
Mohammadi Mobarakeh, Mehdi and HJ Omar Abdul Hafidz
Faculty of Bioscience and Medical Engineering, Center of Sport Innovation and technology. University Technology Malaysia, Malaysia.
DOI : https://dx.doi.org/10.13005/bpj/794
Abstract
Ankle sprain is the most common injury in sport activities. When it’s happened, accurate diagnosis need to be taken care off. Failed to do it will resulted in ligaments stretched out, instability and lose balance especially in walking. This study investigated the effect of friction technique on sprained ankle (grade II). Friction is one of the most appropriate techniques in massage for removing adhesion. 24 young athletes with ankle sprain grade II were selected among 100 patients base on MRI test. Patients were divided into two groups. Experimental group received sport massage. Another group is a control group or non training group. Each group consists of 12 patients who suffered from ankle sprain grade II. The massage group received the 15 minutes effleurage and friction massages on their ankles administered by a sport rehabilitation specialist and professional massager. The control group used ankle brace. Effleurage technique have used as warming-up section. Data were analysed by using paired-t test. Findings show that treatment (massage) group has great impact (P-value <0.05) compared to control group. The implications of this study offer this protocol as a most effective treatment for ankle sprain grade II.
Keywords
Massage therapy; Friction technique; Ankle sprain
Download this article as:| Copy the following to cite this article: Mobarakeh M, Mehdi, Hafidz H. J. O. A. Effect of Friction Technique on Ankle Sprain Grade II Treatment. Biomed Pharmacol J 2015;8(2) |
| Copy the following to cite this URL: Mobarakeh M, Mehdi, Hafidz H. J. O. A. Effect of Friction Technique on Ankle Sprain Grade II Treatment. Biomed Pharmacol J 2015;8(2). Available from: http://biomedpharmajournal.org/?p=3810 |
Introduction
Sprained ankle, also known as an ankle sprain, twisted ankle, rolled ankle, ankle injury or ankle ligament injury, is a common medical condition where one or more of the ligaments of the ankle is torn or partially torn[1]. A sprain is an injury to a ligament. Ligaments are strong tissues around joints which attach bones together and give support to joints. A ligament can be injured, usually by being stretched during a sudden pull. The ligaments at the side of the ankle are the ones most commonly sprained[2]. A damaged ligament causes inflammation, swelling, and bleeding (bruising) around the affected joint. Movement of the ankle joint is painful when you have a sprained ankle[3]. Sprained ankles are the most frequent type of musculoskeletal injury seen by primary-care providers. More than 23,000 people each day in the United States require medical care for ankle sprains [4].
Ankle sprains are common sports injuries but also happen during everyday activities[5]. An unnatural twisting motion of the ankle joint can happen when the foot is planted awkwardly, when the ground is uneven, or when an unusual amount of force is applied to the joint. Sprains happen when the foot is rolled or turned beyond motions that are considered normal for the ankle. An ankle sprain usually occurs when a person lands from jumping or running onto an uneven surface. If the ankle is placed into an abnormal position at the same time, overstretching of the ligaments can occur. The ligaments of the ankle hold the ankle bones and joint in position, and therefore help to stabilize the ankle joint. They protect the ankle joint from abnormal movements-especially twisting, turning, and rolling of the foot[6].
Sport rehabilitation is an important part of treating sports injuries[7]. A rehabilitation program aims to return the injured body part to normal function by gradually introducing it to movement and exercise[8]. With most sports injuries, it helps to move the injured part as soon as possible to help speed up the healing process. Gentle exercises should help improve the area’s range of motion. As movement becomes easier and the pain decreases, stretching and strengthening exercises can be introduced. During the rehabilitation process, you should not attempt to do too much and too quickly. Start by doing frequent repetitions of a few simple exercises before gradually increasing the amount that you do[9]. Avoid painful activities and High intensity exercise until pain removed, and full strength and flexibility have returned to the injured area [10].
Some coaches and experts in rehabilitation believe that massage is very benefit for the body prior to participating in training and physical activities. More especially massage is used as pre-exercise activities to improve performance, reduce the risk of exercise and muscle damage and to sport rehabilitation programs. Massage is very good method to increase blood flow to muscles and increase muscles temperature [11], so is appropriate to rehabilitation program[12]. With use of massage also can reduce tissue adhesion and to improve muscle flexibility [13], which can help to improve injury and remove risk factors [14].
Method
In this study, effectiveness of massage therapy protocol on the patients with ankle sprain grade II was determined through the examination of ROM, strength and balance in the sprained ankle grade II. This study was conducted on 24 male athletes aged 20-25. Patients were divided to two groups including non training group (control group) and experimental group (massage group) and each group contained 12 patients. Control group or non training group no performance any training, and only used brace to fixing the joint and rest. In massage group applied effleurage massage for warm up and then used friction massage across the injured ligaments. The duration of treatment was 8 weeks for both groups. Pre test and post test have done by evaluating of ROM, strength and balance. Assessments has done by using goniometer to ROM, thera band to strength and wobble board to balance in pre test and post test phase (before and after treatment). The first test is evolution of the range of motion (ROM) test (Figure 1). Patients should do dorsiflexion, plantarflexion, inversion and eversion and assess the ROM with goniometric and record the results.
 |
Figure 1: Range of Motion (ROM) for ankle |
Second pre-test is the muscle strength test which performed utilizing the thera-band (Figure 2) and accounts the number of repeats in each direction to assess ankle strength. This test has performed with all the movements of ankle included: dorsiflexion, plantar flexion, inversion and eversion. Ask patients sit on the floor with straight leg, for dorsiflexion, anchor the band to the wall or chair and wrap it around the foot. Patient should pull his toes toward and slowly return to the start position and repeat. For plantar flexion, wrap the band around the patient foot and he should hold the end in his hands. Then ask him gently push toes and return to start position. For inversion and eversion, attach band to secure object and end to forefoot. Pull foot inward and outward and slowly return and repeat.
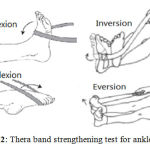 |
Figure 2: Thera band strengthening test for ankle |
Last training in pre-test is ankle balance test that performed on wobble board (Figure 3) and measurement have taken in one leg (sprained ankle) with open eyes position by calculating the time. Asked patients Stand on the balance board with knees bent slightly, feet shoulder width apart and trunk erect. Maintain this position while balancing the board, trying to keep either side from touching the ground. Then Stand on one leg in the center of the rocker or wobble board, trying to keep either side from touching the ground while maintaining erect posture.
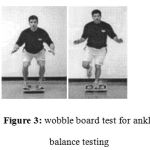 |
Figure 3: wobble board test for ankle balance testing |
Result
Effect of massage therapy on ROM
A paired-samples t-test was conducted to compare massage group and control group in 8 weeks rehabilitation program. There is a significant difference in the results of dorsiflexion in massage group (M=26.52, SD=0.29580) and control group (M=19.87, SD=0. 17645) conditions; t (11)=74.561, p = 0.000. Also result indicated that there is a significant difference in the results of plantarflexion in massage group (M=41.5000, SD=0.35675) and control group (M=36.9417, SD=0.14434) conditions; t (11)= 35.235, p = 0.000. When investigated the inversion result, There is a significant difference in the results of inversion in massage group (M=17.1833, SD=0.79411) and control group (M=13.6333, SD=0.29644) conditions; t (11)= 14.708, p = 0.000. Moreover the results shows that there is a significant difference in the results of eversion in massage group (M=14.4500, SD=0.23160) and control group (M=11.3917, SD=0.50715) conditions; t (11)= 16.810, p = 0.000. Result shows in Table (3.1). Hence, based on this finding, there is significant effect of massage therapy on improves ROM in ankle sprain grade II.
Table 3.1: Paired samples test of ROM in massage group in compared control group.
| Mean | N | Std. Deviation | Std. Error Mean | ||
| Pair 1 | post_Dorsiflexion_Massage | 26.5250 | 12 | .29580 | .08539 |
| Post_Dorsiflexion_Control | 19.8750 | 12 | .17645 | .05094 | |
| Pair 2 | Post_platarflextion_Massage | 41.5000 | 12 | .35675 | .10299 |
| Post_platarflextion_Control | 36.9417 | 12 | .14434 | .04167 | |
| Pair 3 | Post_Inversion_Massage | 17.1833 | 12 | .79411 | .22924 |
| Post_Inversion_Control | 13.6333 | 12 | .29644 | .08558 | |
| Pair 4 | Post_Eversion_Massage | 14.4500 | 12 | .23160 | .06686 |
| Post_Eversion_Control | 11.3917 | 12 | .50715 | .14640 | |
Standard mean of Dorsiflexion=24.68±3.25
Standard mean of Plantarfelxion=40.92±4.32
Standard mean of Inversion=16.29±3.88
Standard mean of Eversion=15.87±4.45
| Paired Differences | t | df | Sig. | ||||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| Pair 1 | post_Dorsiflexion_Massage Post_Dorsiflexion_Control | 6.65000 | .30896 | .08919 | 6.45370 | 6.84630 | 74.561 | 11 | .000 |
| Pair 2 | Post_platarflextion_Massage Post_platarflextion_Control | 4.55833 | .44814 | .12937 | 4.27360 | 4.84307 | 35.235 | 11 | .000 |
| Pair 3 | Post_Inversion_Massage Post_Inversion_Control | 3.55000 | .83612 | .24137 | 3.01876 | 4.08124 | 14.708 | 11 | .000 |
| Pair 4 | Post_Eversion_Massage Post_Eversion_Control | 3.05833 | .63024 | .18193 | 2.65790 | 3.45877 | 16.810 | 11 | .000 |
Effect of massage therapy on ankle strength
As can be seen in Table 3.2 a paired-samples t-test was conducted to compare massage group and control group in 8weeks rehabilitation program. There is a significant difference in the results of strength in massage group (M=11.33, SD=0 .888) and control group (M=7.58, SD=0.669) conditions; t (11)= 10.688, p = 0.000. Hence, based on this finding, there is significant effect of massage therapy on improves strength in ankle sprain grade II.
Table 3.2: Paired samples test of strength in massage group in compared control group.
| Mean | N | Std. Deviation | Std. Error Mean | ||
| Pair 1 | Pre_thera_band_Massage | 2.58 | 12 | .669 | .193 |
| pre_thera_band_Control | 2.50 | 12 | .674 | .195 | |
| Pair 2 | Post_thera_band_Massage | 11.33 | 12 | .888 | .256 |
| post_thera_band_Control | 7.58 | 12 | .669 | .193 | |
Paired Samples Test
| Paired Differences | t | df | Sig. (2-tailed) | ||||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| Pair 1 | Pre_thera_band_Massage pre_thera_band_Control | .083 | 1.165 | .336 | -.657 | .823 | .248 | 11 | .809 |
| Pair 2 | Post_thera_band_Massage post_thera_band_Control | 3.750 | 1.215 | .351 | 2.978 | 4.522 | 10.688 | 11 | .000 |
Effect of massage therapy on balance
As can be seen in Table 3.3 a paired-samples t-test was conducted to compare massage group and control group in 8weeks rehabilitation program. There is a significant difference in the results of balance in massage group (M=6.83, SD=0 .937) and control group (M=5.17, SD=0.937) conditions; t (11)= 5.863, p = 0.000. Hence, based on this finding, there is significant effect of massage therapy on improves balance in ankle sprain grade II.
Table 3.3: Paired samples test of balance in massage group in compared control group.
| Mean | N | Std. Deviation | Std. Error Mean | ||
| Pair 1 | Pre_WBSA_Massage | .75 | 12 | .754 | .218 |
| Pre_WBSA_Control | 1.00 | 12 | .739 | .213 | |
| Pair 2 | Post_WBSA_Massage | 6.83 | 12 | .937 | .271 |
| Post_WBSA_Control | 5.17 | 12 | .937 | .271 | |
|
Paired Samples Test |
|||||||||
| Paired Differences | t | df | Sig. (2-tailed) | ||||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| Pair 1 | Pre_WBSA_Massage Pre_WBSA_Control | -.250 | 1.055 | .305 | -.920 | .420 | -.821 | 11 | .429 |
| Pair 2 | Post_WBSA_Massage Post_WBSA_Control | 1.667 | .985 | .284 | 1.041 | 2.292 | 5.863 | 11 | .000 |
Finding and Discussion
Although lots of researches have been done about ankle rehabilitation, but because frequently of ankle sprain in athletes and other people and due to the importance of joint and it’s damages there is still need to do study on various rehabilitation techniques. Massage is the one of the most important rehabilitation technique that used in this study. Massage is believed to benefit athletes by enhancing performance and recovery, as well as promoting relaxation through biomechanical, physiological, neurological, and psychological mechanisms. The aim of this study was to investigate the effect of massage on the improving of balance after ankle sprain grade II rehabilitation.
Massage has highly relation with muscle and connective tissue relaxation so when muscle is relaxed is able to more stretch and result in long time will be increase in ROM[15]. Effleurage technique as a warm-up technique evokes the relaxation response and increase blood flow to muscles and ligaments. Afterward, friction technique had used to remove adhesion from injured muscle and ligament. On the other hand, massage was associated passive movement in ankle joint. Passive movement contained all directions of ankle joint including dorsiflexion, plantarflexion, inversion and eversion. Passive training help to ankle muscles and ligaments to increase ROM by creating continuous stretching. The mechanical pressure from massage is generally used to treat adherent or contracted connective tissue in order to restore fibres to a more normal alignment. The finding of study showed that massage has an excellent effect on the muscle flexibility and connective tissue that they have high relation with ROM and enhancing performance.
According to the results and statistical data analysis, massage has suitable and meaningful influence on the range of motion of injured joint and also is an optimal treatment method for the improvement and relief of sprain grade II (P-Value <0.05). Effect of massage on ROM after Dorsiflexion with the mean 26.52◦±0.29 is the greatest after combined group. Also when the effectiveness of massage on ROM after Plantarflexion evaluated, the massage therapy group with the mean 41.50◦±0.35 has the greatest value after combined group. After investigation to the effectiveness of massage therapy on ROM, result showed that massage in Inversion with the mean 17.18◦±0.79 and in Eversion with the mean 14.45◦±0.23 has a great impact to increase the ROM of ankle joint after release from ankle sprain grade II.
As biomechanical effect of massage, applying massage and mechanical pressure and stretching in tissue can be effective on decrease adhesion and stiffness and increase muscle compliance. The muscles and connective tissues are not yet at their full strength and the area remains subject to re-injury. With stretching and strength training, pain gradually subsides, while strength and range of motion increase. Strength training is essential to the full recovery of the muscles and connective tissues. Strength training should begin gently and progressively increase.
When applying massage to improves muscle strength, actually patients are benefited from both internal and external resistance provided from therapist and muscles. This means that when therapist applied force (External) patient is making the internal resistance and when patient tries to move the foot (Internal), is facing to external resistance by therapist. Due to data analysis the muscles strength in massage therapy group improved more than control group. Result showed that massage therapy group with the mean (M=11.33, SD=0 .888), the effects were significant.
The sprained ligaments lose the ability to efficiently communicate with brain. The result is decreased coordination of the ankle. On the other hand after ankle sprain, instability of ankle joint because the ligament tearing and laxity increased.
As mentioned before, massage is a very effective method to improving the muscle strength and ROM, and both have a direct relation with balance moreover mechanical pressure from massage help to remove adherent and muscle spasm in order to more normal alignment. Therefore when ROM, muscle strength and stability of ankle joint improved, consequently, balance will develop. Data analysis had showed that massage therapy can be effective on ankle sprain grade II and due to its significant effects on the factors related with ankle sprain grade II the rate of treatment increased. The results of the balance test in massage group showed that the massage treatment group had a significant difference with the control group (P-Value <0.05). Moreover in comparison of the balance time before and after massage therapy, result showed the significant effect on balance time than the control group (6.08±1.24). So massage therapy as a traditional therapy is effective method to ankle sprain rehabilitation.
As can be seen from data analysis, there is a significant difference between results of the ROM test, strength test (thera band) and balance test (WBSA) after treatment and before it. Also the rate of improving after treatment in control group is no comparable with massage group and this means that massage is a most effective rehabilitation method to improve ankle sprain grade II than the bracing and non training method.
Conclusion
Although there are a few studies on the effect of massage in ankle injuries but most of research are corroborant of effect of massage that has been used for centuries in an attempt to prevent and cure injuries [15][16][17][18]. The result of this research showed that there is a significant difference between massage therapy and bracing in treatment of ankle sprain grade II. In fact increase in ROM, muscle strength and balance in massage group was much better than the non training (bracing) group. Study show effectiveness of wobble board training in preventing functional instability, balance training in improving ankle joint proprioception and single leg standing It has been recommended to use the massage to rehabilitation protocols in ankle sprain grade II.
References
- W. Smith and S. F. Reischl, “Treatment of ankle sprains in young athletes,” Am. J. Sports Med., vol. 14, no. 6, pp. 465–471, 1986.
- Rasmussen, “Stability of the ankle joint. Analysis of the function and traumatology of the ankle ligaments.,” Acta Orthop. Scand. Suppl., vol. 211, pp. 1–75, 1984.
- T.-P. Fong, Y. Hong, L.-K. Chan, P. S.-H. Yung, and K.-M. Chan, “A systematic review on ankle injury and ankle sprain in sports,” Sport. Med., vol. 37, no. 1, pp. 73–94, 2007.
- P. Gerber, G. N. Williams, C. R. Scoville, R. A. Arciero, and D. C. Taylor, “Persistent disability associated with ankle sprains: a prospective examination of an athletic population,” Foot Ankle Int., vol. 19, no. 10, pp. 653–660, 1998.
- Moreira and F. Antunes, “Ankle sprains: from diagnosis to management. the physiatric view.,” Acta Med. Port., vol. 21, no. 3, pp. 285–292, 2008.
- W. Johnson Jr, “Ankle brace.” Google Patents, 28-Jul-1981.
- Comfort and E. Abrahamson, Sports rehabilitation and injury prevention. John Wiley & Sons, 2010.
- Shamus and J. Shamus, Sports injury: prevention & rehabilitation. McGraw-Hill Medical, 2001.
- M. Buschbacher, N. D. Prahlow, and S. J. Dave, Sports medicine and rehabilitation: a sport-specific approach. Lippincott Williams & Wilkins, 2008.
- J. Kraemer, J. A. Bush, R. U. Newton, N. D. Duncan, J. S. Volek, C. R. Denegar, P. Canavan, J. Johnston, M. Putukian, and W. J. Sebastianelli, “Influence of a compression garment on repetitive power output production before and after different types of muscle fatigue,” Res. Sport. Med. An Int. J., vol. 8, no. 2, pp. 163–184, 1998.
- Drust, G. Atkinson, W. Gregson, D. French, and D. Binningsley, “The effects of massage on intra muscular temperature in the vastus lateralis in humans.,” Int. J. Sports Med., vol. 24, no. 6, pp. 395–399, 2003.
- Robertson, J. M. Watt, and S. D. R. Galloway, “Effects of leg massage on recovery from high intensity cycling exercise,” Br. J. Sports Med., vol. 38, no. 2, pp. 173–176, 2004.
- H. O. K. CENTER, “TRADITIONAL MEDICINE,” 2000.
- W. Gleim and M. P. McHugh, “Flexibility and its effects on sports injury and performance,” Sport. Med., vol. 24, no. 5, pp. 289–299, 1997.
- L. Braverman and R. A. Schulman, “Massage techniques in rehabilitation medicine.,” Phys. Med. Rehabil. Clin. N. Am., vol. 10, no. 3, pp. 631–649, 1999.
- T. Callaghan, Principles of nuclear magnetic resonance microscopy. Oxford University Press, 1993.
- C. Goats, “Massage–the scientific basis of an ancient art: Part 2. Physiological and therapeutic effects.,” Br. J. Sports Med., vol. 28, no. 3, pp. 153–156, 1994.
- M. Tiidus, “Manual massage and recovery of muscle function following exercise: a literature review,” J. Orthop. Sport. Phys. Ther., vol. 25, no. 2, pp. 107–112, 1997.

