
Soheila Nikakhlagh1, Nader Saki1, Majid Karimi2 , Saeed Mirahmadi2, Mohammad Reza Rostami2
1Associated professor of otolaryngology, Head and neck surgery, Hearing and Speech Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran 2Audiologist, Apadana clinical research center
Abstract
Loudness perception plays pivotal role in speech perception. Intensity-difference limen (IDL) is the best index of loudness perception ability. This study aimed to compare loudness perception performance of subjects who wear cochlear implant and normal-hearing listeners at frequencies of 500, 1000, 2000 and 4000 Hz. In this cross sectional study, IDL was performed on nine postlingually cochlear implanted patients with mean age of 31.77±6.6 and 17 controls with mean age of 32.76±6.5 years. Following a training period (eight sessions on the average), the cochlear implant users were re-evaluated by the same test. Data were analyzed with statistical package of SPSS (version 18) using independent and paired t-test assessments. In the initial tests, intensity-difference limens of cochlear implant users was significantly poor when compared with that of normal-hearing controls at all test frequencies (p<0.05). The mean IDL of cochlear implant users after training period, was significantly improved (p<0.05). The results demonstrated that patients with cochlear implant have some ability of loudness perception that can be significantly improved through regular training.
Keywords
Cochlear Implant; Loudness Perception; Intensity- Difference limen
Download this article as:| Copy the following to cite this article: Nikakhlagh S, Saki N, Karimi M, Mirahmadi S, Rostami M. R. Evaluation of Loudness Perception Performance in Cochlear Implant Users. Biomed Pharmacol J 2015;8(March Spl Edition) |
| Copy the following to cite this URL: Nikakhlagh S, Saki N, Karimi M, Mirahmadi S, Rostami M. R. Evaluation of Loudness Perception Performance in Cochlear Implant Users. Biomed Pharmacol J 2015;8(March Spl Edition). Available from: http://biomedpharmajournal.org/?p=2280> |
Introduction
Auditory perception is the subtle chain of events involving transduction of acoustical stimuli into electrical signals in the inner ear, transmission of electrical signals through peripheral nervous system and finally processing and interpreting them in central nervous system. Any problem in this process is strongly affected on auditory perception (1-2). The role of peripheral and central auditory disorders in perceptual consequences has been studied extensively. For example, damage to the inner ear or auditory nerve leads to the increase hearing threshold and also abnormal intensity, frequency and temporal processing (3-4) and damage to the central nervous system leads to complex processing deficits in speech perception and speech recognition (5-6).
Loudness perception is a key factor in speech perception. Intensity information is important to understand of many aspects of auditory perception including the estimation of motion and radial displacement of an audio source or perception of prosodic features of message (7).
Psychoacoustic is the study of human subjective perception of the sounds (8). The intensity is often a key feature of sounds that study in Psychoacoustic. Intensity-difference limen (IDL) is the best index of loudness perception ability. The lowest level of difference between two sounds that can be detected by the ear is called intensity discrimination. Intensity-difference limen less affected by frequency and intensity of stimulation in compared to difference limen for frequency (9-10).
Intensity-difference limen represents the accurate representation of intensity of acoustic stimuli in the auditory system. In other words, the ability to differentiate intensity within the normal range indicates decoding of data on the intensity in the auditory system has the highest accuracy (8). Many researchers study these parameters in normal population and different pathologic conditions. He et al (1998) studied intensity-difference limen on 13 young people and 13 older adults with normal hearing. They concluded that older adults have less able to differentiate intensity in compared to young people (11).
The peripheral auditory system is the main way of transferring information. Interfere at this level may have a major effect on the auditory processing abilities. Since the peripheral part of the auditory system was compensated by cochlear implantation. Therefore the aim of this study was to compare loudness perception performance of subjects who wear cochlear implant and normal-hearing listeners by using IDL test at frequency of 500, 1000, 2000 and 4000 Hz.
Materials and Methods
This cross sectional study was conducted on nine postlingually cochlear implanted patients with mean age of 31.77 ± 6.6 years and 17 individuals with normal hearing (audiometric thresholds of 20 dB HL or better at octave frequencies between 250 and 8000 Hz) as controls with mean age of 32.76±6.5 years at Khuzestan cochlear implant center (Khuzestan, Iran), speech and hearing research center of Ahvaz Jundishapur University of Medical Sciences. The entire cochlear implanted group was fitted with the Advance Bionic device.
All subjects were informed about the nature and purpose of the study before consenting to participate. Then IDL test at frequencies of 500, 1000, 2000 and 4000 Hz was performed for both normal and cochlear implanted users. In this study, IDLs were performed, using the device AC 40 audiometer (Interacoustics, Denmark) in soundproof booth. All stimuli were presented in the sound field. A short practice trial was performed before each test session.
In IDL test a pure tone with frequency of 1000 Hz was presented by changes in intensity in term of percentage. The subjects were asked to pay attention to the stimulus. If the sound is heard as a uniform then percentage change in intensity was increased until the person hears the pulsating sound. If the sound is heard as a pulsatile then percentage change in intensity was reduced until the person hears the sound uniformly. Minimum percentage change in intensity that would be necessary that person hears the pulsating sound was considered as IDL. This procedure was repeated for other frequencies.
Following a training period (eight sessions on the average), the cochlear implant users were re-evaluated by the same test. Data were analyzed with statistical package of SPSS (version 18) using independent and paired t-test assessments
Results
Patient characteristics are shown in Table 1. The Intensity-difference limens in normal subjects and patients with cochlear implant in initial test are presented in Figures 1, 2.
Table 1: Characteristics of the patients
| Device Type | Age | Implanted ear | No. |
| Advance Bionic | 23 | Right | 1 |
| Advance Bionic | 25 | Right | 2 |
| Advance Bionic | 31 | Left | 3 |
| Advance Bionic | 43 | Right | 4 |
| Advance Bionic | 29 | Right | 5 |
| Advance Bionic | 36 | Right | 6 |
| Advance Bionic | 27 | Left | 7 |
| Advance Bionic | 33 | Right | 8 |
| Advance Bionic | 39 | Right | 9 |
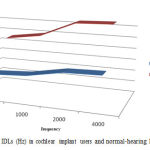 |
Figure 1: IDLs (Hz) in cochlear implant users and normal-hearing listeners |
Figure 2 shows the values of intensity discrimination in cochlear implant patients in initial test and post- training tests.
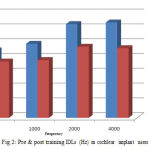 |
Figure 2: Pre and post training IDLs (Hz) in cochlear implant users |
Statistical analyses showed that in the initial test, intensity-difference limen of cochlear implant users was significantly poor when compared with that of normal-hearing controls at all test frequencies (p<0.05). The mean IDL of cochlear implant users after training period, was significantly improved (p<0.05).
Discussion
The aim of this study was to compare loudness perception performance of subjects who wear cochlear implant and normal-hearing listeners at frequency by using IDL test. We found that cochlear implant users in our study did not discriminate sound intensity as well as normally hearing individuals. The results from this study showed that cochlear implant users somewhat were able to discriminate between different pure tone intensities and this ability may be improved by regular training.
The present study has shown that there is a significant difference between IDLs of controls and cochlear implant users at all tests frequencies. These findings are in accordance with the results of other studies such as the study conducted by Cheryl et al (2005). Upon the obtained results, we observed larger IDLs in cochlear implant users.
In normally hearing individuals, varying firing rate of hair cells of the cochlea due to an increase or decrease in levels allows for the cochleotopic coding of intensities (12,13,14,15,16). The auditory pathway preserves this orderly intensity scale. Cochlear implants, however, bypass the cochlea and electrically stimulate auditory nerve fibers directly. Thus, cochlear implant users must rely on computerized processing strategies to encode sound, which may be insufficient (17,18). Furthermore, cochlear implants encode sound based primarily on place pattern and are limited by the number of channels available. In cochlear implants users a number of factors have been shown to affect intensity such as electrode configuration (19), proximity to the modiolus (20), and electrode position (21). It has also been found that characteristics of the stimulus or complexity of the stimulus can affect discrimination. Wojtczak, et al (2003) observed smaller DLs for increments applied to continuous carriers relative to those of gated carriers for some subjects and level conditions (13). These factors, combined with spiral ganglion cell degeneration resulting from auditory deprivation and the possibility of electrode insertion trauma may explain the poorer performance by cochlear implant users in the present study.
Conclusion
The results from this study showed that cochlear implant users have some ability of loudness perception, and this ability may be improved by regular training.
References
- Katz J, Burkard R, Hood L. Handbook of clinical Audiology. sixth ed. Baltimore: 2009.
- Musiek FE, Chermak G. Handbook of (central) Auditory Processing Disorder. 1th; Plural Publishing: 2007
- Buss E, Hall Jr, Grose J, Hatch D. Perceptual consequences of peripheral hearing loss: do edge effects exist for abrupt cochlear lesions?. Hearing research. 1998; 125(1):98-108.
- Gelfand SA. Meassurment principles and the nature of hearing. In: Gelfand SA. Essentials of Audiology. 2th New York : Thieme: 2001; pp 91-118.
- Zeng F-G, Kong Y-Y, Michalewski HJ, Starr A. Perceptual consequences of disrupted auditory nerve activity. Journal of Neurophysiology. 2005; 93(6):3050-3063.
- Zeng F-G, Oba S, Starr A. Supra threshold processing deficits due to desynchronous neural activities in auditory neuropathy Neuroreport16 (1999): 3429-3435.
- Kidd G.Jr. Psychoacoustics. In: Katz J, Burkard R.F, Medwestsky L. Handbook of clinical audiology. 5th Baltimore: Lippincott Williams and Wilkins: 2002; 33-49.
- Allen P. Acoustics and psychoacoustics. In: Roeser R.J, Valente M, Hosford-Dunn H. Audiology Diagnosis. 1th New York: Thieme Medical Publisher Inc: 2000; 153-180.
- Cranford JL, Stream RW. Discrimination of short duration tones by elderly subjects. Journal of gerontology. 1991; 46(1):37-41.
- Marvit p, Florentine M,Buss S.A comparison of psychophysical procedures for level-discrimination thresholds. J. Acoust. Soc. Am. 2003; 113:33-048
- He N-j, Dubno JR, Mills JH. Frequency and intensity discrimination measured in a maximum-likelihood procedure from young and aged normal-hearing subjects. The Journal of the Acoustical Society of America. 1998; 103(1):553-565.
- Bryan E, Pfingst P, atricia A, Burnetta, Dwight S. Intensity discrimination with cochlear implants. J. Acoust. Soc. Am. 1982; 74(4): 1283-92.
- GALVIN JJ, FU QJ. Effects of Stimulation Rate, Mode and Level on ModulationDetection by Cochlear Implant Users. JARO 2005:6: 269–279
- Mojtczak M, Donaldson GS, Viemeister NF. Intensity discrimination and increment detection in cochlear-implant users J. Acoust. Soc. Am. 2003; 114:396-405.
- Stéphane G, Christophe M. Intensity discrimination and auditory brainstem responses in cochlear implant and normal-hearing listeners. Behavioral Neuroscience. 1998; 112(4): 793-799.
- Rogers CF, Healy EW, Montgomery AA. Sensitivity to isolated and concurrent intensity and fundamental frequency increments by cochlear implant users under natural listening conditionsa. J. Acoust. Soc. Am. 2006; 119(4): 2276-2287
- Shannon RV. Temporal modulation transfer functions in patients with cochlear implants. J Acoust Soc Am 1992; 91:2156-2164,.
- Alipour A. the reliability and validity of chapman’s handness inventory in junior high school students. iranian journal of psychologists. 1385;7(2):197-205.
- Drennen, WR, Pfingst BE. Current-level discrimination using bipolar and monopolar electrode configurations in cochlear implants, Hear. Res. 2005; 202, 170–179.
- Cohen LT, Saunders E, Clark GM. Psychophysics of a prototype perimodiolar cochlear implant electrode array, Hear. Res. 2001; 155, 63–81.
- Nelson DA, Schmitz JL, Donaldson GS, Viemeister NF, Javel E. Intensity discrimination as a function of stimulus level with electric stimulation. J. Acoust. Soc. Am. 1996; 100, 2393–2414.

