
Manuscript accepted on :
Published online on: 14-11-2015
Plagiarism Check: Yes
C. J Arabind1, D. Kathirvelu2
1Biomedical Engineering department, SRM University, Katankulathur, Tamil Nadu, India. 2Biomedical Engineering department, SRM University, Katankulathur, Tamil Nadu, India
DOI : https://dx.doi.org/10.13005/bpj/622
Abstract
Touch is an effortless sense that is critically important for fast and accurate interaction with our immediate surroundings. Surgeons, for procedures like palpating tissue to distinguish healthy from diseased, rely heavily on touch. In minimally invasive surgery, including robotic procedures, and remote surgery, Touch sensation is altered or completely absent. It has been observed that restoring or improving the haptic perception could have a substantial impact on the effectiveness of minimal invasive interventions. Despite persistent effort, reliable solutions for haptic feedback in robot-assisted minimally invasive surgery have yet to find their way into practice. This paper presents the development of a robotic arm, equipped with force sensors at the gripper surfaces, as well as an LVDT displacement-based sensor for tissue stiffness identification by indentation method. The proposed project provides the user with a “feel” of the tissue as well as the amount of force applied to the tissue, Thus achieving a much more precise delivery of force and an understanding of the tissue stiffness being dealt leading to a reduction in the tissue damage due to excess force, complications like internal bleeding and trauma while suturing.
Keywords
Robotic surgery; Haptic; Force feedback; Tactile; Minimally invasive surgery
Download this article as:| Copy the following to cite this article: Arabind C. J, Kathirvelu D. Implementation of Force Feedback in Robotic Surgical Systems. Biomed Pharmacol J 2015;8(1) |
| Copy the following to cite this URL: Arabind C. J, Kathirvelu D. Implementation of Force Feedback in Robotic Surgical Systems. Biomed Pharmacol J 2015;8(1). Available from: http://biomedpharmajournal.org/?p=727 |
Introduction
The 20th century witnessed a rapid growth in open surgery, performing operations that were deemed next to impossible in the earlier ages, but it came with a price, there was a significant rise in patient trauma, pain, infections and internal bleeding due to large incisions during open surgeries, In order to overcome these drawbacks 21st century came up with “minimally invasive robotic surgery” commonly known as MIRS. The market leaders in Robotic surgery Intuitive surgical’s “Davinci” Robot performed a total of 570,000 surgeries worldwide in 2014 alone1. Robotic surgery is becoming more and more widely accepted due to shorter hospital stay, less blood loss, less pain and fewer complications, including less risk of infection and Faster return to normal activities.
Robotic surgery also faces challenges which are pale in comparison to its advantages, the initial cost of the machine is significantly high, and there is a huge training period for the practitioner to get used to the machine. It has been observed that the “Davinci” Robot has not been utilizing its full potential due to the absence of haptic and kinesthetic feedback 2, 3. The inclusion of haptic and kinesthetic feedback is recommended by Davinci users for better, precise surgeries in a survey taken by FDA4. This paper presents the incorporation of a strain gage based force sensor at the gripper end surface for tactile force sensing as well as a linear variable differential transformer (LVDT) displacement-based force sensor for achieving kinesthetic feedback.
Tissue interaction feedback has been observed and proven to improve the potential of the robotic surgical systems. It aids the other sensory modules and helps in achieving a perfect sync with visual feedback, the combination of visual and force feedback results in an optimum tissue identification compared to visual or force feedback alone5. Many works has been done in achieving tactile feedback, that is, cutaneous sensing by placing sensors at the gripper surface, Also works have been done in achieving kinesthetic feedback by incorporating load cells at the joints of the robotic arm 3.
The earlier works in the topic can be classified in reference with the sensor based on the location of the sensor and the type of sensor used
Location based classification
The Placement of sensors is of great importance due to the space constraints, here the whole system is sectioned as the Gripper, articulated joints, the shaft and the joint actuation unit, Based on the placement of the sensors at any of these locations we can classify the force feedback system 6, 7
 |
Figure 1: Schematic of robotic arm |
Based on the sensor used
The feedback systems can also be classified on the basis of the type of sensor used as per6. Categorization can also be done by the type and principle used by sensors, that is Displacement based, Pressure based, Current based, Resistive/capacitive based and Optical based.
The displacement based sensors are mechanically stable and simple in calculations and are less prone to noise and errors. It closely resembles the mechanism used in the human fingers to identify the thickness of a substance. The current-based sensing method is prone to noise and hence unreliable5. The pressure based method requires that the tools are driven by pneumatic forces and hence calls for a complete reconstruction of the tool head. Resistive methods are rugged and stable though it lacks in accurate measurement of the force. Optical based sensing is expensive and works have been done for implementing it in higher end robotic equipments for needle insertion which is Magnetic resonance imaging (MRI) compatible8,9.
The maximum force that can be achieved by various surgical tools of the Davinci machine was studied and it was observed that the forces in newton (N) varies from as small as 2.26N for a double fenestrated grasper to as large as 37.7N for a Hem-o-lok clip applier which in Kilograms (Kg) translates to a range from .23Kg to 3.8Kg10. This force, clubbed with the 8mm diameter of the grasper surface far exceeds the force that the soft tissue can bear without damage, pain or even rupture as per the studies shown in11. The experimental setup on porcine tissue showed cell death, clot formation and inflammation due to the compressive forces exerted by graspers
Materials and Methods
The components in the setup comes under either one of the following two: the master controlling unit and the slave robotic gripper
The master controlling unit is the part which is at the user side and comprises mainly of the main control unit, the force actuation unit (vibration) and the variable POTS which are placed in the X,Y and the Z axes for controlling the movements of the robotic arm in the X,Y and the Z axes respectively. It is also equipped with a display for receiving the video camera input from the slave side.
The slave robotic gripper comprises mainly of the strain gage based force sensors at the gripper end as well as an LVDT displacement-based force sensor placed at the shaft for tactile and kinesthetic force sensing respectively.
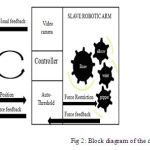 |
Figure 2: Block diagram of the complete setup |
Master control unit
The master control unit can be categorized into 3 units:
- Microcontroller– unit (Atmega162): It is an 8 bit low power microcontroller and acts as the brain of the master side. It is receives the analog variation in the variable POTS in the X, Y and Z axes through an Analog to Digital Converter hence acquiring digital values of the variation. These digital values are transmitted through wire to the slave for corresponding movements in the X, Y and Z axes. It also receives force information sensed at the slave robot.
- PWM based vibrator: This is a DC motor which is placed on the user’s forearm hence acting as the force actuation unit which gives a “feel” of the force sensed for the user. The vibration is controlled by Pulse width modulation, where in the ON/OFF cycle is controlled by the master control unit.
- Display unit: The display unit receives data from the video camera placed at the slave side for visual supervision of the operation done.
Slave robotic gripper
The slave robotic gripper is a 3 joint mechanical structure whose joints work in proportion with the variable POTS at the master side, hence achieving an ergonomic, well coordinated movement of the robotic gripper. There are mainly 2 sensors which are of prime importance in the slave side, they are:
- Strain gage based force sensor at the gripper end surface
- Displacement based force sensor placed at the shaft of the robotic arm
The strain gage based force sensing is for tactile or cutaneous feedback where as the displacement-based force sensor is for kinesthetic or force sensing so that tissue identification can be achieved.
The purpose of achieving tactile as well as the kinesthetic forces is to give an idea to the practitioner on how much force he is applying and on what kind of tissue he is applying it on. The force hence sensed is fed back into the master controller which then, based on certain thresholds generate corresponding vibration, that is, greater the force applied greater the vibration. The vibration varies from a simple touch to maximum pressure that can be applied. The following principles are used for force sensing.
Strain gage based force sensing
The strain gage based force sensor is placed at the gripping surface of the robotic gripper, this act as the tactile sensor. The sensor used is Flexiforce A201 sensor (Tekscan).
 |
Figure 3: Flexiforce sensor |
Table 1: Flexiforce sensor specification
| Model | Specifications | ||
| Length(mm) | Sensing area(mm2) | STD. Force sensed (N) | |
| A201 | 50 | 9.53 | 111 |
The corresponding circuitry for sensing comprises of a voltage divider whose unknown resistance is replaced by the flexi force sensor. Thus on application of even the slightest force on the sensor. The strain causes variation in resistance and hence a deflection and hence a proportional voltage to the strain sensed can be achieved.
The sensed voltage is now given to a 10 bit Analog to digital converter thus digitizing the full range of 111N into a resolution of 1024 hence sense as small as .108N, this digitized value is now fed to the Microcontroller unit for further usage of the sensed values.
Displacement based force sensing
The displacement-based force sensor is placed at the shaft of the robotic gripper and the gripper movement is translated to the LVDT head for corresponding movement. The movement of the head will be corresponding to the thickness of the tissue on which pressure is applied. This principle is used for tissue identification. The LVDT sensor used is “Slimline-010AM” (Roorkee, AG Measurmatics Pvt. Ltd.)
The force translation from the gripper movements to the LVDT gives the gripper movement to the force received and determines the displacement restriction of the LVDT head hence forming a relation with the thickness of the tissue.
Results and Discussion
Tactile sensation has been achieved with proportional vibration allowing the user to reduce the excess pressure applied to objects; it was found that the combination of visual and force feedback gave optimum force application for simple gripping procedures. The differentiation of objects as HARD and SOFT objects also helps to identify how much force to be applied without causing damage to the tissue. The correlation of the displacement after coming in contact with the object has given a platform for successful identification of object and classifying it as either “hard” or “soft”. Identification of hardness of the object in question has been done on some common objects and as a result common objects such as wood or high density plastics were identified as hard, where as the soft objects such as cotton and cloth has been identified successfully as soft objects.
The 21st century is the century for minimally invasive robotic surgery, the present condition of which limits its operation to a limited number of procedures; it is yet to achieve a full conversion of open surgeries into robotic surgeries because of the limitations of being a robot. Hence persistent works have been done in trying to humanize the robot. The proposed paper presents a method in achieving tactile and kinesthetic feedback to the robotic surgical units indirectly giving the user a “feel” of what the robot is in contact with, This will greatly improve the capability of robotic surgical units and hence a step towards total conversion of open surgeries to minimally invasive robotic surgery, thus significantly improving patient comfort and post operative conditions.
The data from the strain gage force sensor at the gripper surface and the displacement-based force sensor at the shaft can be used for training an artificial neural network for creating an intelligent, automated surgical machine which can greatly reduce the complicated decision making burden experienced by the surgeons. Better, stable and more miniature type sensors can be used for more precise force sensing.
Reference
- Nicholas Baer “A Post-renaissance Da Vinci: What 2015 holds for robotic surgery” internet: http://www.advisory.com/research/marketing-and-planning-leadership-council/the-growth-channel/2015/03/a-post-renaissance-da-vinci [March 3,2015]
- M. Okamura, “Haptic Feedback in Robot-Assisted Minimally Invasive Surgery,” Current Opinion in Urology, vol. 19, no. 1,pp. 102-107, 2009.
- Ali Talasaz, Rajni V. Patel, “Integration Of Force Reflection With Tactile Sensing For Minimally Invasive Robotics-Assisted Tumor Localization”, Ieee Transactions On Haptics, Vol. 6, No. 2, April-June 2013.
- FDA report “MedSun Survey Report: da Vinci Surgical System” Internet: http://www.fda.gov/downloads/MedicalDevices/ProductsandMedicalProcedures/SurgeryandLifeSupport/ComputerAssistedRoboticSurgicalSystems/UCM374095.pdf [November 11, 2013]
- Mohamed Guiatni, Vincent Riboulet, Christian Duriez, Abderrahmane Kheddar, St´Ephane Cotin,” A Combined Force And Thermal Feedback Interface For Minimally Invasive Procedures Simulation”Ieee/Asme Transactions On Mechatronics, Vol. 18, No. 3, June 2013.
- Shweta gupta “Application of biomedical engineering in force and tactile sensing in robotic MIS” internet: http://bme240.eng.uci.edu/students/10s/sgupta1/References.html December, 2008.
- Duck Hee Lee ,Seung Joon Song,Reza Fazel-Rezai, Jaesoon Choi, “The Preliminary Results Of A Force Feedback Control For Sensorized Medical Robotics“(Ijarai) International Journal Of Advanced Research In Artificial Intelligence, Vol. 2, No.5, 2013 .
- Weijian Shang, Hao Su, Gang Li, and Gregory S. Fischer, “Tele-operation System with Hybrid Pneumatic-Piezoelectric Actuation for MRI-Guided Needle Insertion with Haptic Feedback” International Conference on Intelligent Robots and Systems (IROS)November 3-7. IEEE-2013.
- Roozbeh Ahmadi, Muthukumaran Packirisamy, Javad Dargah, Renzo Cecere, “Discretely Loaded Beam-Type Optical Fiber Tactile Sensor For Tissue Manipulation And Palpation In Minimally Invasive Robotic Surgery” Ieee Sensors Journal, Vol. 12, No. 1, January 2012.
- Phillip Mucksavage, David C. Kerbl, Donald L. Pick, Jason Y. Lee, Elspeth M. McDougall, and Michael K. Louie “Differences in Grip Forces Among Various Robotic Instruments and da Vinci Surgical Platforms” Journal Of Endourology Volume 25, Number 3, March 2011.
- Smita De, Jacob Rosen, Aylon Dagan, Paul Swanson, Mika Sinanan, and Blake Hannaford “Assessment of Tissue Damage due to Mechanical Stresses” University of Washington, Technical report, July, 2006.
- Ouis B. Kratchman, Daniel Schurzig, Theodore R. Mcrackan, Ramya Balachandran, Jack H. Noble, Robert J. Webster Iii, Robert F. Labadie,“A Manually Operated, Advance Off-Stylet Insertion Tool For Minimally Invasive Cochlear Implantation Surgery” Ieee Transactions On Biomedical Engineering, Vol. 59, No. 10, October 2012
- Vera Z. Pérez, Manuel J. Betancur, Jose R. Martínez, Olga P. Torres, John Bustamante, “Force Feedback Algorithms For Master Slave Surgical Systems” Ieee Conference Paper.
- Pinyo Puangmali, Hongbin Liu, Lakmal D. Seneviratne, “Miniature 3-Axis Distal Force Sensor For Minimally Invasive Surgical Palpation” Ieee/Asme Transactions On Mechatronics, Vol. 17, No. 4, August 2012.
- Tamás Haidegger, Balázs Benyó, Levente Kovács, Zoltán Benyó, “Force Sensing And Force Control For Surgical Robot” Proceedings Of The 7th Ifac Symposium On Modelling And Control In Biomedical Systems, Aalborg, Denmark, August 12 – 14, 2009.
- Nabil Zemiti, Guillaume Morel, Tobias Ortmaier, And Nicolas Bonnet,“Mechatronic Design Of A New Robot For Force Control In Minimally Invasive Surgery” Ieee/Asme Transactions On Mechatronics, Vol. 12, No. 2, April 2007 143.

