moghtadaei M, Otoukesh B, Kaghazian P, Hatami N, Boddouhi B, Yeganeh A. Risk of Superior Gluteal Nerve Injury After Using Ante-Grade Femoral Nailing. Biomed Pharmacol J 2015;9(1). Available from: http://biomedpharmajournal.org/?p=7127 |
Introduction
Antegrade intramedullary femoral nailing (AIFN) is used as the preferred treatment for diaphyseal and subtrochanteric femur fractures. Nevertheless, clinically important complications associated with obtaining nail entry including loss of hip abductor strength, chronic hip pain, heterotopic ossification and femoral head osteonecrosis have been previously shown.
Previous studies have reported that up to 40 % of postoperative AIFN patients experience hip pain that interferes with daily activity (1;2).
The pain in the lateral hip together with the difficulty of nailing has been reported using the antegrade approach in obese patients and those with multiple injuries (3).
This has been suggested in patients with multiply-injureies and those with spinal injuries, fractures of the hip, acetabulum or tibia, pelvis and for bilateral injuries. the technique has been described, but in current study we compared with antegrade nailing. The differences in probable damage to hip abductor musculature, the superior gluteal neurovascular bundle and the deep branch of the medial femoral circumflex artery (MFCA) have been evaluated in cadaveric and clinical studies (4; 5; 6). Abduction weakness and limping is a well-recognized complication of closed antegrade insertion of femoral nails. Iatrogenic injuries to the superior gluteal nerve and the gluteus medius muscle are the most contributing parameters. Bain et al.(7) reported that, a minimum of twenty-four months postoperatively,41% of thirty-two patients in whom an isolated femoral shaft fracture had been fixed with an intramedullary nail on a fracture table limped. Heterotopic ossification in the trochanteric region secondary to the gluteal muscle injury has also been sugessted to be a cause of limping and abductor weakness after intramedullary. Ozsoy et al (8) indicated that, the risk of injury to the superior gluteal nerve and the gluteus medius muscle during closed antegrade insertion of a femoral nail is lessened by increasing the amount of hip flexion and adduction. Knowing the advantages and disadvantages of different methods or technique are effective to reduce the morbidity, disability and period of stay in the hospital and also the risk of injury to the superior gluteal nerve. Therefore, this study aimed to assess the evaluate the risk of injury to the superior gluteal nerve when Ante-grade femoral nailing is used for insertion.
 |
Figure 1: The frequency of patients according to sex
|
 |
Figure 2: The frequency of lameness subjective according to sex
|
 |
Figure 3: The frequency of organ failure according to sex
|
Materials and Methods
This case series study was conducted to evaluate the risk of injury to the superior gluteal nerve when Ante-grade femoral nailing is used for insertion.
In 1389, patients with femoral fractures have been treated in Rasol Akram hospital, Iran using Ante-grade femoral nailing method. The patients were between the ages of 93 to 05 years. After the general description of the project plan, a group of patients were enrolled in the project. EMG-MCV was taken from all patients and were reported by neurologist. Plain radiographs were taken from all patients. The patient’s data such as age, gender, body mass index entered in study. Patients with neurological disorders (previously confirmed by the specialist), the presence of fractures of the acetabulum, patients with a history of diabetes, any type of immunodeficiency disease, cancer and malignancy were removed from the list, as well as long-term use of corticosteroids (over 8 months). Pain intensity of patients in the last month were identified from 4 to 944 according to the patients statements. We assigned the total distance that patients were able to traverse . The frequency of patients with subjective lameness separately with or no signs was determined. Moreover, actual foot length was measured to determine the probable errors in surgery and lower leg length if will happen. The exact frequency of superior gluteal nerve and the gluteus medius and gluteus minimus muscles were determined according to neurologist from EMG-MCV patients and were compared by sex categories.
 |
Figure 4: The frequency of muscle atrophy according to sex
|
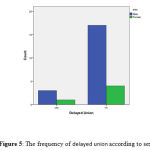 |
Figure 5: The frequency of delayed union according to sex
|
Surgical Techniques
After prop and drep and general anesthesia or regional, the patient was placed in the lateral position. Skin incision was down at the top of the greater trochanter in skin as much as 5 cm. medius and gluteus minimus muscles gently set aside, and the entrance was marked with a guide wire. In all patients, the surgical approach was entering from the piriformis cavity. The path of the wire was controlled in view of the anterior – posterior and lateral using image intensifier. After opening the cortex with a cannulated reamer, then use the handle and hammer to be placed the nail in the medullary canal and gradually was advanced. After the nailing and x-ray control, the patients came out of anesthesia and in the absence of serious problems were transferred to the ward. A plain radiograph of the patient’s bone at the fracture site was used to determine whether the fracture is healing or not, as well as to determine the superior gluteal nerve damage or Gluteus medius muscle damage (rom EMG-MCV) 6 months after surgery. Patients’ demographic characteristics and variables such as severity of pain and postoperative complications and short-term use of crutches and lower leg long and subjective limping were collected by questionnaire.
Statistical Analysis
All quantified data were presented as mean ± SD. Statistical analyses were performed using SPSS 19.0 software (Chicago, Ill., USA). Independent T test was used to compare mean quantitative, and qualitative comparison were analyzed using the χ 2.
Results
Patients with femoral fractures have been treated in Rasol akram hospital, Iran using Ante-grade femoral nailing method. The average age of 10.92 years was calculated (SD = 10.92 years). Of those, 21 were male with an average age of 25.40 years with a standard deviation of 12.05, Also 4 cases were female with an average age of 28.20 years (SD=3.83).
In terms of the mechanism of injury in all patients, 12 patients were referred to hospital due to a motorcycle accident with a car, 8 patients due to motorcycle accident with a pedestrian and 5 patients due to a car accident with a pedestrian. In this study, all patients had femur fractures of which, 18 patients had fractures of the lower extremities in right side and 7 patients with left lower extremity fracture. Moreover, 3 cases had an ipsilateral fracture of tibia and fibula at the same time. To evaluate postoperative complications in patients, the pain score (from 0 to 10 as the least amount of pain and the greatest amount of pain), Duration of crutches per month and the amount of delayed union were evaluated. Moreover, Delayed or lack of repair (Non- Union), were evaluated. Furthermore, all patients underwent EMG-NCV to evaluate the amount of neurogenic and myogenic damages in our study. In terms of the pain score, its average among all patients was calculated to be 4.92 with a standard deviation of 3.01, while the average of 4.75 was calculated among men (SD ±3.25). Among women, the average was 5.60 with a standard deviation of 1.81.
All patients had a mean duration of 3.64 months for using crutches (SD ±.01 3), that the average duration of 3.80 months (SD± 1.47) for men and 3 months (SD± 1.58) for women were calculated.
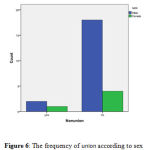 |
Figure 6: The frequency of union according to sex
|
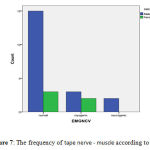 |
Figure 7: The frequency of tape nerve – muscle according to sex
|
In terms of subjective limping, 15 patients (60%) complained from limping, while 10 people were not affected (40 %), of which, 12 patients (80%) was belonged to men group and 3 patients (20%) were assigned in women group. 5 patients were diagnosed with atrophy of gluteus medius and gluteus minimus muscles that, 3 patients were male (60%) and 2 cases (40%) were women respectively. EMG-NCV indicated that the Superior gluteal nerve injury had occurred in 2 patients (8%) and myogenic damage of gluteus medius and gluteus minimus muscles in 5 patients (20%). After checking and using control graph, it was observed that in 4 cases (16%) restoration was delayed. With regard to sex, 5 men (25%) were suffered delayed union or nonunion, while two of the women (40%) had diagnosed with one of these complications.
Discussion
Femoral shaft fractures are the most common injuries, which are the result of severe trauma in young age. Knowing the advantages and disadvantages of different methods or technique are effective to reduce the morbidity, disability and period of stay in the hospital and also the risk of injury to the superior gluteal nerve. Various authors performed and compared the outcome of their techniques in interlocking femoral nailing. A previous study by Jevoor (9) reported that the majority of the patients were belonged to age group of 24 to 81 years old. In our study, the mean age of patients was also 25.16 years old. They documented that about 18 persons (90%) of femur fractures had occurred after road accidents and the incidence of accidents is increasing day by day.
According our study, the most common accidents were motorcycle and car accidents in 12 patients. Secondly, motorcycle accident with pedestrians, which has been observed in 8 patients, while car accident with pedestrians had lowest frequency of femoral shaft fractures femoral shaft fractures has been previously reported by studies (10;11). Previous studies reported that between 2-10% of treated fractures may be non-union fractures that that was 12% in the preset study (12; 13). In a systematic overview by (Bhandari, 2000) 7% non union rate was reported (14),while in the studies performed by Kempf et al 7.6% (15), Wiss et al 1.8% (16), Klemm & Borner (17)1.5%, Christie et al. 1.6%(18), O’Brien et al.(19) 4.8%, Nowotarski & Brumback (20) 5.1%.The good performance may be due to better treatment strategy and careful selection of operative procedure and surgeon’s experience.
Today, the most common method for femoral nailing is Reamed Intramedullary nailing for primary injuries, but antegrade intramedullary nailing is a therapeutic method based on fracture properties and is used in the sole discretion of the surgeon (10;11, 14; 21). Wolinski et al(22) conducted a study on 551 femoral fractures treated with intramedullary nailing. The results of mentioned study showed that 98.5% of fractures of the fractures were union, and the rate of nonunion , infection and equipment disorder were very low. In our study, 72% of 25 cases were treated using Intramedullary nailing method for femoral shaft fractures that suitable union was observed. Harris et al (23) indicated that 13 (23%) of 54 patients with femoral shaft fractures required reoperation due to delayed or non-union fractures. In a study, 2 patients with less than 1 cm and 2 of them at a rate of 1 to 2 cm were suffering from lower limbs (9). Moreover, incidence of 3.1% for lower limbs has been reported in patients (24). Harris et al (23) characterized that 43% of patients had significant differences in organs size. In this study, Out of 25 patients, 5 patients (20%) had lower limb long. In current study, the average duration of crutches and non weight bearing was calculated to be 3.64 months that this time in the men’s group was 3.80 months and in the women was 1.58 months. The average weight bearing has been previously shown to be about 11 weeks. However, 20% of patients were not allowed to have mobility (25). In a study on the patients with bone fractures, it has been showed that 3% of patients had femoral shaft fractures and 42% of treated patients with lower limb long had subjective limping (7). Although, using Ante-grade femoral nailing provides treatment of many femoral shaft fractures, but was associated with complications such as nerve damage, pain, lower limb and subjective limping. Our study indicated that the superior gluteal nerve injury had occurred in 2 8% of patients and myogenic damage of gluteus medius and gluteus minimus muscles in 20%. Further investigations are required to find a way to reduce these complications.
References
- Bednar DA, Ali P . Intramedullary nailing of femoral shaft fractures: reoperation and return to work. Can J Surg 1993;36(5): 464–466.
- Dodenhoff RM, Dainton JN, Hutchins PM () Proximal thigh pain after femoral nailing. causes and treatment. J Bone Joint Surg Br 1997;79(5): 738–741.
- Ostrum R, DiCicco J, et al. Retrograde intramedullary nailing of femoral diaphyseal fractures. Presented at the Orthopaedic Trauma Association, Louisville, KY, 1997.
- Ansari Moein CM, Verhofstad MH, Bleys RL et al .Soft tissue anatomy around the hip and its implications for choice of entry point in antegrade femoral nailing. Clin 2008;568–574.
- Lowe JA, Min W, Lee MA et al . Risk of injury to the superior gluteal nerve when using a proximal incision for insertion of a piriformis-entry reamed femoral intramedullary nail: a cadaveric study. J Bone Joint Surg Am 2012;94(15):1416–1419.
- Ansari Moein C, ten Duis HJ, Oey L et al . Functional outcome after antegrade femoral nailing: a comparison of trochanteric fossa versus tip of greater trochanter entry point. J Orthop Trauma 2011;25(4):196–201.
- Bain GI, Zacest AC, Paterson DC, Middleton J, Pohl AP. Abduction strength following intramedullary nailing of the femur. J Orthop Trauma1997;11(2):93-7.
- Ozsoy MH, Basarir K, Bayramoglu A, Erdemli B, Tuccar E, Eksioglu MF. Risk of superior gluteal nerve and gluteus medius muscle injury during femoral nail insertion. J Bone Joint Surg Am. 2007 Apr;89(4):829-34.
- Jevoor R. Study of surgical management of diaphyseal fractures of femur in adults treated with intramedularry interlocking nails. Karnatak institute of medical science 2005:1-122.
- Bennett FS, Zinar DM, Kilgus DJ. Ipsilateral hip and femoral shaft fractures. Clin Orthop Relat Res 1993;296:168-77.
- Wu CC, Shih CH. Ipsilateral femoral neck and shaft fractures. Retrospective study of 33 cases. Acta Orthop Scand1991;64:346-51.
- Harper MC, Carson WL. Curvature of the femur and the proximal entry point for an intramedullary rod. Clin Orthop 1987;220:155-61.
- Swiontkowski MF. Ipsilateral femoral shaft and hip fractures. Orthop Clin North Am1987;18:73- 84.
- Pape HC, Grimme K, van Griensven M, Sott AH, Giannoudis P, Morley J, Roise O, EllingsenE,Hildebrand F, Wiese B, Krettek C. Impact of intramedullary instrumentation versus damagecontrol for femoral fractures on immune inflammatory parameters: prospective randomized analysis by the EPOF study group. J Trauma. 2003;55:7-13.
- Kempf I, Grosse A, Beck J. Closed locked intramedullary nailing: its application to comminuted fractures of the femur. J Bone Joint Surg1985;67A: 709-20.
- Wiss DA, Brien WW, Becker V. Interlocking nailing for the treatment of femoral fractures due to gunshot wounds. JBone Joint Surg1991; 73A:598-606.
- Klemm K, Borner M. Interlocking nailing of complex fractures of the femur and tibia. C/in Orthop. 1986;212: 89-100.
- Christie I, Court-Brown C, Kinninmonth AWG, Howie CR. Intramedullary locking nails in the management of femoral shaft fractures. J Bone Joint Surg. 1988;70B: 206-10.
- O’Brien PJ, Meek RN, Powell IN, Blackat PA. Primary intramedullary nailing of open femoral shaft fractures. J Trauma.1991; 31:113-6.
- Nowotarski P, Brumback RJ. Immediate interlocking nailing of fractures of the femur caused by low- to mid velocity gunshots. J Orthop Trauma. 1994;8(2):134-141.
- Whittle AP, George W. Wood II: Fractures of lower extremity. In: Canale T, editor. Campbell’s Operative Orthopaedics. Philadelphia: Mosby; 2003. 2725-2872.
- Wolinski PR, Mc Carthy E, Shyr Y, Johnson K. Reamed intera medullary nailing of femur: 551 cases. J Trauma1999;46:392-9.
- Harris I, Hatfield A, Donald G, Walton J. Outcome after intramedullary nailing of femoral shaft fractures. ANZ J Surg2003;73(6):387-9.
- Watson JT, Moed BR. Ipsilateral femoral neck and shaft fractures: complications and their treatment. Clin Orthop Relat Res 2002;399:78-86.
- Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip1987;18:1-206.

