
Fatemeh Ghavi1, Leili Mosalanejad2, Masomeh Golestan3 and Sahabeh Etebariy3
1Midwifery Department, Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran 2Mental Health Department, Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran 3Research and Clinical Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
DOI : https://dx.doi.org/10.13005/bpj/860
Abstract
Aim: Investigation holistic Stress in infertile women and relation to demographic Characteristics in women who referred to Yazd infertility center by cross sectional descrpitive study. This study was carried on 400 infertile women who referred to Yazd Infertility Center between 2013-2014. These participants were selected by purposive sampling method. Data were collected using demographic characteristics’ questionnaire, Coudron Stress Test and Perceived Stress Test. Relation between demographic variables and stress obtained from Inferential statistics. Mean score of perceived stress and all level of life, personality and health stress is higher than other causes , when the causes is related to common causes, but there are not any significant difference between them. There are significant difference in stress mean score from duration of infertility. (p<0.05).Positive perceived stress in common causes of infertility and negative perceived stress in unknown causes were higher than other one .There was not any significant difference between educational level, age and stress (p>0.05). Results highlights infertility has a significant impact on the infertile women's mental health. It is important psychological approach consider as an important part of treatment inside other medical treatments.
Keywords
Infertility; Perceived stress; Depression; Anxiety; Stress
Download this article as:| Copy the following to cite this article: Ghavi F, Mosalanejad L, Golestan M, Etebariy S. The Investigation Holistis Stress in Infertile Women and Relation to Demographic Characteristics in Women Who Referred to Yazd Infertility Center. Biomed Pharmacol J 2015;8(2) |
| Copy the following to cite this URL: Ghavi F, Mosalanejad L, Golestan M, Etebariy S. The Investigation Holistis Stress in Infertile Women and Relation to Demographic Characteristics in Women Who Referred to Yazd Infertility Center. Biomed Pharmacol J 2015;8(2). Available from: http://biomedpharmajournal.org/?p=1885 |
Introduction
Infertility is a major life crisis that leads to serious psychological problems and stressful experiences for infertile people(Sadock et al., 2003).According to the World Health Organization(WHO), fertility rates vary in different parts of the world, but its average is 20 percent (Ramezanzadehet al., 2004a).Wichman et al Studies show that infertility is such a complex experience in terms of psychology that can increase depression in some women(Wichmanet al., 2011). Gourounti et al also suggest that infertility and its treatment are severe stress derivers (Gourountiet al., 2012).Some researchers such as Connolly et al speculate that damaging psychological factors play a major and pathogenic role in infertility .Connolly et al in their research also suggest that infertility causes many mental health problems of infertile cases that these problems can consequently contribute to some infertility treatments. For instance, the stress derived by delaying o rpreventing ovulation may affect the outcome of medical treatment(Connollyet al., 1992).Infertility-induced stress is defined as the interaction between the physical conditions that lead to infertility and medical interventions ,reactions of others and mental characteristics of the individual that may accompany the individual for along time and relapse with any diagnostic or therapeutic intervention including treatment for IVF and other infertility treatments. Numerous medical tests and limb inspection, the long-term treatment of infertility, low rate of treatment success as well as the economic problems caused by infertility treatments include severe stressors for infertile individuals(Covington, Hammer, 2007).
Mollaiy Nezhad et al in their study found that all infertile couples suffered from infertility stress to varying degrees and about 46 percent of them didn’t have marital compatibility (Mollaiy Nezhadet al., 2000).Studies have shown that8 6percent of infertile women are involved with infertility stress in their lives(Ramezanzadehet al., 2004).Newton et al in their study showed that infertile couples in particular experience the stress of infertility indifferent aspects including the stress related to the need for being a parent(Newtonet al., 1999).Other researchers showed that due to the low success rate of IVF treatment, involvement in infertile women with infertility stress is understandable(Seible, 1997).Litzinger and Gordon stated that 80% of infertile patients suffer from a psychological disorder,including marital dissatisfaction, disturbance in relationships especially between the couples, the rage and negative emotional effects(Litzinger, Gordon, 2005).Several mechanisms have been proposed for the effects of stress on fertility including impairing secretion of gonadotropins, also anxiety leads to infertility intensification by an increase in cortisol, prolactin(Cooperet al.,2007; Karlidere et al., 2008).Women in infertile couples reported greater psychological symptoms (anxiety and depression) and more decreased marital adjustment than men in infertile couples; but the couples did not show any significant difference with those in control groups regarding these common parameters(Burns, Covington, 2000).Due to the relatively high incidence of infertility and relation between psychosocial symptom and cultural basis in infertile people, we were to examine the complete stress of infertile women (in the dimensions of life, personality and health stress) and to determine its relationship with demographic factors such as duration of infertility, duration of marriage ,cause of infertility, age, occupation and education.
Aim
This study was performed with the aim of examining the holistic stress in infertile women and its association with demographic factors(Sn- causes of infertility-duration of marriage, age, education& job) on women referring toYazd Infertility Center. The data gathering tools have included demographic data and as second section of the questionnaire included perceived stress and holistic coudron stress.
Methods
Design
This cross sectional study was carried out on 400 infertile women who referred to Yazd infertility center between 2013-2014.
Sample
The research population was considered all infertile women referring to Infertility Center in Yazd and the research samples were about 400 individuals regarding the prevalence of infertility.
Data Collection
The data gathering tools were a questionnaire of perceived stress scale and Coudron stress test. Cohen et al. perceived stress questionnaire was made in 1983. The scale has 14 items and each item is answered on the basis of a five-point Likert scale(none, low, medium, high and very high); these options are scored in the order of 0, 1, 2, 3 and 4 and include positive and negative sub scales of perceived stress.
Internal consistency reliability coefficients of the scale have been achieved through Cranach’s alpha coefficient in the range of 0.84 to 0.86 in two groups of students and a group of smokers who were on the giving-up smoking program. This scale is a useful tool for assessing overall stress experienced in different age groups. Cranach’s alpha coefficients for this scale are obtained 0.88 and 0.81, respectively.
For reviewing holistic stress in various areas, Coudron stress questionnaire was used. This questionnaire is standardized and has good reliability and validity in several studies.
In repeated use of the questionnaire, validity and reliability of instruments were in all cases higher than 7.0 and was 8/0, respectively. The applied tools consist of several sections that investigate life, personality– health and institutional stresses. Given that a large portion of the samples were house wives and it was not possible to study workplace stress in them, therefore, this part of the questionnaire was removed and only the other three sections were evaluated. The first section contained 23 questions that measured personality-driven stress and Intellectual habits of the patients. In this section, some cases such as dissatisfaction with life, worry about the future, feelings of internal anxiety and guilt have been assessed. The second part consisted of 16 questions that were used to measure the level of stress in personal life, more over, cases such as divorce, relationship and family conflicts, economic and job concerns were explored. The grading of this type of stress is as follows: lower than 15 as normal, between 15 and 40 as not having a satisfactory life and higher than 40 means that you live in stressful condition so there is the possibility of burnout.
The questions were two-choice questions in a “Yes”, “No” fashion. For grading the questions, standard grading method of the questionnaire will be used. This means that for each positive response in the level of stressful thought habits, 1 point will be considered and finally, with respect to the obtained scores, the score higher than 5 is considered as a stressful personality. And then the last part of this questionnaire examines health stresses. This questionnaire contains 17 questions and measures the stress caused by compliance with health issues.
Health stress which is defined as stress toward one’s own life is classified as lower than 30 (care in personal health), between 30 and 60 (health in not such that can be controlled), and higher than 60 ( life-health brings disturbance).
Data Analysis
For data analysis, descriptive statistics such asmeans and standard deviation and then correlation coefficient were used to examine the distribution of stress and analytical tests were applied to examine mean differences in terms of demographic factors.
Results
The results showed that most people aged less than 20 years and they have married for less than5yearsso they have less than a 5-yearhistory of infertility(Table 1 cite here).
Table 1: Demographic distribution in infertile women
|
Frequency (%) |
Categories |
Demographic Data |
| 228(58.5%)
116(29.7%) 36(9.2%) 10(2.6%) 390(100%) |
Lower than 20
21-30 31-40 41-50 Total |
Age
|
| 182(46.8%)
140(36%) 52(13.4%) 15(3.9%) 389(100%) |
Lower than 5
6-10 11-15 More than 16 total |
Duration of marriage
|
| 111(28.4)
80(20.6%) 147(37.6%) 53 (13.6%) 391(100%) |
Lower than 5
6-10 11-15 More than 16 total |
Case of infertility
|
| 86(21.7%)
177(43.3%) 135(34%)
|
Primary
Diploma higher |
Education level |
| 66(16.6%)
332(83.4%) |
Employer
Household |
Job |
Table2 shows that the mean score of stresses is higher than in other cases when the stress factor is in both cases. Moreover, when the cause of infertility is unknown, the mean score of stresses has been reported to be higher than that of masculine causes. (Table2 cite here)
Table 2: Distribution of stress from causes of infertility N=398
| Perceived stress | Causes of infertility | Mean | SD | CI |
| Negative conception | Male factor | 10.14 | 5.97 | (9.01-11.26) |
| Female factor | 11.03 | 5.16 | (9.87-12.18) | |
| unknown | 10.61 | 5.100 | (10.62-12.30) | |
| Both | 11.46 | 5.83 | (8.97-12.25) | |
| Positive conception | ||||
| Male factor | 13.65 | 5.31 | (12.65-14.66) | |
| Female factor | 14.15 | 4.54 | (13.29-15.32) | |
| unknown | 14.30 | 4.72 | (13.37-14.93) | |
| Both | 14.80 | 5.38 | (13.29-16.32) | |
| Cordon stress | ||||
| Life stress | Male factor | 2.02 | 0.70 | (1.88-2.10) |
| Female factor | 1.95 | 0.72 | (1.78-2.11) | |
| unknown | 2.26 | 0.69 | (2.05-2.28) | |
| Both | 2.70 | 0.69 | (2.06-2.46) | |
| Health stress | Male factor | 1.66 | 0.60 | (1.54-1.77) |
| Female factor | 1.57 | 0.52 | (1.45-1.69) | |
| unknown | 1.72 | 0.67 | (1.61-1.83) | |
| Both | 1.82 | 0.59 | (1.65-1.99) | |
| Personality stress | Male factor | 0.7 | 0.45 | (0.68-0.80) |
| Female factor | 0.66 | 0.47 | (0.55-0.77) | |
| unknown | 0.72 | 0.45 | (0.65-0.79) | |
| Both | 0.78 | 0.41 | (0.66-0.90) | |
The results of another research indicate that the level of stress varies in accordance with infertility duration, and this fact shows that there is a significant difference in positive perceptions of stress on the basis of infertility duration.(Table3 cite here)
Table 3: Stress in infertile women from duration of infertility
| Significance | X2 | Mean Rank | N | Duration. Of infertility | Variables | |
| Perceived stress test | ||||||
| 0.99 | 0.64 | 193.64 | 222 | lower than 5 years | Negative. Conception | |
| 190.87 | 116 | 6-10 | ||||
| 190.36+ | 36 | 11-15 | ||||
| 193.90 | 10 | more than 16 | ||||
| 384 | Total | |||||
| Positive .conception | ||||||
| 0.01 | 11.36 | 203.98 | 222 | lower than 5 years | ||
| 170.21 | 116 | 6-10 | ||||
| 211.08 | 36 | 11-15 | ||||
| 129.25 | 10 | more than 16 | ||||
| 384 | Total | |||||
|
courdon stress |
|||||||||
| Life stress | |||||||||
| Duration of infertility | Normal | No satisfaction | Exhaustion | X2 | value | ||||
| lower than 5 years | 51(23.1%) | 116(52.5%) | 54(24.4%) | 23.37 | 0.001 | ||||
| 6-10 | 21(18.6%) | 57(50.4%) | 35(31%) | ||||||
| 11-15 | 5(14.7%) | 11(32.4%) | 18(52.9%) | ||||||
| more than 16 | 2(22.2%) | 0 | 7(77.8%) | ||||||
| Health stress Normal Moderate High | |||||||||
| Health stress | lower than 5 years | 99(44.8%) | 103(46.6%) | 19(8.6%) | 28.26 | 0.001 | |||
| 6-10 | 32(28.6%) | 74(66.1%) | 6 (5.4%) | ||||||
| 11-15 | 16(47.1%) | 15(44.1%) | 3(8.8%) | ||||||
Table 4 shows that there is no significant difference in people’s stress based on infertility factor.(table 4 cite here)
Table 4: Stress in infertile women from causes of infertility
 |
Table 4: Stress in infertile women from causes of infertility: |
This graph represents that,when infertility exists with an unexplained cause, the mean of negative perception of stress has been observed more than others cases. (Figure1 cite here).While a positive perception of stress is observed to be higher than other cases when both couples are causes of infertility.(Figure2 cite here)
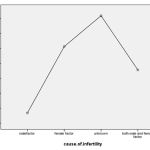 |
Figure 1 |
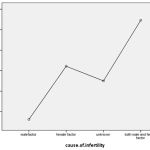 |
Figure 2 |
Discussion
According to the results of the present study that aims to examine holistic stresses in infertile women and its association with demographic factors ,the mean score of perceived stress (in both positive and negative perceptions subscale) was more likely than other cases when stress factors were in both individuals. The results of the study by Ogawa et al on 83 infertile Japanese women showed the effect of two factors of age and male infertility on their psychological distress and women whose husbands were infertile had significantly lower scores on psychological distress than women whose husbands were not infertile, the results of this study were inconsistent with those of the present study (Ogawaet al.,2011).
Sheiner et al recognize the reason for stress reduction in women with infertile husbands in Japanese society is that women acknowledge themselves to be responsible for infertility (Sheineret al.,2003).Moreover, the mean score of stress has been reported to be higher than feminine or masculine causes when the cause of infertility is unknown. Other results of this study showed that there was no significant difference in the stress of individuals in terms of infertility causes; in addition, a significant difference was observed in the individuals’ stress scores in both life stress and health stress groups. In our study, the mean negative perception of stress was reported to be higher than other cases when infertility existed with unexplained causes. While positive perceptions of stress were reported to be higher than other cases when both couples were the causes of infertility. Abbey et al & Domar et al found that infertility with an unknown cause increases the risk of psychological distress. (Domaret al.,1992; Abbey et al., 1992). In Franco’s study, infertile women show higher rates of psychological symptoms than their partners, especially in feminine causes and their irrationality, because women have a more important role in the treatment and it is natural that they are affected more (Franco et al.,2003).In another study by Domar, psychological distresses were higher in women with unknown cause of infertility(Domar et al.,2000).Eszter Cserepes et al also showed that women have higher stress scores than men(Eszter Cserepes et al.,2013).Herrmannet al& Burns’ research also suggests that infertility is a major mental health problem for women while men generally suffer less psychological distresses(Herrmannet al.,2011; Burnset al.,2006). All the aforementioned results confirm the results obtained in the present study.Parallel to the results of the present study regarding the higher level of stresses in women, the results of many studies confirm the mentioned case(Petersonet al.,2012;Greilet al.,2010).Other studies on infertile couples also suggest that psychological symptoms are higher in women than in men(Fatoyeet al.,2008;Eren Bodur et al.,2013;Syiem1, Jayashankar Reddy.,2013;El Kissi et al., 2013).Having conducted a study on 124 infertile couples in Malaysia, Ramli et al found that with psychological distresses were significantly higher in women compared to men(Ramliet al.,2014).In analyzing the higher level of stress in women, experts have raised several reasons. Among them is that, women undertake various methods of backbreaking infertility treatments to maintain their positions and perhaps this fact makes them more vulnerable to various psychological traumas(Grudzenet al.,2011;Halk Sagligi and Celal Bayer Univ., 2011).Noorbala et al believe that the most important factors that put pressure and stress on infertile women are the reaction of other people to infertility, loneliness and difficult infertility treatments(Noorbalaet al.,2007).Other researchers stipulate that there are significant gender differences in the perception of the infertile person of himself, it means that infertile women compared with fertile men, have a more negative conception of themselves and consider themselves as less valuable and worthy of blame; even worse, they may lose their identity as a woman(Galhardoet al.,2010).Other research results indicate that the level of stress may vary in accordance with infertility duration and in this case, there is a significant difference in positive perceptions of stress on the basis of duration of infertility. Domar et al have reported most psychological distresses in the second and third years of infertility and this rate decreases after six years of infertility, also Lok et al & et alKee, like Domar, have asserted that duration of infertility affects the couples’ stress level(Domaret al.,1992;Loket al., 2002;Keeet al., 2000).In a study by Ogawa et al, no direct relation between duration of infertility and psychological distresses has been found(Ogawa et al.,2011).Kousalya et al suggest that the levels of psychological distresses, such as stress, increase with increasing duration of infertility and this result is contrary to the results of this study that Ramezanzadeh et al also have confirmed (Kousalya et al.,2013;Ramezanzadeh et al., 2004b).
Conclusion
results highlights infertility has a significant impact on the infertile women’s mental health. Mental health professionals and consolers can educate couples regarding the ineffectiveness coping strategies as well as the stress management technique and psychological approach while experiencing the stress of infertility. Also it is important these approach consider as an important medical treatment inside medical treatments.
Ethical Aspects
The study protocol was approved by the Ethics Committee of the Jahrom University of Medical Sciences, Jahrom, Iran
Conflict of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author Contribution
F.GH was responsible for writing of paper, final editing and data analysis. L.M was responsible for idea of title, writing of paper, editing the manuscript and data analysis. M. G was responsible for sampling and overview of the manuscript.
Acknowledgements
I appreciate all participant in this study. Also executive manager, head of center of infertility and other manager In yazd infertility center.
References
- Abbey A, Halman LJ, Andrews FM. Psychosocial, treatment, and demographic predictors of the stress associated with infertility. Fertil Steril. 1992;57(1):122-8.
- Burns LH, Covington SN. Infertility counseling a holistic handbook for clinicians. London:Parthenon;2000.
- Burns LH, Covington SH. Psychology of infertility. In: Covington SH, Burns LH, editors. Infertility counseling a holistic handbook for clinicans. 2nd ed. Cambridge: Cambridge University Press; 2006. p. 1–19.
- Cohen S, Kamarck T, & Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior.1983; 24: 385-396.
- Cohen S, Williamson J. Perceived stress in a probability sample of the United States,” in The Social Psychology of Health, S. S. A. S. Oskamp, Ed., , Sage, Newbury Park, Calif, USA;1988. p. 31–67.
- Connolly KJ, Edelmann RJ, Cooke ID, Robson J. The impact of infertility on psychological functioning. J Psychosom Res. 1992; 36(5):459-68.
- Cooper BC, Gerber JR, McGettrick AL, Johnson JV. Perceived infertility-related stress correlates with in vitro fertilization outcome. Fertil Steril. 2007;88(3):714-7.
- Covington SN, Hammer Burns L. Infertility counseling.2nd ed. New York: Cambridge University Press; 2000. p.1- 17, 175-180, 493-506.
- Domar AD, Broome A, Zuttermeister PC, Seibel M, Friedman R: The prevalence and predictability of depression in infertile women. Fertil Steril. 1992;58:1158-1163.
- Domar AD, Clapp D, Slawsby EA, Busek J, Kessel B, Frezinger M: Impact of group psychological interventions on pregnancy rates in infertile women. Fertil Steril. 2000; 73:805-811.
- El Kissi Y , Ben Romdhane A, Hidar S, Bannour S, Ayoubi Idrissi K , Khairi H, Ben Hadj Ali B . General psychopathology, anxiety, depression and self-esteem in couples undergoing infertility treatment: a comparative study between men and women. European Journal of Obstetrics & Gynecology and Reproductive Biology.2013;167:185–189.
- Eren Bodur N , Çoşar B, Erdem M. The Relationship between Dyadic Adjustment with Demographic and Clinical Variables in Infertile Couples. Cukurova Medical Journal. 2013; 38(1):51-62.
- Eszter Cserepes R , Kolla´r J , Sa´py T , Wischmann T , Buga´n A. Effects of gender roles, child wish motives, subjective well-being, and marital adjustment on infertility-related stress: a preliminary study with a Hungarian sample of involuntary childless men and women. Arch Gynecol Obstet. 2013;288:925–932.
- Fatoye FO, Owolabi AT, Eegunranti BA, Fatoye GK. Unfulfilled desire for pregnancy: Gender and family differences in emotional burden among a Nigerian sample. J Obstet Gynecol. 2008;28:408–9.Franco JG JR, Razera Baruffi RL, Mauri AL, Petersen CG, Felipe V, Garbellini E: Psychological evaluation test for infertile couples. J Assist Repord Genet. 2003;19:269-273.
- Galhardo A, J. Pinto-Gouveia, M. Cunha & Matos. “The impact of shame and self-judgment on psychopathology in infertile patients”, Human Reproduction. 2010;26 (9).
- Gourounti K, Anagnostopoulos F, Potamianos G, Lykeridou K, Schmidt L & Vaslamatzis G. Perception of control, coping and psychological stress of infertile women undergoing IVF. Reproductive BioMedicine Online. 2012;24(6):670-679.
- Greil AL, Slauson-Blevins K, McQuillan J. The experience of infertility: a review of recent literature. Sociol Health Illn. 2010; 32:140–62.
- Grudzen CR, Meeker D, Torres JM. Comparison of the mental health of female adult film performers and other young women in California. Psychiatric Services.2011;62(6):639-45.
- Halk Sagligi & Celal Bayer Univ. The relationship between domestic violence and the prevalence of depressive symptom in married women between 15 and 49 years of age in a rural area of Manisa Turkey. Turkish Psikiyatri Dergisi. 2011;22(1):6-10.
- Herrmann D, Scherg H, Verres R, von Hagens C , Strowitzki T,Wischmann T.Resilience in infertile couples acts as a protective factor against infertility-specific distress and impaired quality of life. J Assist Reprod Genet. 2011;28:1111–1117.
- Karlidere T, Bozkurt A, Ozmenler KN, Ozsahin A, Kucuk T, Yetkin S. The influence of emotional distress on the outcome of in-vitro fertilization (IVF) and/or intracytoplasmic sperrm injection (ICSI) treatment among infertile Turkish women. Isr J Psychiatry Relat Sci. 2008;45(1):55-64.
- Kee BS, Jung BS, Lee SH. A study on pshycological strain in IVF patients. J Assist Reprod Genet. 2000;17(8):445–8.
- Kousalya K, Sanjeeva Reddy N, Uma Maheswara Reddy C, Jayashree K .Depression,anxieety and stress among infertile women and the impact of counseling on these levele. Innovative Journal of Medical and Health Science. 2013;3:110 – 112.
- Litzinger S, Gordon KC. Exploring relationships among communication, sexual satisfaction and marital satisfaction. J Sex marital. 2005;31(5):409-24.
- Lok I H, Lee DT, Cheung LP, Chung WS, Lo WK, Haines CJ. Psychiatric morbidity amongst infertile Chinese women undergoing treatment with assisted reproductive technology and the impact of treatment failure. Gynecol Obstet Invest. 2002;53(4):195–90.
- Mollaiy Nezhad M, Jaaferpour M, Jahanfar SH. Infertility related stress and marital life in Iranian infertile women who referred to Isfahan infertility treatment clinic. J Repod Infertile .2000;2:26-39.(Persian)
- Newton CR, Sherrard W, Glavac I. The Fertility Problem Inventory: measuring perceived infertility-related stress. Fertil Steril. 1999;72(1):54-62.
- Noorbala AA, Ramezanzadeh F ,Abedinia N. Study of psychiatric disorders among fertile and infertile women and some predisposing factors. Journal of Family and Reproductive Health .2007;1(1):6-11.
- Ogawa M, Takamatsu K, Horiguchi F. Evaluation of factors associated with the anxiety and depression of female infertility patients.Biopsychosocial medicine. 2011;5:15.
- Peterson B , Boivin J , Norré J, Smith C , Thorn P , Wischmann T. An introduction to infertility counseling: a guide for mental health and medical professionals. J Assist Reprod Genet. 2012; 9:243–248.
- Ramezanzadeh F, Aghssa M, Abedinia N, Zayeri F, Khanafshar N, Shariat M, Jafarabadi M. A survey of relationship between anxiety, depression and duration of infertility.BMC Women’s Health. 2004;4:9 doi:10.1186/1472-6874-4-9.
- Ramli M, Ramli R, Azantee Yazmie A, Siti Khadijah M, Yatim Hayati M, Midin M,et all. A preliminary study of the psychological differences in infertile couples and their relation to the coping styles.Holistic Psychiatry. 2014;55:565–569.
- Sadock BJ, Kaplan HI, Sadock VA. Kaplan & Sadock’s synopsis of psychiatry. 9th ed. Philadelphia: Lippincott Williams and Wilkins; 2003.p.872.
- Samari A , Lali faz A. Study of Effect Life Skill Instruction on Stress. Principal of Psychiatric Health. 2005;7(25,26):47-55.
- Sheiner E, Sheiner EK, Potashnik G, Carel R, Shoham-Vardi I: The relationship between occupational psychological stress and female fertility. Occup Med (Lond). 2003;53:265-269.
- Seible MM. Infertitility: a holistic text. 2nd ed.Ph iladelphia:Appleton & Lange;1997.p. 667-751.
- Syiem1 T, Jayashankar Reddy K. The Multifaceted Aspects of Infertility. International Journal of Science and Research (IJSR). 2013; 2(11).
- Wichman C L, Ehlers SL L,Wichman SE, Weaver A L. & Coddington Ch. Comparison of multiple psychological distress measures between men and women preparing for in vitro fertilization. Fertility and Sterility. 2011;95(2):717-721.

