
Vijayashri Sakthi1, B. Saravanan2 and E. Thulasiram2
1Senior lecturer, Tagore Dental College and Hospital, Chennai, India. 2Department of Orthodontics, Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, Chennai-600100
DOI : https://dx.doi.org/10.13005/bpj/754
Abstract
Bimaxillary protrusion is a condition warranting retraction of upper and lower incisor for optimizing their axial inclination to obtain lip competency and for straightening the profile. These cases generally require maximum conservation of anchorage since the entire retraction space must be utilized for retracting the incisors with protracted treatment time. Demineralization of a thin layer of bone over a root prominence after corticotomy surgery can optimize the response to applied orthodontic forces. The current technique employed a modified stage of corticotomy procedure which utilizes the principle of Regional acceleratory phenomenon, in addition Demineralized freeze dried bone was also used to augment the periodontal apparatus. The current modification is relatively simple, less invasive and can be done under local anesthesia as an outpatient procedure. The results conclusively prove that selective alveolar decortication is effective for retraction, reduces the retraction time by half in addition to conserving anchorage.
Keywords
Corticotomy assisted retraction; Selective alveolar decortications; En-masse retraction
Download this article as:| Copy the following to cite this article: Sakthi V, Saravanan B, Thulasiram E. A-One Stage Corticotomy Assisted Orthodontic Technique for Accelerated Retraction. Biomed Pharmacol J 2015;8(October Spl Edition) |
| Copy the following to cite this URL: Sakthi V, Saravanan B, Thulasiram E. A-One Stage Corticotomy Assisted Orthodontic Technique for Accelerated Retraction. Biomed Pharmacol J 2015;8(October Spl Edition). Available from: http://biomedpharmajournal.org/?p=3436> |
Introduction
Bimaxillary protrusion is a condition characterized by protrusive and proclined upper and lower anterior teeth and an increased procumbency of the lips1, many patients with bimaxillary protrusion seek orthodontic treatment to decrease this procumbency. During retraction, the characteristics of the anterior alveolar bone can resist the efforts to remodel bone. The anatomic limits set by the cortical plates of the alveolus at the level of the incisor apices act as barriers to incisor retraction.
Corticotomy is one of the surgical procedures that is commonly used in which only the cortical bone is cut and perforated but not the medullary bone. In 1959, Köle2 introduced a technique called selective alveolar decortications to enable movement of a bone segment that included a tooth by sectioning the layer of compact bone. In 2001, Wilcko et al3 developed a new treatment method combining corticotomy, alveolar augmentation, and orthodontic treatment. They have observed that orthodontic tooth movement is accelerated by the increase of bone turnover and decrease of bone density because osteoclasts and osteoblasts are increased due to a regional acceleratory phenomenon (RAP).4, 5
Concept and Indication
Stages of active orthodontic treatment depending on Class of malocclusion and extraction or nonextraction treatments, emphasizes the stage requiring the greatest tooth movement. For extraction cases, the limited duration of the corticotomy (Selective alveolar decortications) effect might be best applied during the retraction stage of treatment, when the greatest tooth movements are required.6
Indications
- Bimaxillary protrusion cases with proclined incisors.
- Cases with aligned arches and crowding ‹3mm.
- Cases requiring all first bicuspid extraction.
- Dentoalveolar to moderate alveoloskeletal malocclusions
The potential advantages of the treatment in comparison with traditional orthodontics are
- Increased rate of tooth movement.
- Increased alveolar volume and a more structurally complete periodontium.
Undecorticated segment serves as better source of anchorage.
Technique
Initial Preparation Stage
A treatment plan was developed by the orthodontist/ surgeon team to determine the teeth that will undergo bone activation, anchorage, and the teeth that will need to be extracted.
Typically, the orthodontic brackets were placed and a light wire engaged with 0.022’ slot Roth appliance. Leveling and aligning (Fig. 1) was carried out until 0.019”X 0.025” stainless steel archwire could be fully engaged in the bracket slot, the first premolars were not-extracted till the time of selective alveolar decortications stage.
 |
Figure 1: Leveling and aligning |
Stage of Selective alveolar decortications (SAD)/ Corticotomy:
Corticotomy after orthodontic alignment. A single arch requiring selective decortications can require 1/2 hour to 1hour carried out under local anesthesia (Lignox 2%A). Lower arch (Fig 2) procedure preceded 2 weeks ahead of the upper arch. First premolars were extracted at the time of the surgery and a stainless steel 0.019” × 0.025” archwire with soldered brass hooks was placed before flap elevation .
Sulcular incisions from the distal aspect of one canine to the contralateral canine were placed, and full thickness flap was elevated, 3 mm above the apical region of the tooth. 701 fissure bur and number 2 size round bur mounted on a micromotor handpiece under copious
irrigation was used for decortications (only cortical surface scoring and not through and through penetration). If there was a good amount of inter‑root distance between two adjacent teeth vertical interdental cortical surface scoring was done otherwise only surface punch hole were placed in the area, stopping 2 mm short of the alveolar crest, occlusally. Horizontal decortications connected the vertical 2 mm beyond root apex. Selective alveolar decortication from the mesial aspect of one canine to the mesial surface of the contralateral canine involving the anteriors was performed. Similarly, a palatal flap incision was raised immediately for decortications of the superficial surface of the palatal bone for RAP to occur (Fig. 2, 3). The graft was placed only in cases with evidence of bone loss (dehiscence and fenestration) on flap elevation . Demineralized demineralized freeze‑dried bone allograft, wetted with sterile saline and maintained in the desired position by full thickness flap, sutured with an interrupted loop, nonresorbable 4‑0 black silk suture material, left in place for 1–2 weeks.
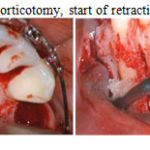 |
Figure 2: Mandibular corticotomy, start of retraction 1 week post operative. |
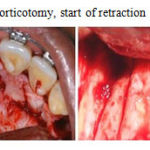 |
Figure 3: Maxillary corticotomy, start of retraction 1 week post operative |
Stage of Retraction
Initiation of orthodontic force was done within 5–7 days after the surgery with the help of closed NiTi coil spring which was engaged from the first molar tube to the soldered hook on the archwire delivering a force of 250 g for en‑masse retraction using sliding mechanics. (Fig 4)
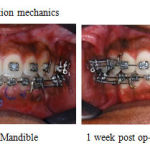 |
Figure 4: Retraction mechanics |
Discussion
In the treatment of bimaxillary protrusion, two important factors for consideration are: esthetic improvement of the dentofacial area and the establishment of the stable dental relationship that embodies the requirement of line of occlusion. Time is an important factor during the course of orthodontic treatment. Corticotomy (selective alveoloar decortictation) can be effectively used to correct dentoalveolar and moderate alveoloskeletal problems. As the severity increases from alveoloskeletal to pure skeletal problems osteotomy and/or distraction osteogenesis would be the choice of treatment.
In Wilcko’s7 protocol corticotomy was performed prior to aligning and an additional procedure namely Ostectomy (surgical removal of cortical plate) in the extraction space was required which is both cumbersome and expensive to the patient because of additional grafting required in the area. The procedure employed in our study has the advantage of being less invasive, is done under local anesthesia and is a simpler technique.
Case selection with minimal crowding helps to maintain the tooth within the cortex during leveling and aligning stage. Thus the first bicuspids were delayed and extracted to act as a fresh extracted socket and reduced bony resistance to retraction, an added advantage to accelerated retraction. The use of rigid archwires during and after selective alveolar decortications provided controlled retraction of the anteriors whereas the undecorticated posterior segment acted as good source of anchorage module.
Aboul Ela et al8 who reported that the rate of space closure peaked during the end of 1st and 2nd month and reduced by the end of 4th month. This could be biologically co-related with the transient RAP phenomenon as mentioned by Frost4 which remains active for 4 months. For extraction, the limited duration of the corticotomy effect might be best applied during the retraction stage of treatment, when the greatest tooth movements are required.
Table 1: Selective Alveolar Decortication
| Key Characteristics | Traditional technique | Current Modified technique |
| Decortication timing | · Beginning of orthodontic treatment.
· SAD as required throughout therapy. |
SAD planned just before stage of retraction. |
| Exraction of teeth | At the start of treatment. | Delayed extraction along with SAD |
| Flap reflection | Buccal and lingual in cases of retraction | Buccal and lingual for en- masse retraction. |
| Activation intervals | Biweekly | Continuous moderate force. |
| Archwire | Flexible Niti archwires during decortication procedure. | Rig.id archwires during decortications procedure. |
| Indications | · Accelerated tooth movement.
· Mild to moderate crowding. · Mild to moderate arch development. · Extraction site closure |
· Accelerated tooth movement in extraction cases.
· En-masse retraction. · Bimaxillary protrusion cases with mild crowding. |
Conclusion
Corticotomy assisted retraction drastically reduces the overall duration of Orthodontic treatment. It is particularly useful in maximum anchorage cases since by Selective decortications the anchorage segment can be made virtually stationary and the entire extraction space can be utilized for retraction. This novel technique also allows the possibility for severely proclined anterior to attain ideal axial inclination within the alveolar trough and retain stable occlusion.
Bibliography
- Lewis SJ- Bimaxillary Protrusion. Angle Orthod. 1943;13:51-59.
- Köle H: Surgical operations of the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol. 1959; 12: 515-529.
- Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int J Periodontics Restorative Dent 2001;21: 9‑
- Frost HM. Biology of fracture healing – An overview for clinicians Part I and II. Clini Orthop Relat Res 1989;248:283
- Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon in the mandible following mucoperiosteal flap surgery. J Periodontol 1994;65: 79‑
- Peter H. Buschang, Phillip M. Campbell, and Stephen Rus. Accelerating Tooth Movement With Corticotomies: Is It Possible and Desirable?. Semin Orthod 2012;18:286-294.
- Wilcko MT, Wilcko WM, Bissada NF. An evidence‑based analysis of periodontally accelerated orthodontic and osteogenic techniques: A synthesis of scientific perspectives. Semin Orthod 2008;14: 305‑
- Aboul-Ela SMB, Beialy AR, El-Sayed KMF, Selim EMN, EL-Mangoury NH, Mostafad YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthodontics and Dentofacial Orthopedics 2011;139: 2.

